We presented the management of two cases of general anesthesia for cesarean sections in parturients with aortic root dilation exceeding 45 mm. These cases offer numerous clinical points for discussion, some of these will be addressed below.
Despite thoracic aortic aneurysms have an incidence of approximately 6 per 100,000 patient/year [4], the occurrence of ascending aortic aneurysm dissection in pregnant patients is exceedingly rare, accounting for only 0.0004% of all pregnancies [5]. Even though life-threatening complications are rare, around half of all aortic complications in women younger than 40 years of age are associated with pregnancy [5, 6].
Indeed, hemodynamic and hormonal changes during pregnancy contribute to the increased risk of aortic aneurysm [7], with alterations in the cardiovascular system including increased cardiac output (50%), increased heart-rate (10–20 beats/min), and elevated circulating volume and left ventricular mass. Additionally, the aorto-caval compression from the growing fetus raises resistance to aortic outflow, potentially exacerbating the risk of aortic aneurysm dissection and rupture. At the same time, elevated levels of estrogen and progesterone alter the structure of media and intima layers, leading to weakening of the aortic wall [7, 8] These hemodynamic changes peak during the third trimester, coinciding with a significant portion of aortic dissections occurring during pregnancy, with 33% happening in the peri-partal period [8, 9].
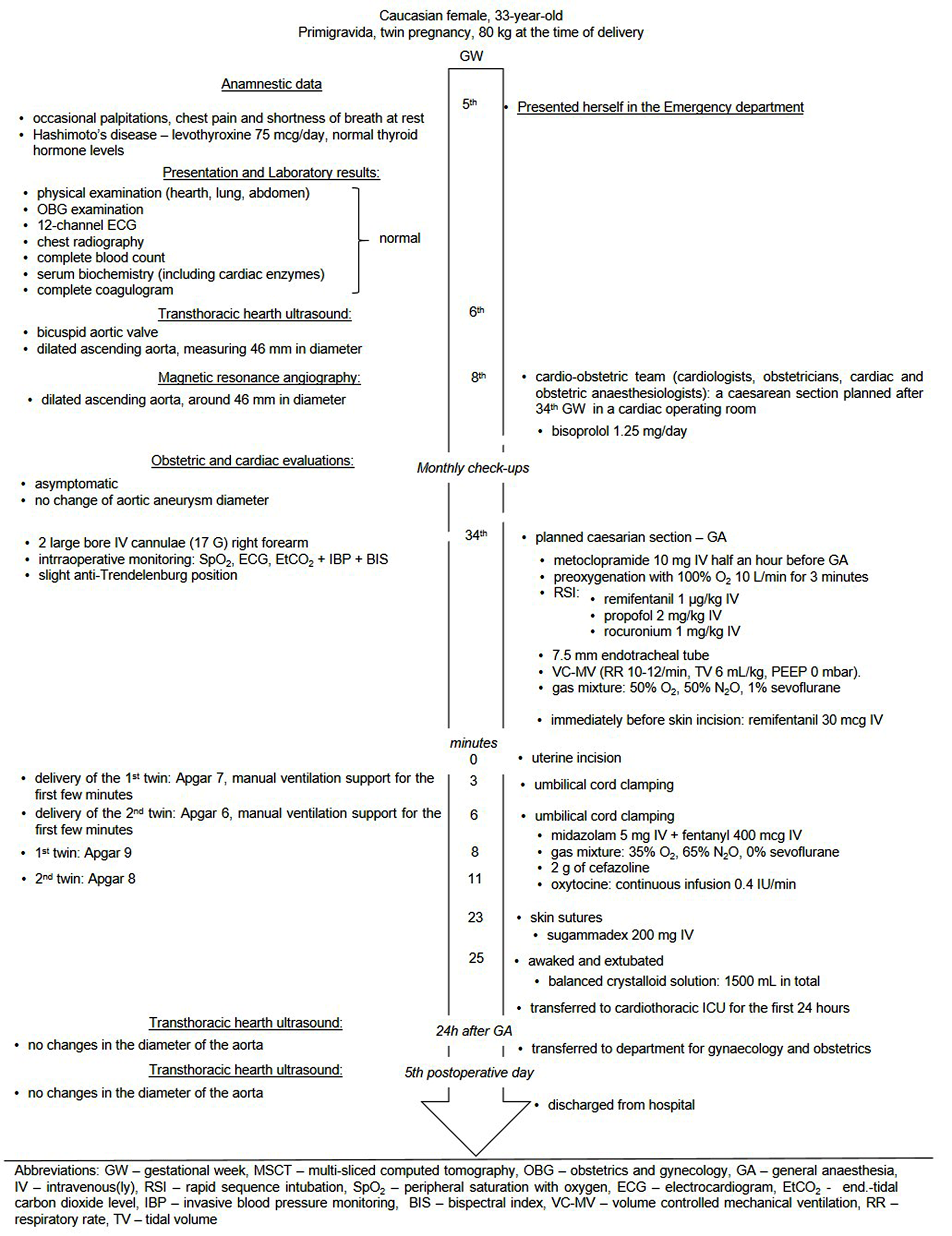
In both of our cases, management during pregnancy focused on the reduction of arterial pressure and control of heart rate with the use of a beta-blocker, while anesthesia for cesarean section aimed to mitigate the neuroendocrine response to intubation, thus maintaining hemodynamic stability and minimizing the risks of aortic aneurysm rupture or dissection.
Beta-blockers have been shown to successfully control blood pressure and heart rate and slow the progression of aortic root enlargement [8]. However, not all beta-blockers are safe for use during pregnancy. For instance, atenolol has been associated with fetal malformations and hypospadias when used during the first trimester, whereas metoprolol, propranolol and bisoprolol are deemed safe for use during pregnancy, although regular fetal growth monitoring is recommended [9, 10].
The management of pregnant patients with aortic aneurysm is probably best conducted through a multidisciplinary approach at a tertiary center, involving obstetrician, cardiologist, anesthesiologist, and preferably medical geneticist. Close monitoring, strict blood pressure control and regular heart ultrasound examinations to evaluate of aortic root diameter every 4–8 weeks are crucial [8,9,10]. Echocardiography is considered to be a safe method, so both of our patients had monthly cardiac evaluations that included cardiac ultrasound examination in addition to regular obstetric checkups.
On the other hand, CT angiography is the gold standard for diagnosing acute aortic dissection [8, 11], with the benefits of an accurate diagnosis outweighing the risks of radiation exposure (0.01–0.66 mGy), which are below the threshold for fetal injury (50 mGy). However, CT angiography was used as a diagnostic procedure before pregnancy in one of the described cases, while in the second case, magnetic resonance angiography was used to diagnose aortic aneurysm during early pregnancy. Currently, there are no studies that have shown any attributable harms of magnetic resonance imaging during any trimester of pregnancy [12].
Surgical repair of known aortic aneurysms and other valvular and aortic conditions meeting certain criteria is recommended prior to pregnancy (which had been also recommended to our patient in the second case), with surgery during pregnancy considered only when conservative treatment fails to control aortic dilation progression (aortic diameter increases too rapidly or exceeds 5 cm, or if aortic valve regurgitation is present) or when the mother’s life is at risk [8,9,10, 13].
If cardiothoracic surgical repair is indicated before 20 weeks of gestation, termination of pregnancy should be considered because cardiopulmonary bypass increases the risk of long-term neurological impairment and is related to a fetal loss rate of up to 33% [8, 14]. For parturients between 28 and 32 weeks of gestation, cesarean section before surgical repair is indicated because it is believed that risks of exposure of the baby to cardiopulmonary bypass exceeded the risks of premature delivery [8]. In such cases, maternal administration of intravenous magnesium-sulphate for fetal neuro-protection and corticosteroids for lung maturation should be administered [5]. For pregnancies at approximately 25 GW, surgical repair with the fetus remaining in utero, is thought to be the treatment of choice [11, 14].
Considerable hemodynamic changes are present during labor and the early post-partal period, since approximately 500 mL of venous blood is forced backwards with each uterine contraction. Pain and Valsalva maneuvers during pushing efforts significantly contribute to central venous pressure fluctuations. At the third stage of labor, the delivery of the placenta may lead to a situation of “autotransfusion” of an additional 500 mL of blood from the utero-placental into the maternal circulation. These changes also result in an increased central venous pressure, preload, and cardiac output, with a concomitant increase of the risk of aortic aneurysm rupture [15].
The mode of delivery in parturients with aortic aneurysm depends on factors such as aneurysm size, presence, or absence of aortic dissection, a possible underlying aortopathy and fetal gestational age [8]. For low-risk patients having an aortic diameter less than 40 mm, vaginal delivery is recommended, however, strict blood pressure and heart-rate control are still of great importance to decrease the risk of dissection or aortic rupture. Blood pressure and heart-rate are usually maintained by adequate analgesia via an epidural catheter [7, 16].
Cesarean section is typically recommended for parturients with an aortic diameter exceeding 45 mm, with careful attention to maintaining hemodynamic stability throughout the procedure, regardless of whether general or regional anesthesia is employed [7, 9, 16]. For both of our cases obstetricians opted for caesarian delivery, which were both conducted in a cardiac operating room. Since cardiac operating rooms are not well equipped for caesarian sections, all necessary obstetric surgical instruments and necessities were prepared for the caesarian section, while a neonatology table was preheated and ready for the neonate. The caesarian sections were performed by an obstetric team and a neonatology team with neonatal resuscitation equipment ready for the newborn, and the neonatal intensive care unit being informed about a possible admission. In addition, the cardiac surgery team and perfusionist (including their equipment) were ready in case of necessity.
Although regional anesthesia is a method of choice for cesarean section, general anesthesia (GA) is usually conducted in high-risk parturients, such as those suffering from preeclampsia or heart and vascular diseases [17,18,19]. Traditionally, for induction of GA in pregnant women, a rapid-sequence induction (RSI) with a hypnotic agent and a fast-acting muscle relaxant is used. However, the usual absence of opioid use during induction, to avoid respiratory depression in a neonate since they readily cross the placental barrier, leads to a strong neuroendocrine response that includes a severe increase in blood pressure and heart-rate [18, 20]. However, the main objective of anesthetic management during cesarean section in parturients with ascending aortic aneurysm is to maintain hemodynamic stability throughout the procedure [18, 21, 22], while attenuating the hemodynamic response to endo tracheal intubation and surgical stimulation without inducing respiratory depression in the neonate.
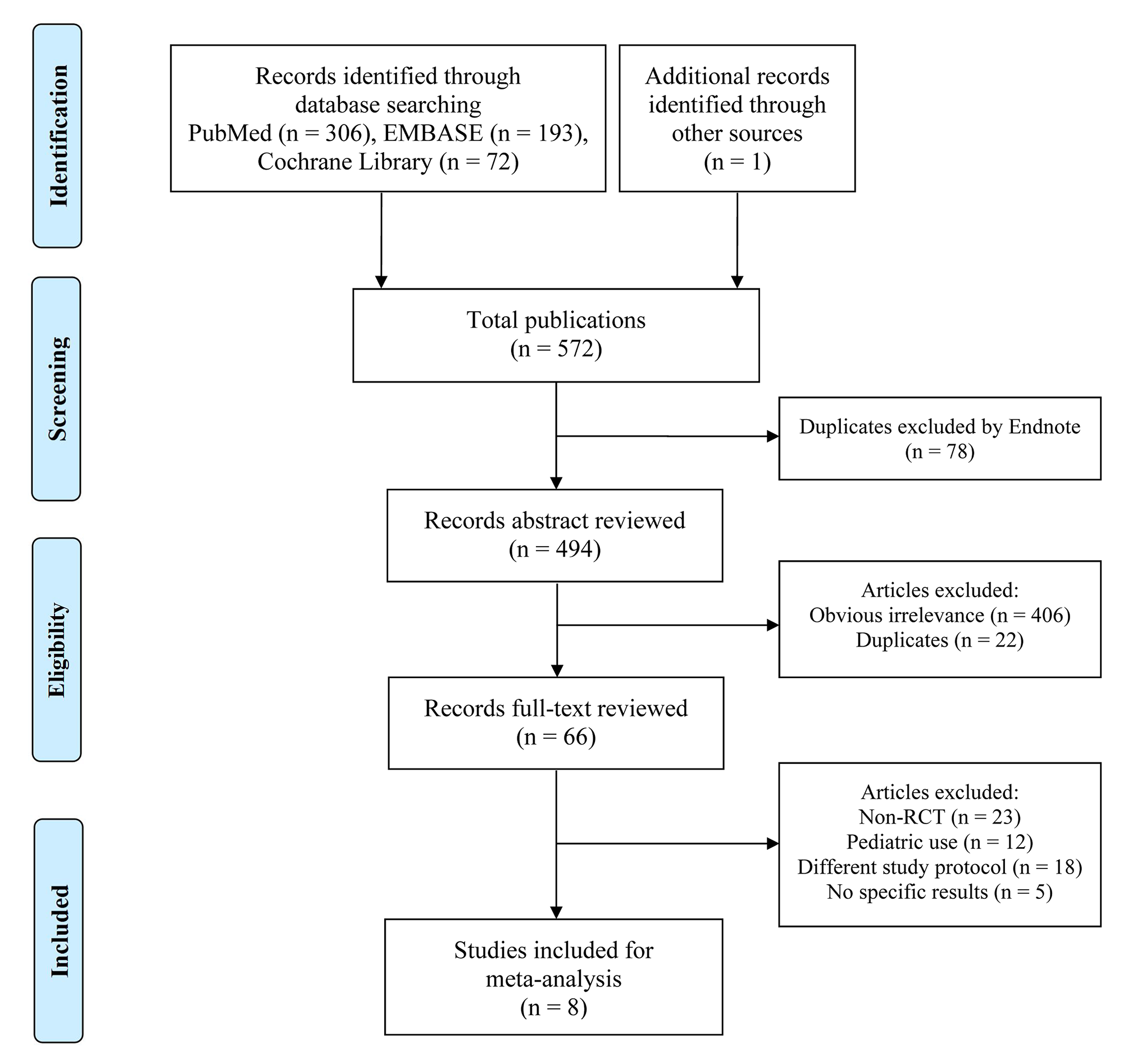
Several randomized placebo-controlled studies have investigated the effects of remifentanil on maternal hemodynamic variables and neonatal outcome with conflicting results, in our opinion mainly due to the differences in remifentanil dosage [17, 19, 21, 23,24,25]. However, the meta-analysis done in 2019 reported that the use of remifentanil probably maintains hemodynamic stability during the procedure, despite the conflicting results mentioned previously [22]. In our cases remifentanil was found to be a proper choice for maintaining hemodynamic stability.
Usually, the elimination of remifentanil from the newborn’s circulation at the time of birth is considered to be nearly completed due to its short duration of action [26]. However, all three of the newborns in our cases needed manual ventilation support during first minutes of life. Improvement in Apgar score was seen within 5-min after delivery and then, no further need for manual ventilation was necessary. Considering that the elimination half-life of remifentanil is 3–10 min, it is possible that remifentanil was not eliminated from the neonatal circulation at the time of delivery.
Although there are no studies investigating the conduction of general anesthesia for cesarean sections for parturients with aortic aneurysms, three published case reports described the successful use of remifentanil during general anesthesia for cesarean section in parturients with aortic aneurysm in Marfan syndrome [27,28,29]. In these three case reports, the authors reported the hemodynamic stability of parturients during the whole procedure, similar to our patients. On the other hand, Singh reported the need for neonatal ventilation one minute after delivery [27], as we reported, while the babies in Miyawaki’s [28] and Young’s reports [29] did not need for respiratory support.
Another way to avoid the respiratory depression in neonate is to reduce the use of opioids in parturient, which could be done by applying neuroaxial, instead of general anesthesia. Neuroaxial modes (spinal and epidural anesthesia) are reported to be preferred types of anesthesia for caesarean section, including for patients with aortic lesions [30], as in our patients. The first choice for both patients would thus be providing a spinal anesthesia. However, the first patient refused it and in the second we decided to conduct general anesthesia, mainly because of concerns on failure of spinal anesthesia in patients with connective tissue disorders [1,2,3]. Regardless of the type of anesthesia, it is priority to maintain hemodynamic stability by avoiding an increase of systemic vascular resistance (which increase aortic sheer stress) and hypotension (which endangers fetal perfusion) [30].
Except of the hypotension induced by anesthesia and hypertension due to the pain provoked by intubation and surgical stimulus, the application of uterotonics during the caesarean section is another important factor needing consideration when managing the parturient with ascending aortic aneurysm. Indeed, uterotonics are known to induce hypertension, with ergometrine having additional pronounced hypertensive and spastic effect on coronary arteries as well, which could even lead to myocardial infarction [31, 32]. Therefore, guidelines recommend avoiding ergometrine, with use oxytocin instead [10].
In our patients there were no hypertensive period during the operation and they did not need intervention of cardiac surgery team during and immediately after the caesarean section was performed. In addition, to ensure that there is no increase in aortic aneurism diameter we could use transoesophageal echocardiography (TOE) during the surgery. TOE during caesarean section in parturients with Marfan’s syndrome has been reported [27, 33]. However, we did not opt for it. Despite TOE is being considered safe and is the preferred imaging method in pregnancy [10], there is a risk of vomiting and aspiration, as well as a sudden increases in intra-abdominal pressure [10], which are not welcomed during the anesthesia nor abdominal surgery, especially when it could compromise the fetal circulation. Therefore, in both cases we relied solely on clinical status and monitoring (Figs. 1 and 4) with the addition of invasive blood pressure monitoring.
Overall, the management of parturients with ascending aortic aneurysm is complex and necessitates a comprehensive approach involving various medical specialties, including cardiologist, obstetrician, cardiac surgeon and anesthesiologist. If an ascending aortic aneurysm is diagnosed during the pregnancy or it was not repaired before the pregnancy as it is recommended, elective cesarean delivery in tertiary centers with available cardiac surgery and blood products is obligatory, to be prepared in cases of catastrophic events, such as aortic dissection or rupture during the perioperative period.
In the context of preoperative assessment, communication with patients regarding the risks and benefits of different anesthesia options is crucial. General anesthesia with administration of remifentanil is a reasonable choice in these cases because it enables the blunting of the hypertensive response to intubation and surgical stimulation. Due to placental transfer of remifentanil, neonatal respiratory depression is to be expected during the first minutes after delivery, especially if larger bolus dose of remifentanil is used. We consider maintenance of haemodynamic stability to be paramount in the prevention of a rupture or dissection of an ascending aortic aneurysm during delivery of a newborn.







留言 (0)