
記住我


Established by federal law in 1965, Medicare has grown to become the largest healthcare purchaser in the United States. In 2022, Medicare covered approximately 65 million lives at a total expenditure of $905 billion and is expected to cover more than 80 million beneficiaries at a cost of approximately $1.5 trillion by 2030.1 The program helps with healthcare expenses for people aged 65 years or older and some younger individuals with various disabilities (Table 1). Because Medicare is the largest, most transparent, and most critical payer for most hospitals and many other healthcare entities, the approaches Medicare leaders take to quality and cost dominate and shape the healthcare insurance industry.
Table 1 - Medicare Plans (Traditional Medicare and Medicare Advantage) Traditional Medicare Beneficiary Costsa General Coverage Provider Network Restrictions Preauthorization for Services Part A Dd and Co, but no Prem unless payroll taxes paid for <10 years by beneficiary or spouse Hospital services, skilled nursing facility care, home health care, hospice No No (unless nonroutine or special coverage rule) Part B Prem, Dd, Co Outpatient and physician services, durable medical equipment No No (unless nonroutine or special coverage rule) Part D Prem, Dd, Co Prescription medications Yes Yes (if the drug is on a plan's list for preauthorization) Medigap Prem Dd and Co for Part A and Part B No No Medicare Advantage No Prem for Part A unless payroll taxes paid <10 yr by beneficiary or spouse; Prem, Dd, and Co for Part B, medications, and other services Part A and Part B, ± medications, ± routine hearing, eyesight, dental Yes Yes (many, but not all services)Prem = premium, Dd = deductible, Co = copay or coinsurance, y = year.
aPeople who qualify for both Medicare and Medicaid (a.k.a. dual-eligible beneficiaries) may receive coverage for Medicare beneficiary costs through the Medicare Savings Programs, a set of four Medicaid benefit programs that help pay for Medicare costs in this group.
Medicare was initially crafted in the likeness of an existing Blue Cross insurance framework and included two parts: A (hospital services) and B (outpatient and doctor's office services).2 Both parts were designed in a fee-for-service format: A customary, prevailing, and reasonable fee was charged to Medicare, and the bill was paid through the Health Care Financing Administration [the predecessor of the Centers for Medicare and Medicaid Services (CMS)]. Part A now covers inpatient care in a hospital, skilled nursing facility care, laboratory tests, surgery, home health care, hospice care, and a large portion of graduate medical education. Part B covers healthcare providers' services, durable medical equipment, some home health services, some preventive services, some outpatient prescription drugs, ambulance services, and physiotherapy services.
Two additional programs were added to Medicare in the 1980s and early 2000s: Parts C and D. Medicare Part C (a.k.a. Medicare Advantage [MA]) was formulated by federal legislation in 1982 and evolved into its current structure over the ensuing four decades. The program authorizes Medicare to contract with commercial insurance carriers and provider-owned health plans to accept cost responsibility (ie, risk) for defined components of their enrollees' care in exchange for predetermined, risk-adjusted payments per enrollee to cover the cost of benefits included in Medicare Part A and a portion of benefits in Part B. This program has grown to cover 30.8 million participants, or just over half of the eligible Medicare population as of March 2023.3
Medicare Part D was established by federal law in 2003 and went into effect in 2006. This program provides an outpatient prescription drug benefit. Medicare beneficiaries can join Part D as an add-on to traditional (ie, original) Medicare, or they can be automatically enrolled in Part D as part of an MA plan that provides pharmaceutical benefits. More than three quarters of all Medicare beneficiaries received Part D prescription drug benefits in 2023.4
Funding for Medicare is through two accounts held by the US treasury: the Hospital Insurance Trust Fund (Medicare Part A) and the Supplementary Medical Insurance Trust Fund (Medicare Parts B and D). Both funds comprise general revenues and payroll taxes. The Supplementary Medical Insurance Trust Fund also comprises premiums from people enrolled in Medicare Parts B and D. Medicare Part C is paid for by funds from both Part A and B treasury accounts and enrollee payments to MA insurers.
Medicare is managed by CMS, an agency of the US Department of Health and Human Services. Numerous public and private sector stakeholders interact with CMS. There is a statutory requirement for CMS to announce any newly planned rules for Medicare with open comments from the public before final rule publication.
Value Equation and Quality Measures in Health CareThe Institute of Medicine defines quality as the degree to which healthcare services increase the likelihood of desired health outcomes and are consistent with current professional knowledge.5 In 2006, Michael Porter and Elizabeth Teisberg coined the term ‘value-based’ health care, emphasizing the importance of patient-centered health outcomes at acceptable costs. In effect, they defined value as a ratio of quality to cost.6
Quality assessment has been organized by CMS into two domains of measured performance (outcome and process), aligning with the Donabedian framework for healthcare quality evaluation.7 Performance measures selected by CMS are from those endorsed through a statutorily mandated undertaking of national, multistakeholder review. Hundreds of measures have been endorsed over the years, but not all have been adopted by CMS for use in value-based programs. The current contract for managing review of performance measures is with Battelle's Partnership for Quality Measurement.8 Several active CMS measures relevant to orthopaedic surgery are presented in Table 2, and a full list of measures is available online in the CMS Measures Inventory.
Table 2 - Examples of Medicare Quality Measures Relevant to Orthopaedic Surgery in 2023 Measure Identification Number and Description 1 - Surgical site infection 85 - Back pain after lumbar diskectomy/laminectomy 86 - Back pain after lumbar fusion 141 - Communication with the physician or other clinician managing ongoing care after fracture for men and women aged 50 years and older 162 - Consumer assessment of healthcare providers and systems outpatient and ambulatory surgery survey 276 - Functional status after lumbar diskectomy/laminectomy 277 - Functional status after lumbar fusion 278 - Functional status assessment for total hip arthroplasty 279 - Functional status assessment for total knee arthroplasty 285 - Functional status change for patients with hip impairments 286 - Functional status change for patients with knee impairments 287 - Functional status change for patients with lower back impairments 288 - Functional status change for patients with lower leg, foot, or ankle impairments 289 - Functional status change for patients with neck impairments 290 - Functional status change for patients with shoulder impairments 345 - Hospital visits after orthopaedic ambulatory surgical center procedures 349 - Hospital-level, 30-day, all-cause, risk-standardized readmission rate after elective primary total hip arthroplasty and/or total knee arthroplasty 350 - Hospital-level, risk-standardized complication rate after elective primary total hip arthroplasty and/or total knee arthroplasty 355 - Hospital-level, risk-standardized payment associated with a 90-day episode of care for elective primary total hip and/or total knee arthroplasty 401 - Functional outcome measure: change in mobility score 411 - Leg pain after lumbar diskectomy/laminectomy 412 - Leg pain after lumbar fusion 453 - MRI lumbar spine for lower back pain 456 - Multimodal pain management 502 - Patient-centered surgical risk assessment and communication 655 - Risk-standardized complication rate after elective primary total hip arthroplasty and/or total knee arthroplasty for Merit-Based Incentive Payment System 725 - Total knee arthroplasty: shared decision making: trial of conservative (nonsurgical) therapy 726 - Total knee arthroplasty: venous thromboembolic and cardiovascular risk evaluation 737 - Unplanned revision surgery within the 30-day postoperative period 758 - Venous thromboembolism prophylaxis 763 - Wrong site, wrong side, wrong patient, wrong procedure, wrong implant 1606 - Clinical data registry reporting 1618 - Hospital-level, risk-standardized improvement rate in patient-reported outcomes after elective primary total hip and/or total knee arthroplasty 344 - Hospital visits after hospital outpatient surgery 403 - Functional outcome measure: discharge mobility score 736 - Unplanned hospital readmission within 30 days of principal procedureResponding to concerns raised over the burden of complex reporting requirements for quality performance, leaders in CMS are working to align quality measures into a universal foundation that can be used across the various CMS value-based payment programs.9 In addition, CMS is moving toward patient-reported outcome measures with recent establishment of the hospital-level total hip arthroplasty/total knee arthroplasty patient-reported outcome–based performance measure. This measure has been added to the Hospital Inpatient Quality Reporting Program, with a financial penalty for failure to achieve at least 50% patient engagement for both preoperative and 1-year postoperative assessments, as well as measurable clinical benefit.10 The same requirement is being proposed for outpatients.11
Experts in CMS have also been working to transition performance measures to an electronic format, termed the electronic Clinical Quality Measures (eCQM), with performance measures reported directly from electronic medical record systems in hospitals, clinicians' offices, and other settings—a move that is intended to reduce the reporting burden and cost for providers. A list of current CMS-used electronic quality measures is available online in the eCQI Resource Center.
Medicare Value-Based Care Forces Shaping Medicare Value-Based CareThe costs of the Medicare program have increased substantially since the program's inception because of various factors, including population growth, inflation, wasteful spending, and a demand for new technologies that do not all contribute commensurately to improved outcomes.1,12 From the 2023 Medicare Boards of Trustees report, the Medicare Part A Trust Fund is expected to be depleted by 2031.13 This prediction is annually updated after Congressional moves to control spending and maintain sufficient funding.
The premise of value-based health care is to incentivize and improve care quality while containing the overall costs of care.14 One of the earliest CMS value-based programs was attempted (albeit without outcome measures) in 1983 when the Diagnosis Related Groups codes were developed, and for the first time, hospitals received a fixed payment for each patient stay. In 1992, the Resource-Based Relative Value Scale was embraced by CMS to help mitigate high variability in physician payments for equivalent services. This new payment construct established relative value unit (RVU) designations for all medical services and procedures.
In 2006, the Physician Quality Reporting System was implemented by CMS to motivate provider reporting of quality measures related to preventative care and chronic disease management of Medicare beneficiaries. Three years later, the Health Information Technology for Economic and Clinical Health Act was passed and incentivized the stepped adoption of electronic health records for digitization of data and reporting of performance measures to CMS (a.k.a. “Meaningful Use”). In 2010 and 2015, the Patient Protection and Affordable Care Act (ACA) and the Medicare Access and Children's Health Insurance Program Reauthorization Act, respectively, were passed into law and provided foundations for many of the current value-based Medicare Payment Programs. This accretion of federal laws and subsequent federal agency rules created an intricate patchwork of CMS payment constructs.
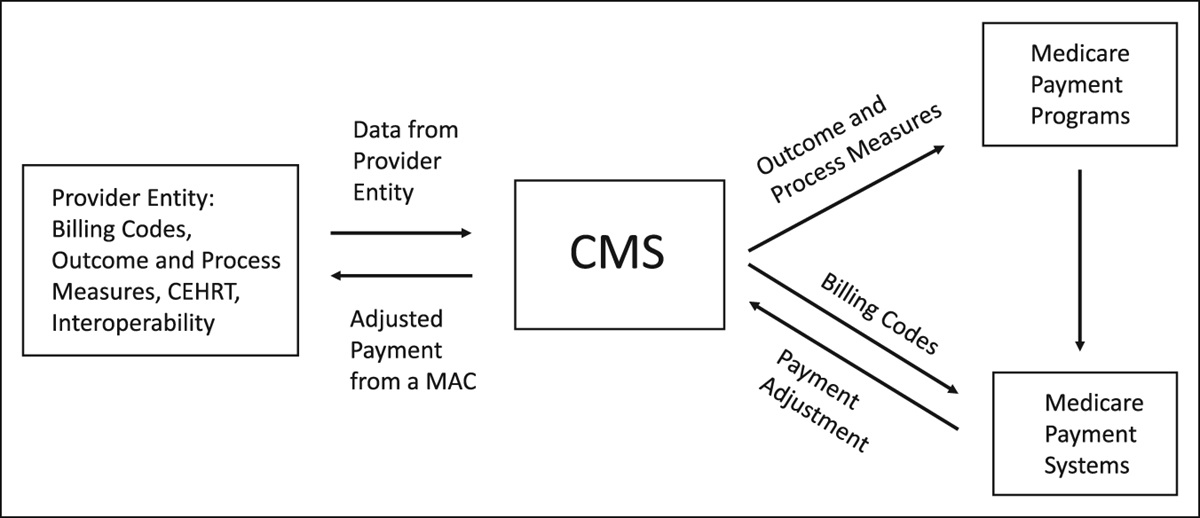
Value-Based Payment Programs (Traditional Medicare)Fundamentally, value-based Medicare Payment Programs are intended to incentivize providers for care quality rather than solely volume in traditional Medicare. CMS receives multitudinous data points from providers, including billing codes, care assessment instruments, quality performance measures, annual cost reports, and electronic health record improvement attestations, and match these data points to the appropriate Payment Systems and Payment Programs to determine final payment amounts. In effect, data points are matched with a Payment System(s) and an overarching Payment Program(s) is leveraged to adjust payments upward or downward (Figure 1).
 Figure 1:
Figure 1: Diagram showing interactions between Provider Entity, Medicare Payment Systems, and Medicare Payment Programs for payment adjustments to the Provider Entity in traditional Medicare. CMS = Centers for Medicare and Medicaid Services, CEHRT = certified electronic health record technology, MAC = Medicare Administrative Contractor.
Nearly everything in health care is codified, from diseases to treatments to durable medical goods. Several coding systems have been devised or adopted by CMS for different purposes and different settings.15 As examples, the International Classification of Diseases, 10th Revision, Clinical Modifications (ICD-10-CM) codes designate diseases and health-related conditions, and the Current Procedural Terminology (CPT) codes designate services or procedures performed by clinicians in an inpatient, outpatient, or ambulatory surgery setting. These and other coding systems are used by CMS in various Medicare Payment Systems (Table 3).
Table 3 - Medicare Recognized Coding Systems Used in Medicare Payment Systems in 2023 Medicare Payment Systems Medicare Coding Systems Medicare Payment Systems Medicare Coding Systems Physician Payment System ICD-10-CM, CPT (HCPCS I), HCPCS II, POS, NDC, LOINCa, SNOMED CTa Inpatient Psychiatric Facilities Prospective Payment System ICD-10-CM, ICD-10-PCS, Revenue Codes, NDC, LOINCa, SNOMED CTa Acute Care Hospital Inpatient Prospective Payment System ICD-10-CM, ICD-10-PCS, HCPCS II, CMG in the form of MS-DRG, Revenue Codes, NDC, LOINCa, SNOMED CTa Long-Term Care Hospital Prospective Payment System ICD-10-CM, ICD-10-PCS, CMG in the form of MS-LTC-DRG, Revenue Codes, NDC, LOINCa, SNOMED CTa Hospital Outpatient Prospective Payment System ICD-10-CM, ICD-10-PCS, CPT (HCPCS I), HCPCS II, APC, POS, Revenue Codes, NDC, LOINCa, SNOMED CTa Skilled Nursing Facility Prospective Payment System ICD-10-CM, CPT (HCPCS I), HCPCS II, HIPPS, CMG in the form of RUG, NDC, LOINCa, SNOMED CTa Inpatient Rehabilitation Facility Prospective Payment System ICD-10-CM, ICD-10-PCS, CMG, LOINCa, SNOMED CTa Hospice Payment System ICD-10-CM, HCPCS II, Revenue Codes, NDC, LOINCa, SNOMED CTa Home Health Prospective Payment System ICD-10-CM, CPT (HCPCS I), HCPCS II, HIPPS, NDC, LOINCa, SNOMED CTa End-Stage Renal Disease Prospective Payment System ICD-10, HCPCS II, ESRD CMC; Revenue Codes, NDC, LOINCa, SNOMED CTa Ambulatory Surgical Center Payment System ICD-10-CM CPT (HCPCS I), HCPCS II, APC, POS, Revenue Codes, NDC, LOINCa, SNOMED CTa — —ICD-10-CM = International Classification of Diseases, 10th Revision, Clinical Modification; ICD-10-PCS = International Classification of Diseases, 10th Revision, Procedure Coding System, CPT = Current Procedure Terminology (designate services or procedures), HCPCS I = Healthcare Common Procedure Coding System I (designate services or procedures—same as the CPT coding system), HCPS II = Healthcare Common Procedure Coding System II (designate medications, durable medical equipment, ambulance transport services, prosthetics, orthotics), POS = Place of Service (designate where service was performed), Revenue Codes (designate type of service or item associated with a specific charge), CMG = Case-Mix Group (designate patient groups with similar clinical and resource utilization characteristics), NDC = National Drug Codes (identify specific drugs and medications), LOINC = Logical Observation Identifiers Names and Codes (designate laboratory tests and results), SNOMED CT = Systemized Nomenclature of Medicine Clinical Terms (designate standardized electronic health information exchange), APC = Ambulatory Payment Classification (designate outpatient services), MS-DRG = Medicare Severity Diagnosis-Related Groups (designate patient groups based on similar clinical and resource utilization characteristics), HIPPS, Health Insurance Prospective Payment System rate codes (designate specific sets of patient characteristics), MS-LTC-DRG = Medicare Severity Long-Term Care Diagnosis Related Groups (designate patient groups based on similar clinical and resource utilization characteristics) RUG = Resource Utilization Group (classify patients based on care needs), ESRD CMC = End-Stage Renal Disease Claim Modifier Codes.
aCodes not used directly in the Medicare Payment System but may play a role in data exchange; dental codes are not included in this table.
Medicare Payment Systems define fee-for-service (ie, prospective flat-rate) payment amounts to care providers and care facilities.16 The fee schedules for Medicare Payment Systems are revisited annually in Congress with input from the Medicare Payment Advisory Commission (MedPAC), an independent, nonprofit legislative branch group comprising experts in the delivery and financing of healthcare services.17 The methodologies for calculating payments in the many Medicare Payment Systems vary. For example, the Physician Payment System operates through a Physician Fee Schedule that comprises CPT codes and assigned RVU numbers with place of service and geographic practice cost index adjustments, a monetary conversion factor for each RVU, and National Correct Coding Initiative editing rules.18 The Physician Fee Schedule includes physicians and other types of health professionals. Anesthesia services utilize this methodology or a time-based unit formula with a different conversion factor. The CPT code set, including RVU updates, and the conversion factors are subject to annual changes.
Since 1992, there has been a budget neutrality requirement in the Physician Fee Schedule involving a $20 million ceiling for any projected annual overage in allotted spending. Forecasted spending exceeding this cap leads to redistribution of payments for services in the Physician Fee Schedule, typically by decreasing the monetary conversion factors. Medical societies are lobbying Congress to revise budget neutrality policies that have resulted in frequent annual reductions in the the RVU and anesthesia conversion factors. Medical societies are also lobbying Congress to update these conversion factors to keep pace with inflation in the future--adjustments that would reflect the Medicare Economic Index, a government measure of inflation in medical practice costs.19
Medicare Payment Programs (Table 4) interact with Medicare Payment Systems to adjust final payment amounts based on numerous performance measures.20 Outcome and process performance measures cross over in the various Medicare Payment Programs, and more than one Payment Program can influence reimbursement. For example, Medicare payments to a hospital may be negatively affected up to 6% through a combination of the Hospital Value-Based Purchasing Program, Hospital Readmissions Reduction Program, and Hospital-Acquired Condition Reduction Program.21 A hospital must complete reporting to CMS as required by the Hospital Inpatient Quality Reporting Program to mitigate additional payment penalties. Hospitals with a poor payer mix may receive supplemental Medicare payments (ie, disproportionate share hospital payments) based on Medicare funding methodologies.22 Because the typical US hospital is reliant on Medicare for as much as one-third of revenues, payment rewards and penalties are consequential.
Table 4 - Examples of Medicare Payment Program Payment Adjustments Through the Medicare Payment Systems in 2023 Medicare Payment Programs Penalties/Rewards in Medicare Payment Systems Quality Payment Program (clinicians) Payment adjustments through the Physician Payment System. Penalties up to 9% and rewards up to 2.33% based on specified measures for providers participating in MIPS. For providers participating in Advanced APMs, shared losses or savings with CMS and reward of 3.5%. Hospital Value-Based Purchasing Program Payment adjustments through the Acute Care Hospital Inpatient Prospective Payment System. Penalties up to 2% for acute care hospitals based on quality of care (clinical outcomes, safety, patient experience, efficacy) provided in the inpatient setting. Reward (budget neutral) for highest performing hospitals. Hospital Readmissions Reduction Program Payment adjustments through the Acute Care Hospital Inpatient Prospective Payment System and the Long-Term Care Hospital Prospective Payment System. Penalty up to 3% based on 30-day all-cause hospital readmissions for specific conditions and procedures.a Hospital-Acquired Condition Reduction Program Payment adjustments through the Acute Care Hospital Inpatient Prospective Payment System. Penalty of 1% based on one measure of patient safety and five hospital-acquired infection rates.b Facilities in the lowest performing 25% are penalized. Hospital Inpatient Quality Reporting Program Payment adjustments through the Acute Care Hospital Inpatient Prospective Payment System. Penalty of 25% of the annual payment rate update if all abstracted and electronic quality metric inpatient reporting requirements are not met. Ambulatory Surgical Center Quality Reporting Program Payment adjustments through the Ambulatory Surgical Center Payment System. Penalty up to 2% if reporting requirements are not met. Skilled Nursing Facility Value-Based Purchasing Payment adjustments through the Skilled Nursing Facility Prospective Payment System. Penalty up to 2% based on 30-day all-cause hospital readmissions. Reward (budget neutral) for highest performing facilities. End-Stage Renal Disease Quality Incentive Program Payment adjustments through the End-Stage Renal Disease Prospective Payment System. Penalty up to 2% to renal dialysis facilities based on a total performance score of several clinical and reporting measures. Home Health Value Based Purchasing Payment adjustments through the Home Health Prospective Payment System. Beginning in 2025, penalties and rewards up to 5% for home health agencies based on a set of quality measures.MIPS = Merit-Based Incentive Payment System, APM = Alternative Payment Model.
aAcute myocardial infarction, chronic obstructive pulmonary disease, heart failure, pneumonia, coronary artery bypass graft surgery, elective primary total hip arthroplasty, elective primary total knee arthroplasty.
bCentral line-associated bloodstream infection, catheter-associated urinary tract infection, surgical site infection for abdominal hysterectomy and colon procedures, methicillin-resistant Staphylococcus aureus bacteremia, Clostridium difficile infection.
The Quality Payment Program is arguably the most intricate of the value-linked Medicare Payment Programs in traditional Medicare and defines clinician payment rules. The program includes two options for eligible clinician participation: (1) traditional Merit-Based Incentive Payment System (MIPS) and (2) Advanced Alternative Payment Models (APMs) (Figure 2; Table 5).23,24 Participation in MIPS is by default, whereas participation in an Advanced APM(s) requires an application(s) to CMS. Clinicians are expected to take part in MIPS unless they do not meet a volume threshold, they are in their first year of participating in the Medicare program, or they are participating in an Advanced APM. If a participating provider does not meet eligibility for MIPS, Medicare payments are based on the Physician Fee Schedule without additional incentives. In special circumstances defined by CMS, clinicians can also apply for a MIPS exception to avoid program penalties.
 Figure 2:
Figure 2: Diagram showing the Quality Payment Program (applicable to Medicare providers such as physicians). MIPS = Merit-Based Incentive Payment System; APM = Alternative Payment Model.
Table 5 - Medicare Payment Models in the Quality Payment Program Available for Orthopaedic Surgery Participation in 2023 Medicare Payment Models in the Quality Payment Program Qualifies for Merit-Based Incentive Payment System Alternative Payment Modela Qualifies for Advanced Alternative Payment Model (Care Episode, Clinical Condition, or ACO) Bundled Payment for Care Improvement Advanced Model Y Y Comprehensive Care for Joint Replacement Payment Model (Track 1—CEHRT) Y Y Comprehensive Care for Joint Replacement Payment Model (Track 2—non-CEHRT) Y N Medicare Shared Savings Program BASIC Track Levels A, B, C, and D Y N Medicare Shared Savings Program BASIC Track Level E Y Y Medicare Shared Savings Program Enhanced Track Y YY = qualifies for payment model, N = does not qualify for payment model, CEHRT = certified electronic health record technology, ACO = accountable care organization.
aMerit-Based Incentive Payment System Alternative Payment Models that use Merit-Based Incentive Payment System rules when criteria are not met for participation in the Advanced Alternative Payment Model of the same name. A list of all Medicare payment models is available at https://qpp.cms.gov/apms/advanced-apms.Barring employment and/or care facility stipulations, clinicians have the option of choosing to be nonparticipating Medicare clinicians. These providers accept Medicare Physician Fee Schedule rates and can charge patients more than the approved amounts for services provided, although with state-defined limits up to 15% above Physician Fee Schedule rates. Nonparticipating Medicare clinicians do not receive monetary incentives or penalties associated with the Quality Payment Program. In the absence of employment and/or care facility restrictions, clinicians can also opt out from Medicare altogether by signing an exclusion agreement.
For eligible clinicians participating in MIPS, payment adjustments are based on performance measures in four areas: quality (ie, outcome and process measures that best fit a practice), cost, improvement activities (eg, care coordination), and electronic record interoperability. The MIPS Value Pathways are new and evolving means for clinicians to report streamlined quality and improvement activity measures more aligned to their specialties or health conditions treated. The performance measures are converted into a point system with a maximum score of 100 points and influence payment adjustments two years later. For example, peak MIPS performance in 2023 will result in a positive CMS payment of 2.33% in 2025. There are substantial CMS payment penalties (up to 9% in 2025 based on 2023 data) for suboptimal reporting of performance measures or failure to report performance measures altogether. The current threshold to avoid a penalty is 75 points. MIPS is budget neutral because penalties offset bonuses.
Advanced APMs operate through two types of payment models: (1) population of people [eg, accountable care organization (ACO)] and (2) care episode or clinical condition (eg, total joint arthroplasty or congestive heart failure). In a population of people model, a mean target cost per beneficiary is set according to a CMS methodology and adjusted for risk through the Hierarchical Condition Categories (HCCs) that are associated with ICD-10-CM diagnosis codes. In a care episode or clinical condition model, a target price is crafted by CMS to cover the entire continuum of care over a set time period for a single medical event. A covered patient's journey may include physician care, other provider care, acute and post-acute hospitalization, and skilled nursing facility stay.
Payments from CMS to providers participating in Advanced APMs are either prospective or retrospective in design. If a prospective payment, remittance at the target price is made and the episode initiator (a.k.a. episode convener) directs distribution to parties involved in the patient care journey. If a retrospective payment, fee-for-service charges are submitted by providers and reconciled at intervals with the preset target price. In either case, Advanced APM provider participants share in savings or losses with CMS that result from the difference between the target price and the total cost of care.
Because of added financial risk, a supplemental incentive payment is available for providers participating in an Advanced APM who meet payment or patient volume thresholds (a 3.5% incentive in 2025 for performance year 2023, followed by a higher Physician Fee Schedule update for performance years 2024 and beyond). Providers in an Advanced APM are also excluded from MIPS reporting requirements. However, if eligible clinicians who participate in an Advanced APM do not meet a defined threshold for payments or patients, reimbursement rules default to MIPS in the so-called MIPS APM approach.25
Eligible providers can also apply electively for MIPS APM participation if thresholds for Advanced APM participation are not possible. The advantages of participating in a MIPS APM over traditional MIPS are favorable scoring and the potential for a reduced reporting burden through the APM Performance Pathway.26 The APM Performance Pathway comprises a single, predetermined reporting measure set. The added simplicity is intended to serve as an incentive for providers to move away from traditional MIPS and toward APM participation.
Medicare Advantage (Medicare Part C)Unlike traditional Medicare, patients in an MA plan are required to seek care within a defined network of contracted providers. MA insurance carriers are paid capitated rates per beneficiary by CMS and can cover more services than traditional Medicare for their enrollees by recovering savings through risk contracts with care providers and network limitations. The contracted carriers may use value-based payment arrangements with providers that use the same or different performance measures recognized by CMS. The contractors must demonstrate a defined medical loss ratio (ie, revenues spent on direct patient care) or pay a penalty. As a means of oversight, MedPAC reviews the MA program, in addition to the Medicare Part D prescription drug program annually in a report to Congress.
Hierarchical Condition Category and Risk Adjustment FactorThe HCC risk adjustment model and Risk Adjustment Factor (RAF) score are used for risk-adjusted payments from CMS. The purpose is to ensure that plans and providers are appropriately compensated for beneficiaries with differing levels of health complexity. The HCC system categorizes a patient's medical conditions that are charted and coded with ICD-10-CM codes. The HCC risk adjustment model is used to adjust benchmark payment amounts to a Medicare Shared Savings Program (MSSP) ACO. The HCC codes, and demographic factors such as age and disability status, are input into calculating an RAF score. The RAF score is used to estimate the cost of care of an MA plan's beneficiaries and to adjust capitated payments to the insurance carrier. Incomplete ICD-10-CM coding can adversely affect payments to MSSP ACO providers and MA plans, whereas submitting ICD-10-CM codes without proper clinical documentation may be construed as violating the False Claims Act.27
Center for Medicare and Medicaid InnovationThe Center for Medicare and Medicaid Innovation (a.k.a. Innovation Center) was established by Congress in 2010 as part of the ACA.28 The Innovation Center oversees with CMS ways to improve healthcare quality and equity and reduce costs in Medicare, Medicaid, and the Children's Health Insurance programs. The Innovation Center supervises the creation, implementation, revision, continuation, and retirement of payment models that cross over in the various value-based Medicare Payment Programs.
Since its inception, the Innovation Center has tested numerous payment models including bundled payment programs such as Bundled Payment for Care Improvement and population-based models such as the Pioneer ACO Model. Input into the design of payment models is received from numerous public and private stakeholders, including the Health Care Payment Learning and Action Network and the MACRA-created Physician-Focused Payment Model Technical Advisory Committee.
While most payment models are voluntary, the Innovation Center has introduced a few mandatory pilot payment models which require participation from providers practicing in certain geographic regions. For example, the Comprehensive Care for Joint Replacement Payment Model mandates the participation of hospitals located in 34 metropolitan statistical areas in total joint arthroplasty of the lower extremity care episodes.
Success of Traditional Medicare Payment ModelsThe most studied of value-based care models are population of people ACO models. Short and long-term studies of the MSSP have found modest savings, ranging from under 1% to just over 6%.29 A CMS report noted that this payment model saved Medicare $1.8 billion in 2022 with approximately 63% of ACOs earning shared savings payments.30 The authors have remarked that it takes time for clinician groups and organizations to make the necessary changes for effective ACO participation; consequently, higher savings may be realized with longer ACO participation. However, complicating efforts at savings, there is no requirement or incentive for patients with traditional Medicare to seek care solely within the ACO provider sites.
The results of care episode payment models in achieving savings are more mixed with joint arthroplasty models (eg, Comprehensive Care for Joint Replacement Payment Model) showing the greatest potential for reduced spending. While many models have been found to achieve a reduction in gross spending, net spending (which includes incentive payments) has increased in some payment arrangements.29
Success of Medicare AdvantageThe Kaiser Family Foundation (KFF), an independent source for policy research, published a literature review that noted few differences between MA and traditional Medicare in beneficiary experience, affordability, utilization, and quality.29 In an analysis of 2021 data, KFF found that CMS paid more to MA plans for enrollees, on average, than their costs would be in traditional Medicare.31 In the same report, MA plans were discerned to have attained gross margins substantially higher than those achieved in commercial insurance and Medicaid-managed care plans.
The number of patients choosing MA plans has soared in recent years with intensive advertising and incentives. However, delayed payments from MA commercial insurers and high prior authorization denial rates are leading to a growing number of physician groups, hospitals, and health systems leaving MA plans. In parallel, provider-owned health insurance plans are entering into agreements with CMS to operate their own MA plans alone or in partnership with other insurance carriers and provider networks.
Medicare Requirements for HospitalsTo receive Medicare reimbursement, hospitals must follow the Medicare ‘Conditions of Participation,’32 a comprehensive and foundational set of operating requirements. Fundamental standards include physical environment; infection control and prevention; and nursing, medical staff, and patient rights. These provisions are the essential infrastructure of any hospital and are the basis of accreditation requirements by The Joint Commission, Det Norske Verita, and the Healthcare Facilities Accreditation Program.
Medicare Star RatingsThe Five-Star Quality Rating System was devised by CMS to help consumers compare hospitals, Medicare Part D prescription drug plans, MA insurance carriers, nursing homes, ambulatory surgery centers, home health agencies, hospice care, inpatient rehabilitation facilities, long-term care hospitals, dialysis facilities, and doctors and clinicians. The CMS ‘Care Compare’ data are available online for the public to view.33 The ratings are weighted using performance (ie, outcome and process) measures, cost, and other data that are submitted by providers to CMS in fulfillment of Medicare Payment Program reporting requirements. One star represents poorest observed performance, and five stars represent best observed performance.
The Future of MedicareThe Medicare program is faced with difficult challenges. The US population is aging along with increased complexities of disease management, the costs of health care continue to rise, waste and low-value care persist,12 critical access hospitals in some rural areas are closing, clinicians are advocating for equitable payment adjustments, and the Medicare Part A Trust Fund is headed toward insolvency. Unless the current structure of Medicare evolves, general revenues, payroll taxes, and Medicare enrollee dollars may not be able to adequately sustain the Hospital Insurance Trust Fund and Supplementary Insurance Trust Fund that help fund Medicare benefits.
Medicare has been instrumental in providing eligible adults access to medical care and in reducing racial and ethnic disparities related to insurance coverage and care access.34,35 Nevertheless, beneficiary inequities persist and additional improvements in population health are needed.36 CMS recently launched the National Quality Strategy and defined an approach called Rewarding Excellence for Underserved Populations, which will attempt to improve quality of care for all while avoiding penalties for clinicians who provide care to patients with notable social needs and complexities.37,38 The Area Deprivation Index was introduced by the Innovation Center into select payment models (eg, MSSP) to incentivize providers to increase their focus on disadvantaged po
留言 (0)