
記住我








Available online 1 May 2024
 Author links open overlay panel, , , , , , Highlights•
Author links open overlay panel, , , , , , Highlights•AS with normal flow (≥35 mL/m2), low gradient (mean gradient <40 mm Hg), and AVA ≤1.0 cm2 or AVAi ≤0.6 cm2/m2 (NFLG severe AS) represents a challenging clinical entity.
•A diagnostic algorithm to ensure no measurement errors and use of adjunctive data from cardiac computed tomography and magnetic resonance imaging may be useful for delineating moderate vs severe AS in these settings of divergent echocardiographic data.
•There are very limited trial data to guide management of this condition, and observational studies have shown inconsistent results.
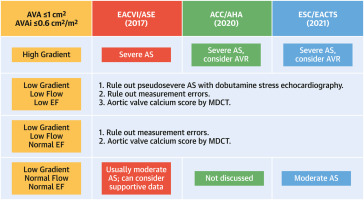
•ESC/EACTS 2021 guidelines and EACVI/ASE 2017 report that patients who meet criteria for NFLG severe AS usually have clinically moderate AS and should be managed as such. NFLG severe AS was not mentioned in the AHA/ACC 2020 guidelines.
•Ongoing trials of valve replacement vs surveillance in patients with moderate AS may provide supportive data on how to manage these patients with this challenging clinical entity.
AbstractPatients with normal-flow low-gradient (NFLG) severe aortic stenosis present both diagnostic and management challenges, with debate about the whether this represents true severe stenosis and the need for valve replacement. Studies exploring the natural history without intervention have shown similar outcomes of patients with NFLG severe aortic stenosis to those with moderate aortic stenosis and better outcomes after valve replacement than those with low-flow low-gradient severe aortic stenosis. Most studies (all observational) have shown that aortic valve replacement was associated with a survival benefit vs surveillance. Based on available data, the European Society of Cardiology/European Association for Cardio-Thoracic Surgery guidelines and European Association of Cardiovascular Imaging/American Society of Echocardiography suggest that these patients are more likely to have moderate aortic stenosis. This clinical entity is not mentioned in the American Heart Association/American College of Cardiology guidelines. Here we review the definition of NFLG severe aortic stenosis, potential diagnostic algorithms and points of error, the data supporting different management strategies, and the differing guidelines and outline the unanswered questions in the diagnosis and management of these challenging patients.
Section snippetsDefinitionPrecisely determining the severity of aortic stenosis (AS) using the echocardiographic parameters is not always simple and straightforward, as there is often inconsistency among the measures of AS severity (eg, mean gradient, peak velocity, aortic valve area [AVA], dimensionless index).1,2 Discordance between the mean gradient (or peak velocity) and valve area (or dimensionless index) is understandable in the setting of a low-flow state (ie, stroke volume index <35 mL/beat/m2) across a severely
DiagnosisEuropean Society of Cardiology (ESC)/European Association for Cardio-Thoracic Surgery (EACTS), EACVI/ASE, and American Heart Association (AHA)/American College of Cardiology (ACC) have all recommended primarily using echocardiography to assess the severity of AS with 3 parameters: mean transvalvular pressure gradient, peak transvalvular velocity, and AVA.1,3,4 When there is discordance among these parameters, an integrated approach should consider additional parameters: dimensionless index
Follow-upIn studies that evaluated the natural history of patients with different flow-gradient patterns of severe AS, most studies have shown better survival in patients with NFLG severe AS as compared with either LFLG or HG severe AS (Table 2).21,38, 39, 40, 41, 42, 43, 44, 45, 46, 47 In a meta-analysis including 9 studies and 3,065 patients where patients were censored at the time of AVR, patients with NFLG severe AS had a lower risk of all-cause mortality compared with those with HG severe AS
Role of aortic valve replacementEleven observational studies have examined the outcomes of patients with NFLG severe AS treated with AVR vs surveillance (Table 3).11,40, 41, 42,51, 52, 53, 54, 55, 56, 57 When these studies were analyzed using meta-analytic techniques, AVR was associated with a reduced risk of all-cause mortality vs surveillance58,59 with HRs of 0.48 (95% CI: 0.28-0.83; studies through 2015)58 and 0.41 (95% CI: 0.27-0.62; studies through 2020).59 These estimates are similar to the HRs for AVR in patients with
Guidelines discussion and unanswered questionsThe 2021 ESC/EACTS guidelines for the management of valvular heart disease indicate that patients with these indices consistent with NFLG severe AS (ejection fraction ≥50%, stroke volume index ≥35 mL/beat/m2, mean gradient <40 mm Hg, and AVA ≤1.0 cm2 [or AVA index ≤0.6 cm2/m2]) are usually more clinically similar to moderate AS and should be treated as such.4 These recommendations were based on studies that showed similar outcomes for patients with NFLG severe AS vs moderate AS21,38,39 and no
Funding Support and Author DisclosuresThis study was self-funded. Dr Huded has received consulting fees from Boston Scientific; and has received grants from Abbott. Dr Saad has received consulting fees from Boston Scientific. Dr Chhatriwalla has been a proctor with Edwards Lifesciences, Medtronic; has been on the Speakers Bureau with Abbott Vascular, Edwards Lifesciences, and Medtronic; and has received grants from Boston Scientific. Dr Abbott has received grants from Boston Scientific and Microport; and has received consulting
View full text© 2024 by the American College of Cardiology Foundation. Published by Elsevier.
留言 (0)