
記住我






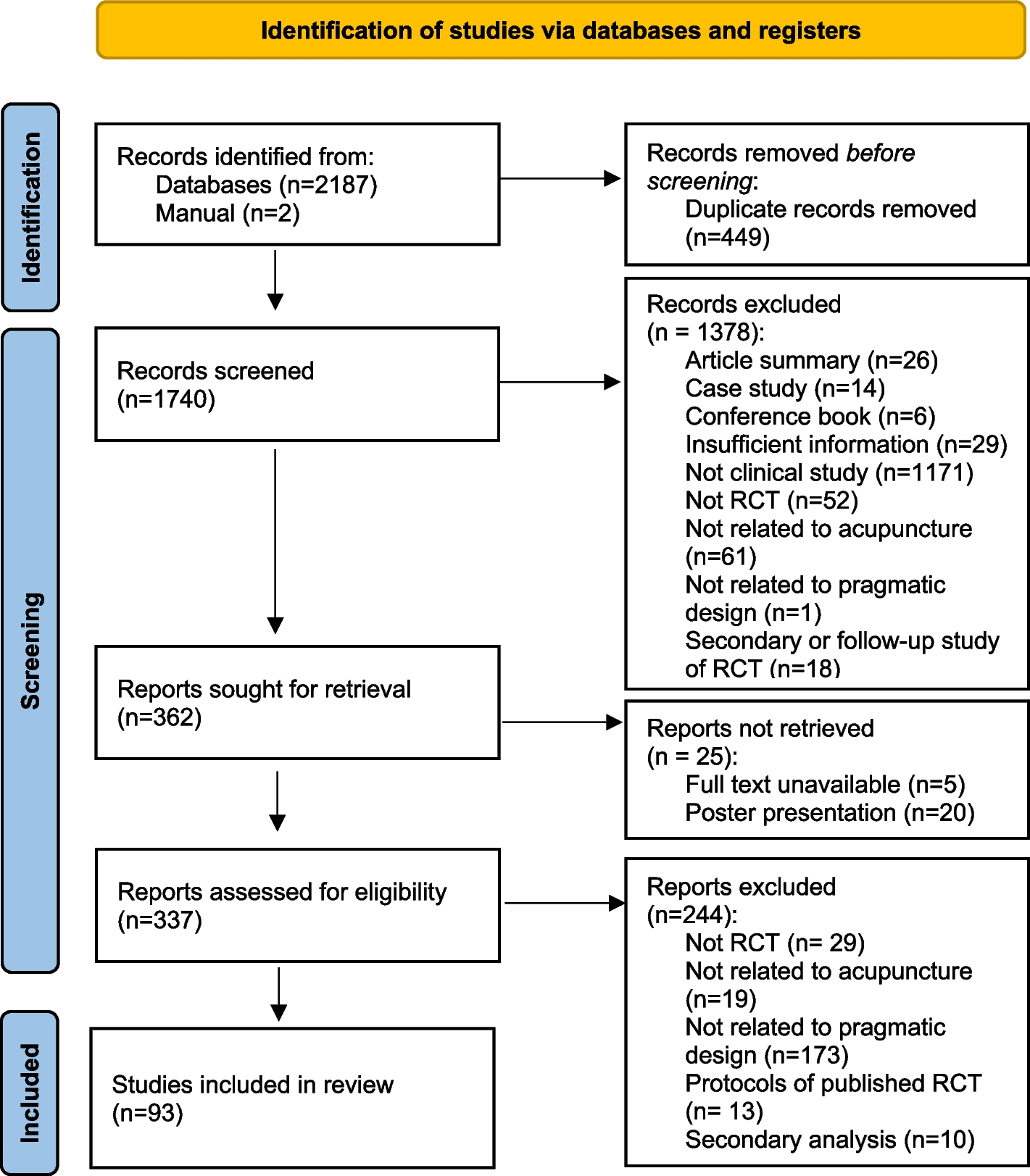
In total, 1,740 studies were found after searching and excluding duplicates. Based on the titles and abstracts, 1,647 studies were excluded, and 93 studies were finally included in the review. Two studies [13, 14] were considered to be the same trial; however, they reported different outcomes. Hence, we reviewed both articles. The flow chart [12] of this study is shown in Fig. 1.
Fig. 1
Sixteen studies were published until 2009 when PRECIS was first presented, [15] and 27 more were published between 2010 and 2015 when PRECIS-2 was presented. Thirty-eight studies in European countries (14 in the UK; 10 in Germany; 3 in Norway; 2 each in Denmark, Italy, Spain, and Sweden; 1 each in France, Greece, and the Netherlands), 35 studies in East Asian countries (21 in China; 9 in Korea; 3 in Japan; 1 each in Singapore and Hong Kong), 9 studies in the United States, 5 studies in Australia, 3 studies in Brazil, and 1 study each in Canada, Israel, and New Zealand was conducted. Three of the studies were written in Korean, Chinese, and German, and one was written in Japanese. Twenty-seven were protocol articles, 18 studies were pilot or feasibility trials, and one study was an interim analysis. The bibliographic characteristics of these studies are summarised in the Additional file 1.
PRECIS-2 scoresOverall resultsThe mean ± standard deviation (p-value) values of 10 domains (eligibility, recruitment, setting, organisation, flexibility:delivery, flexibility:adherence, follow-up, primary outcome, primary analysis, and control) were 3.49 ± 1.08 (p < 0.01), 3.48 ± 1.47 (p < 0.01), 3.26 ± 1.37(p = 0.06), 3.61 ± 1.43 (p < 0.01), 2.84 ± 1.50 (p = 0.83), 2.29 ± 0.83 (p = 0.99), 3.20 ± 1.24 (p = 0.07), 3.82 ± 1.22 (p < 0.01), 3.78 ± 1.73 (p < 0.01) and 3.76 ± 1.18 (p < 0.01) respectively (Fig. 2). The mean ± standard deviation (p-value) of the average score of nine domains in each study was 3.41 ± 0.64 (p < 0.01). The key factors of scoring in each RCT were summarised in Table 1. Individual scores of the studies and the scores of nine domains divided by subgroups [publication years before 2009, between 2010 and 2015, and after 2015; countries where five or more studies were reported (China, the United Kingdom, Germany, Korea, the United States of America, and Australia); type of study (pilot or feasibility trial and original RCT)] are shown in the Additional file 2.
Fig. 2
PRECIS-2 score of included studies
Table 1 Key pragmatic and explanatory factors used to score the PRECIS-2 of the included RCTsEligibilityWe assessed whether inclusion or exclusion criteria unnecessarily narrowed the number of possible participants compared to usual care. Contraindications to acupuncture and usual diagnostic criteria were not considered during scoring.
Fifteen studies that stated loose criteria without specific limitations were scored as five. Thirty-six studies with strict criteria, such as excluding common diseases or comorbidities, were considered pragmatic (scored as four). One study was scored as 3.5 since the study included patients with rather severe conditions. Twenty-one studies were scored as three, and the reasons for this included requiring laboratory results, setting a specific cut-off, or excluding common comorbidities, medication, low education level, and other diseases that could have affected the results of the intervention. One study was scored as 2.5 since it required specific inclusion criteria and excluded patients with common conditions and acupuncture experience. Twelve studies were scored as two, and these studies stated stricter criteria that required laboratory results, questionnaire scores, and daily diaries before enrolment, and excluded common conditions and medication that could have affected the results of the intervention. One study that required endoscopic results and excluded common comorbidities was scored as 1.5. Four studies were scored as one as they required extensive data before enrolment and exclusion of various conditions and diseases. Two studies did not properly state the inclusion/exclusion criteria, and thus the score was left blank.
RecruitmentIn the recruitment domain, we assessed whether additional strategies rather than the usual setting were used as part of the recruitment method.
Twenty-six studies were scored as five as they recruited participants only through referrals. They contacted eligible persons who visited a clinic or were admitted or mailed eligible patients after searching a local database or registry (achievable in the usual setting) [9]. Eight studies were scored as four since they advertised the trial only to patients who visited clinics or searched specialised hospital registries. Five studies were scored as three because they recruited participants as in the usual setting and additionally advertised the trial. One study that used massive advertisements and contacted possible patients through an outpatient clinic scored as 2.5. Nineteen studies were scored as two because they used advertisements in centres or newspapers or mailed to extensive groups of people who may have been ineligible from a database. Five studies were scored as one as some recruited participants from one specific unit, used massive advertisements, or compensated participants.Twenty-nine studies did not properly report their recruitment methods, and the score was left blank.
SettingWe assessed the appropriateness of study centres for managing patient conditions and research on the delivery of acupuncture or other interventions as well as the number of study centres.
Nineteen studies were scored as five as they were conducted in more than two general practices (GPs) or hospitals according to the disease or condition they investigated. Six studies were scored as four because they included two GPs or two specialised hospitals appropriately in accordance with participant conditions. Thirty-two studies were scored as three as they had conducted single-centre trials appropriately in accordance with participant conditions. Thirteen studies were scored as one because they conducted single-centre trials of specialised or tertiary hospitals on diseases or conditions which are usually treated by GPs. Twenty-three studies were scored as blank since they either failed to mention where the study was conducted and treatment delivered or reported that they conducted a multicentre trial, but the types of centres or clinics were not clearly identified.
OrganisationWe assessed the experience level of the acupuncture practitioners and the level of equipments used in the included studies.
Thirty-seven studies were scored as five as they required a minimum qualification that was required to practise acupuncture in each country without additional training. Six studies were scored as four because they included acupuncture practitioners with 10 years of experience. Twelve studies were scored as three since they required moderate additional training to perform acupuncture. One study was scored as 2.5 as it included two types of professionals without extensive training. Twenty studies were scored as two since they required extensive additional training, various kinds of professionals, or an academic degree. Five studies were scored as one as they required highly experienced and trained practitioners with an academic degree and additional professionals. Twelve studies either did not report or insufficiently reported the practitioner’s information and thus were scored as blank.
Flexibility: deliveryWe also assessed how much acupuncture treatments were individualised or based on the discretion of practitioners.
Seventeen studies were scored as five as acupuncture point selection and treatment were highly individualised and flexible at the discretion of practitioners. One study was scored as 4.5 since the delivery was highly flexible, but a protocol was suggested. Fifteen studies were scored as four as acupuncture prescriptions were generally individualised and flexible based on the practitioner’s discretion; however, other treatment regimens such as the number of treatment sessions or co-intervention were minimally fixed. Fifteen studies were scored as three since they showed semi-individualised (flexible within certain standard treatment procedures) acupuncture treatments, fixed treatment sessions, and cointerventions. Sixteen studies were scored as two as their acupuncture treatments were standardised and defined strictly as treatment sessions and cointervention with adherence management of practitioners. Twenty-four studies were scored as one since they thoroughly investigated standardised acupuncture treatments within a strict discipline. Five studies did not report sufficient information on the delivery of the intervention and thus were scored blank.
Flexibility: adherenceAny specific method used to manage the adherence of participants to intervention was assessed.
Two studies were scored as four since they attempted to maintain adherence as in usual care by allowing non-attendance of participants or sending messages for upcoming sessions. One study was scored as three because the study fixed minimum treatment sessions prior to inclusion. Ten studies were scored as two because they excluded poor compliance from trials or measured various outcomes to promote adherence. One study was scored as one as it compensated participants at each follow-up visit. Seventy-nine studies either did not sufficiently report any methods regarding adherence or were not applicable.
Follow-upThe frequency and duration of follow-ups, additional data collection, or any other methods regarding follow-up management were also measured. Typically, acupuncture treatments consist of several sessions, and therefore follow-up outcome assessments during treatment sessions were considered pragmatic unless they were more extensive than usual care.
Thirteen studies were scored as five since either participants were not followed up after the end of the treatment session or medical records were used for follow-up assessments. Thirty studies were scored as four because they carried out follow-up assessments, but they were not extensive in terms of frequency and duration. Twenty-three studies were scored as three because their follow-up assessments were considered quite intense in terms of frequency and duration. Fourteen studies were scored as two since the follow-ups were intense as compared with usual care and quite intense with extensive outcome measurements or excessive reminders used. Twelve studies were scored as one since the follow-ups were intense in terms of frequency and duration, and extensive outcome measurements were collected with participants either individually contacted to turn in outcome measurements or compensated on each follow-up and at the end of the study. One study did not properly state the follow-up strategy and was scored as a blank.
Primary outcomeWe additionally measured whether the primary outcome was patient-centred and available in usual care. If there were many outcomes like in the pilot study, the outcome used to calculate the sample size was considered the primary outcome.
Thirty-three studies used pragmatic measurements such as the visual analogue scale or objective outcomes using medical records and were scored as five. Thirty studies were scored as four as most of them used questionnaires related to the disease or condition, and this was regarded as pragmatic. Five studies were scored as three because they employed questionnaires that were less commonly used in usual care. Two studies were scored as 2.5 since they used questionnaires that were unrelated to the disease or condition. Sixteen studies were scored as two because they used unrelated outcome measurements or outcome measurements requiring intense data collection such as daily diaries or additionally trained assessors. Three studies were scored as one because they used various outcomes as primary outcomes and required additional professionals and equipment. Four studies did not determine the primary outcome and measured various outcomes without sample calculation, and the score for these was left blank.
Primary analysisWe also assessed the statistical methods such as the intention-to-treat (ITT) and per-protocol analysis.
Fifty studies analysed all the participants at randomisation and were scored as five. Twelve studies were scored as four since they used a full analysis set or modified ITT (for instance, including participants who received at least one treatment session) even though they used ITT analysis. Twenty-three studies were scored as one since they used the per-protocol analysis or excluded missing data and poor compliance despite the fact that they used ITT analysis. Eight studies did not report the analysis methods, and these scores were left blank.
ControlWe also measured which interventions were used in control groups. Studies that provided usual care without any discipline to their control groups were scored as five; thus, 27 studies that used usual care without specific restrictions as the control group were scored as five. Eighteen studies were scored as four since there was a restriction placed on usual care in the control group. Twenty-six studies were scored as three since they used fixed treatments available in usual care as the control group. One study was scored as two since the study used physical touch in the control group that tended to function as sham acupuncture. Six studies used sham-acupuncture treatment in the control groups and were scored as one. Fifteen studies that did either not report the extent to which usual care or sham treatment was applied in the control group or had no available control group (for instance, all groups were using acupuncture treatment for experimental purposes) were left blank in this domain.
留言 (0)