SCC of the lip is a relatively common epithelial malignancy in sub-Saharan Africa with significant morbidity and mortality [22]. While known risk factors such as tobacco use, alcohol, ultraviolet light, and fair skin have been identified, there still exists a gap in our understanding of the disease’s etiopathogenesis [3, 4]. The role of HR-HPV in SCC of the lip has been a subject of investigation. A few studies (Table 1) have researched the role of HR-HPV in SCC of the lip and many with small sample sizes (some with a combination of SCC from the lip and other parts of the oral cavity) and utilizing single testing methodologies, predominantly HPV DNA PCR [12, 15,16,17,18]. The purposes of the present study were (1) to determine the prevalence of HR-HPV in a series of lip SCC from South African patients, using currently accepted HPV-testing methodologies (p16 IHC, PCR-based HPV-typing and mRNA PCR in a subset) and (2) to define the clinical and histomorphologic features of HPV-associated lip SCC, which may provide new insights into the development of these lesions.
To the best of our knowledge, our study is the first to use a multimodal testing approach, and the first to examine the incidence of HR-HPV in lip SCC using mRNA PCR technology. Using this approach, we were able to establish the presence of HR-HPV in 2% of the lip SCC.
In general, DNA PCR-based studies have reported a higher prevalence of HR-HPV in SCC of the lip. Mitsuishi et al. reported a prevalence rate of 100% using DNA PCR to detect HR-HPV in a small sample of 5 lip verrucous carcinomas, 3 of which harbored HPV-18 [17]. However, PCR detection alone does not distinguish HPV infections that are transcriptionally active from those that are not (i.e., so-called “passenger” HPV). Of the five HR-HPV DNA-positive SCC in the present study, only one was positive for p16 and mRNA PCR. In addition, HR-HPV DNA was detected in 8% of the control cases, which is just below the frequency of 10% observed in lip SCC. The latter finding clearly suggests that HR-HPV DNA detection alone is of limited value to confirm HPV-positive lip SCC.
p16 immunohistochemistry is easily accessible and affordable [23] and is recommended by the College of American Pathologists (CAP) as a reliable test for HR-HPV in OPSCC [20]. Transcriptionally active HR-HPV infection in OPSCC is typically correlated with p16 protein overexpression [20]. In an Egyptian study, Tealab et al. using p16 IHC demonstrated a high prevalence of HR-HPV in lip SCC (48%) [16].
Although the sensitivity of p16 IHC for HR-HPV infection is high, approaching 100%, its specificity is only 80–90%, as mechanisms other than pRb inactivation (e.g., pRb mutation) may lead to p16 overexpression [24]. In addition, while the concordance rate between p16 overexpression and molecularly confirmed HR-HPV infection is approximately 92–100% in OPSCC in the western world [25, 26], the concordance rates are significantly lower (32%), in regions with lower prevalence of HR-HPV-associated OPSCC, such as South Africa [27]. Therefore, p16 is not a perfect stand-alone surrogate marker for HR-HPV infection, especially in sub-Saharan Africa, where a low prevalence rate of HPV-associated OPSCC has been documented [27]. Similarly, of the 11 p16-positive lip SCC in our study (22%), only one case demonstrated mRNA positivity, resulting in a low p16 positive predictive value of 9% (sensitivity = 100 and specificity = 83%). Our results show that the combination of DNA PCR and p16 IHC appears to correlate with the presence of transcriptionally active virus (Table 3). A large meta-analysis showed a high sensitivity and specificity when both p16 IHC and HPV DNA PCR were utilized to detect transcriptionally active HPV infection in OPSCC [14].
Although HPV E6/E7 mRNA detection is the gold standard for identifying HR-HPV infection [14], the test is not widely available in developing countries due to technical and financial constraints. Similarly, to minimize study costs and based on p16’s outstanding negative predictive value (with p16 sensitivity approaching 100%) [24], we opted to evaluate the expression of HPV-16 and HPV-18 mRNA transcripts only in p16-equivocal/positive and HPV DNA PCR-positive lip SCC. Thus, the two p16-negative/HPV DNA PCR-positive lip SCC most likely represent passenger- and not truly active infections.
In fact, for pathology laboratories across sub-Saharan Africa, we recommend initial screening of lip SCC with p16 IHC complemented by HPV DNA PCR in p16-positive cases. Nevertheless, as clearly demonstrated in our study, mRNA ISH/PCR tests are best reserved for lip SCC with equivocal p16 IHC (Table 3).
Several factors may contribute to the lower HR-HPV prevalence in our study. This includes an increase in the prevalence of other risk factors in the population, such as tobacco and alcohol use, the African sun or regional sexual practices with a low prevalence of oral-genital sexual intercourse, leading to decreased exposure to HR-HPV in the oral cavity [28]. Additionally, genetic protective factors may play a role, as observed in cervical cancer [28].
According to the Joint United Nations Program on HIV/AIDS (UNAIDS), South Africa has one of the highest HIV prevalence rates, with a prevalence of 20.4% [29]. HIV infection has been linked to an increase in head and neck cancers. Beachler et al. reported an increase in HNSCC in HPV (oropharyngeal) and non-HPV (non-oropharyngeal locations, including the lip)-related sites in HIV-positive individuals compared to the general population [30]. Similarly, studies conducted in America and Netherlands have demonstrated a higher prevalence of HPV infection in HIV-positive individuals than in HIV-negative individuals [31, 32].
Despite the high HIV prevalence in certain regions in Africa, studies have revealed a lower-than-expected prevalence of HR-HPV in head and neck cancers, implying the involvement of multiple factors in the development of head and neck cancer in this area [27, 33]. In fact, none of the three SCC from HIV-positive patients in the present study were HR-HPV positive.
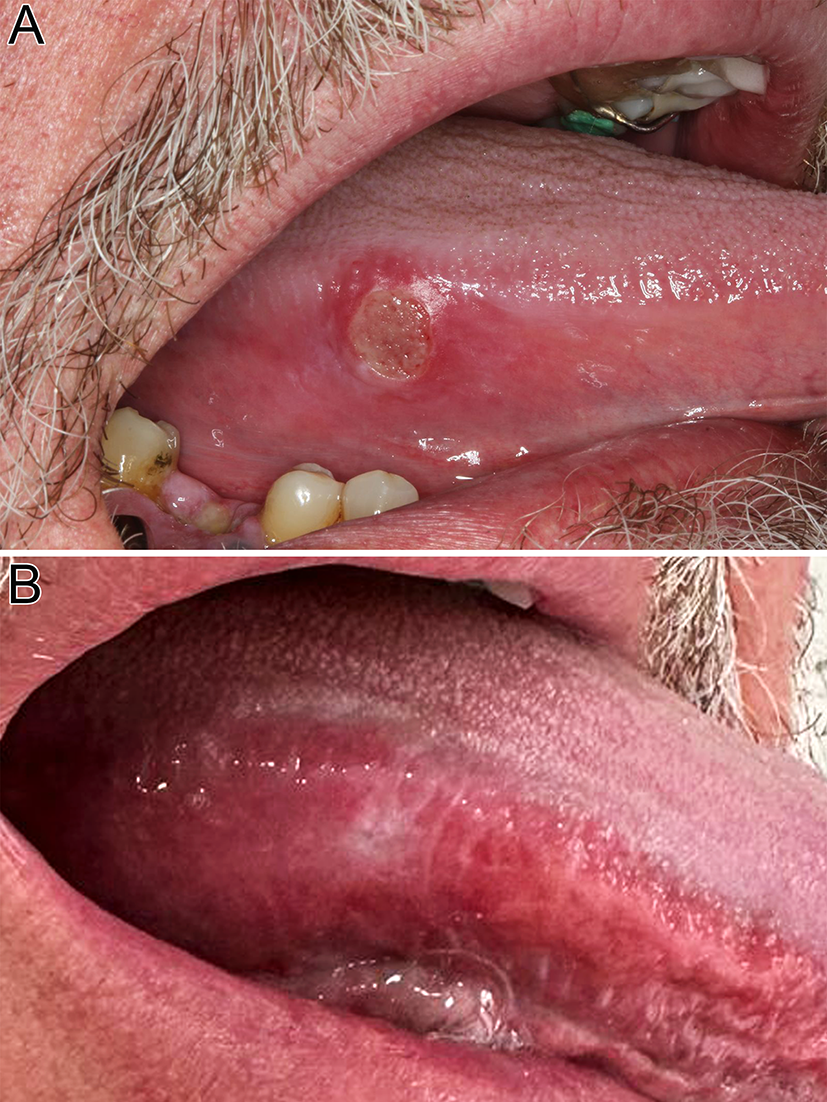
Numerous studies have consistently demonstrated a strong association between HR-HPV and non-keratinizing histomorphology in OPSCC [8, 9]. Similar to HPV-associated OPSCC, the only HR-HPV-positive lip SCC in our study showed a non-keratinizing morphology.
Most of the p16-positive lip SCC in our study arose from the vermillion border of the lower lip, a transition from highly keratinized external skin to less keratinized internal skin. Given that the majority of HPV-associated squamous lesions of the uterine cervix occur at the ecto-endocervical transition zone, it is tempting to speculate that the vermillion border of the lower lip might bear some analogy to the latter. However, an exact site for the only HR-HPV-positive case in our study could not be determined.
The strength of our study lies in the fact that, it is the first prevalence study using multiple HPV-testing modalities, including mRNA PCR in lip SCC. However, a notable limitation is the retrospective nature of the study with limited information on participant risk factors.






留言 (0)