Metabolic dysfunction associated fatty liver disease (MAFLD) is a disorder characterized by the accumulation of fat in the hepatic parenchyma that can evolve from simple steatosis to non-alcoholic steatohepatitis (NASH) via scarred tissue and inflammation combined with metabolic abnormalities (Chalasani et al., 2012). The prevalence of MAFLD is rapidly increasing worldwide, in parallel to the epidemics of diabetes and obesity, as well as the burdens of the disease, which include both cardiovascular and liver-related complications such as cirrhosis and cancer (Gill and Majumdar, 2020; Maurice and Manousou, 2018). While clinical suspicion and management of non-severe cases is largely based in non-invasive tests such as vibration-controlled transient elastography (VCTE) (Tapper and Afdhal, 2015), certain serum biomarkers (Goyale et al., 2021) and imaging including abdominal ultrasound, magnetic resonance imaging (MRI) and computed tomography (CT) (Vernuccio et al., 2021; Zhang et al., 2018), liver biopsy remains the gold standard for MAFLD diagnosis.
VCTE is a non-invasive method that provides semi-quantitative information on the accumulation of fat in the liver via the controlled attenuation parameter (CAP) (Tapper and Afdhal, 2015). This assessment is performed only at a whole organ scale and with decreased reliability for patients with obesity, who commonly have MAFLD (Berzigotti et al., 2021), whereas MRI and CT are voxel-specific imaging techniques that allow precise region assessment via image segmentation. Despite being defined as the go-to mode for quantification via proton density fat fraction measures (Hernando et al., 2008; Reeder et al., 2007; Triay Bagur et al., 2019; Vilgrain et al., 2013), MRI is time-consuming, expensive, and not available or extremely busy in most healthcare centers, which makes it a less used protocol in routine clinical practice (Ricci et al., 1997; Roldan-Valadez et al., 2008). Thus, medical institutions could miss out on affected patients. Furthermore, MRI can be contraindicated in patients with metal implants or pacemakers. In addition, the reliability of the quantified fat on patients with hepatocyte dysfunction may be compromised.
Conversely, CT imaging is more available, cheaper, non-time consuming and a widely used modality for diagnosis of multiple pathologies. Thus, CT-based fat quantification algorithms open the door to detection of hepatic steatosis in adult patients that have been evaluated for other medical purposes where CT imaging is routinely acquired, as a screening tool. This is supported by findings suggesting that MAFLD coexists with multiple extrahepatic pathologies that are evaluated using abdominal or chest CT scans in routine clinical practice (Kaya and Yilmaz, 2022; Pipitone et al., 2023). This could prevent them from exposure to developing complications born from liver affectations (Vernuccio et al., 2021).
CT-based assessment of fat in liver tissue relies on radiodensity values of the liver. Steatosis of such organ is detected by parenchyma hypoattenuation in CT (Kodama et al., 2012). Nevertheless, more powerful radiodensity-based benchmarks relating the liver and the spleen have been broadly and consistently defined for NCE-CT images (Boyce et al., 2010; Hamer et al., 2005), whereas the analogous standards used in CE-CTs have been discussed in the literature with many divergent proposals and a diminished potential due to the contrast agent effect on tissue attenuation (Jacobs et al., 1998; Kim et al., 2010; Lee and Park, 2014). However, one of the current pitfalls of using attenuation as reference information in NCE-CT lies in the fact that other pathologies, such as hepatocellular carcinoma and vascular conditions, may appear with variable intensities that could be mistakenly contemplated as MAFLD, whereas under contrast agent injection they appear hyperattenuated instead (Hamer et al., 2006).
Furthermore, the established segmentation approach relies on manually drawing regions of interest (ROI) in the right lobe of the hepatic parenchyma and inside the spleen and therefore depends on the user who analyzes the image (Hamer et al., 2006; Li et al., 2018; Zeb et al., 2012). Since the organs display different radiodensity values depending on the area that is being segmented, using this method is subject to inter-user variability and therefore has a diminished robustness that exhibits the necessity of developing automatic and user independent methods to solve the aforementioned issues.
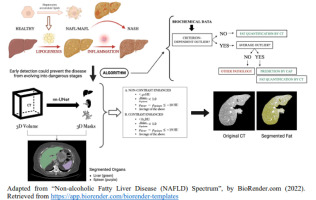
Prior studies have addressed the problem using methods based on algorithms that either quantify a portion of the liver, analyze it at a global organ scale, or use limited radiodensity thresholds (Graffy et al., 2019; Jirapatnakul et al., 2020; Pickhardt et al., 2021; Zhang et al., 2022), which has associated limitations such as missing out on region-specific information and susceptibility to radiological changes, respectively. Therefore, the aim of the present study was to develop a new fully automatized method inspired by an algorithm for quantifying the percentage of fat in the liver based on a CT voxel analysis independently of contrast agent. In particular, we addressed non-invasiveness, global and region-specific hepatic fat accumulation, reduced costs and time consumption, objectivity, and automaticity as the main goals of the presented tool. We focused on developing an automatic algorithm that contemplates radiodensity-based criteria including absolute liver threshold, liver-to-spleen ratio, and liver-minus-spleen difference to include or discard voxels as contributors to steatosis. VCTE is a widely used technique for qualitative evaluation MAFLD on medical centers (Siddiqui et al., 2019), for which we used it as reference data when comparing with estimated percentage of fat in the liver. Namely, the fit aimed at a proportional relationship between CAP values and computed percentage fat in the liver for prior validation of the established benchmarks for both CE- and NCE-CT. The algorithm adapted the criteria according to the presence or absence of a contrast agent to increase the utility of the tool for future usage in clinical routines involving any type of CT imaging.










留言 (0)