Study design and participants
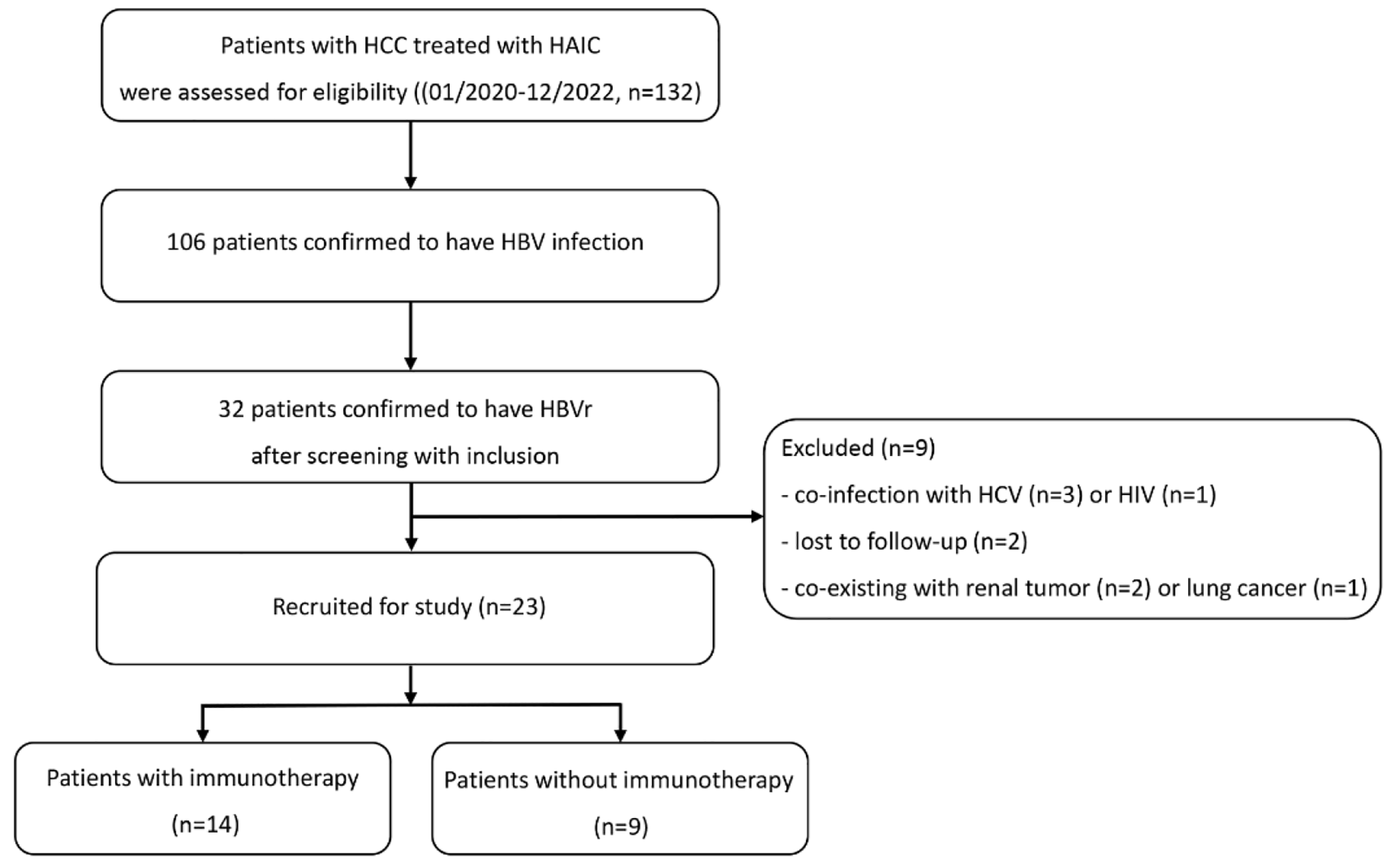
A retrospective analysis was carried out on patients with HCC at our institution between January 2021 and June 2023. In this study, the requirement for written informed consent was waived, and prior approval from the Institutional Review Board was obtained before beginning the study.
The inclusion criteria for this study were as follows: (1) individuals over the age of 18 with advanced primary unresected HCC, confirmed through pathological or clinical diagnosis, and in accordance with the guidelines set forth by the American Association for the Study of Liver Diseases (AASLD) [21]; (2) patients solely treated with HAIC or a combination of HAIC and immunotherapy, without undergoing surgical operations or any other local treatments until reaching the primary endpoint during the study period; (3) individuals tested positive for HBV infection, specifically HBsAg, or tested negative for HBsAg but positive for anti-HBc; (4) patients diagnosed with HBVr based on the provided definition; (5) patients with regular monitoring of HBV DNA and liver function during hospitalization and follow-up, as recommended by the treating physician; (6) patients with presence of at least one measurable lesion; (7) patients with liver function classified as Child-Pugh Class A or B without ascites; and (8) an Eastern Cooperative Oncology Group (ECOG) performance status of 0–2.
Participants who met any of the following criteria were excluded from the study: co-infection with other hepatotropic viruses or HIV, lost to follow-up, obstructive jaundice, concurrent malignant comorbidities, serious non-malignant illnesses, history of hepatotoxic medication within eight weeks prior to HCC treatment [10], or a history of corticosteroid administration.
HAIC treatment
The patients underwent a three-week cycle regimen, involving the intra-arterial insertion of a catheter into the hepatic artery, and a microcatheter into the feeding arteries of the tumor. The HAIC protocol was used for the administration of mFOLFOX6 treatment, which included infusion of oxaliplatin, calcium folinate and 5-fluorouracil (5-FU) (with a 10-minute interval after calcium folinate) on the first day at a dose of 85 mg/m2, 200 mg/m2 and 250 mg/m2 (I.V. for 15 min), respectively, followed by continuous arterial infusion of 5-FU for 46 h at a dose of 2,400 mg/m2.
Following the procedure, the catheter and sheath were removed and a pressure bandage was applied. The HAIC procedure was repeated until the tumor remained stable or progressed, or if intolerable toxicity was observed. Patients had the option to discontinue treatment if they declined the protocol. The HAIC treatment would only be initiated if the viral load decreased below the level of 105 IU/ml.
Immunotherapy
The immunotherapy drugs, tislelizumab, camrelizumab, sintilimab, and atezolizumab, were given to patients through IV infusion every three weeks, following the dose prescribed by the doctor. In case of disease progression or intolerable adverse events (AEs), the administration of immunotherapy was stopped. To manage symptoms, treatments like glucocorticoids or immune-suppressant agents were given, depending on the severity and the affected organs.
Antiviral therapy
Based on the 2017 guidelines from the European Association for the Study of the Liver (EASL) [22], individuals diagnosed with chronic hepatitis B, either hepatitis B ‘e’ antigen (HBeAg) -positive or -negative, with HBV DNA levels exceeding 2,000 IU/ml, serum alanine aminotransferase (ALT) greater than the upper limit of normal (reference range less than 40 IU/L), and/or displaying moderate liver necroinflammation or fibrosis, should undergo antiviral therapy. Moreover, patients with compensated or decompensated cirrhosis requiring treatment should receive antiviral therapy regardless of their HBV DNA or ALT levels. If the patient was previously on antiviral therapy before hospitalization, the treatment was continued.
In our hospital, there were three types of oral antiviral drugs (nucleoside analogs) available: entecavir (ETV), tenofovir disoproxil fumarate (TDF), and tenofovir alafenamide fumarate (TAF).
To optimize the efficacy of antiviral treatment, patients who had previously received ETV or TDF before the onset of HBVr were additionally administered TAF, while those who had previously received TAF before the HBVr were additionally given ETV [23]. Concurrently, internal medicine treatment was administered. The treatment plan was modified as necessary until the HBV DNA became undetectable or the viral load decreased to the same level as before the HAIC.
Definition
The primary endpoint was the hepatic AEs.
HBVr was defined as the initial detection of HBV DNA or a more than 10-fold increase (1 log10) in HBV DNA levels compared to the baseline value before HAIC treatment in individuals who have the HBsAg protein present. In the case of individuals who have cleared the infection (negative for HBsAg but positive for anti-HBc), reactivation is determined by the reversal of seroconversion to a positive HBsAg status [24].
Hepatitis was characterized by a threefold increase or more in the serum ALT levels, surpassing the reference range of 40 IU/L, or an absolute increase in ALT levels exceeding 100 IU/L. HBV-related hepatitis was defined as hepatitis occurring during or after HBVr, without any concurrent acute viral hepatitis infection or systemic disease. The classification of hepatitis was conducted by the treating physician and corresponding authors, considering clinical manifestations, laboratory tests, and imaging examinations. The categories included HBV-related, drug-induced, liver lesion progression-related, and immune-related hepatitis [25, 26].
The criteria for determining hepatic AEs were established based on the guidelines provided by the Common Terminology Criteria for AEs version 5.0 [27]. Grade 3 hepatitis was characterized by ALT levels greater than 5 times the upper limit of normal (ULN) to 20 times the ULN if the baseline levels were within normal range, or more than 5 to 20 times the baseline levels if the baseline levels were abnormal. Grade 4 hepatitis was defined as ALT levels exceeding 20 times the ULN if the baseline levels were within normal range, or more than 20 times the baseline levels if the baseline levels were abnormal.
Antiviral prophylaxis was described as the administration of antiviral treatment (nucleoside analogs) prior to and during HAIC treatment.
Follow-up
Patients were monitored until the discontinuation of HAIC, occurrence of all-cause mortality, follow-up failure, or completion of the study, whichever came first.
The monitoring of patients comprised of physical examinations, laboratory assessments, and imaging procedures. Laboratory assessments, which encompassed liver function evaluations, screening for tumor markers, and tests for HBV (hepatitis B virus) (HBV serology and quantification of HBV DNA), were performed at three-week intervals during HAIC and every two months after therapy completion. Imaging procedures, specifically CT or MRI scans, were carried out every three months within the initial two years and every six months thereafter. Lung metastasis was confirmed through chest radiography conducted every six months. Additional imaging tests, such as chest CT, bone scintigraphy, and PET, were only conducted if clinically indicated.
Statistical analysis
The demographic data, including mean, standard deviation, and percentage, were analyzed with the statistical software SPSS version 26.0. The data were presented in the form of means and standard deviations or medians and ranges. The comparison of categorical variables involved the utilization of the X2-test or Fisher’s exact test when appropriate, while the comparison of continuous variables utilized the Mann-Whitney U test or Wilcoxon Signed Rank test. Statistical significance was determined with a two-tailed P value of less than 0.05. Graphs were created using GraphPad Prism 8.0 (GraphPad Software Inc., San Diego, CA, USA).




留言 (0)