
記住我
Vibration is a common occurrence in our daily lives. It can have therapeutic effects in conditions such as osteoarthritis or cancer when experienced in moderate amounts locally or throughout the body. However, prolonged and excessive exposure to vibration can harm the human body [1–3]. Long-term exposure to hand-transmitted vibration (HTV) from operating vibration tools can lead to hand-arm vibration disease (HAVD), which is the worst circumstance. HTV can be found almost everywhere, such as manufacturers, drivers, grinding operators, polishing operators, and so on. The incidence of HAVD has been increasing in many countries in recent years [4]. HAVD is a systemic disease primarily affecting the nerves and peripheral microcirculation in the hands. Its characteristic change in the vascular component is vibration-induced white finger (VWF), also known as occupational Raynaud’s phenomenon (RP) [5,6]. VWF can make the afflicted fingers periodically blanch when a cold attacks. The attacks of VWF are usually accompanied by a lack of sensation and frequent pain when the digital circulation returns.
Although HAVD can negatively impact the mental and physical health of workers who are exposed to HTV, numerous questions remain unsolved. The exact pathogenesis of HAVD remains unclear, and a specific diagnostic indicator is needed [7].
In China, the diagnosis of HAVD involves conducting cold provocation and operating white finger induction tests based on the current standard (GBZ 7-2014) ‘Diagnosis of occupational hand-arm vibration disease’. However, the test results may vary among individuals. Additionally, we utilize electromyography to identify neurogenic damage in sensory conduction velocities (SNCV) and motor conduction velocities (MCV) as an auxiliary method. However, none of these techniques can quantitatively monitor vascular functional deficit [8,9]. Many countries such as Germany, England and Japan have recommended finger SBP (FSBP) as a diagnostic indicator of HAVD [10]. FSBP measurements, standardized internationally by the International Organization for Standardization (ISO) in 2005, perform well in detecting fingertip circulatory disorders and ischemic injuries [11,12]. Several scholars have proved that FSBP measurements have high diagnostic value in VWF diagnosis, but relevant research in China is insufficient [13]. To provide massive evidence regarding FSBP’s medical application and regional-specific reports, we conducted this study based on Guangdong province, which is taking the lead in the manufacturing industry in China. The labor of a golf goods factory was chosen as the overall sample.
Therefore, we measured the FSBP of specimens and investigated its application value in determining the presence of VWF. We compared the FSBP data of each finger, drew a primary conclusion about the most suitable diagnosis index, and then discussed its application value in HAVD diagnosis. This study aimed to compare the accuracy and specificity of FSBP indexes for the diagnosis of HTV-induced VWF in a large sample of workers who used vibrating tools and determined the best index that can be applied to discriminate healthy workers and VWF workers. We also aimed to obtain normal limit values for the FSBP index.
Materials and methods ParticipantsA nonrandomized concurrent controlled trial was conducted. A total of 100 participants who came from one golf product factory were equally divided into two groups. The 50 subjects who used hand-held vibratory tools and had been working in metal grinding posts for over 2 years formed the VWF group, and 50 nonmanual workers formed the control group. All participants in the control group were not experiencing any symptoms consistent with RP. All VWF patients were diagnosed by qualified doctors. All participants were right-handed. Subjects in the VWF group were diagnosed at the Guangdong Provincial Occupational Disease Prevention Hospital from February 2018 to December 2020. Workers with primary Raynaud’s disease, systemic lupus erythematosus, scleroderma, liver and kidney diseases, diabetes, heavy metal poisoning, peripheral nervous system diseases and hand injuries were excluded. All subjects were male.
All participants were not hand-injured. All of them did not take vasoactive therapy within 2 weeks. We also ensured that none of the participants had exercised vigorously or been exposed to stimulants (e.g. caffeine, alcohol and nicotine) over 3 h before the examination.
The study was reviewed and approved by the medical ethics committee of Guangdong Province Hospital of Occupational Disease Prevention and Treatment (Approval code: GDHOD MEC2010038), and all participants gave informed consent.
Occupational health questionnairesWell-trained investigators carried out a one-to-one survey of all participants. The questionnaire was designed by ourselves. Basic information (e.g. gender, height, weight, age, etc.), occupational history (e.g. post, length of service, occupational hazard factors, protection measurements, etc.), living habits (e.g. smoking, drinking, commuting transportation, etc.), basic health status (e.g. family history, personal history, etc.), conscious symptoms (e.g. hand numbness, pain, distension, stiffness, etc.), white fingers related information (e.g. the conditions with attacks, the time of occurrence, and the incidence locations of VWF) were included in the main contents. Two well-trained doctors entered the raw data into the Epidata software (version 2.0) for further analysis.
Only if a participant who had been smoking less than 6 months or had not smoked more than six packages was considered a nonsmoker. Participants who had not been drinking over half a bottle of beer were supposed to be nondrinkers.
Finger systolic blood pressure measurementsWe measured FSBP following the provisions of the International Organization of Standardization (ISO/DIS 14835-2) [17]. We used the HVLab plethysmograph (ISVR, Southampton University). Before the FSBP measurements, all participants had to avoid exposure to HTV for over 24 h and smoking and drinking for 12 h. The cold provocation test or VWF induction test had to finish over 3 h before FSBP measurements. The room temperature we set for the measurements was 20 °C ± 1 °C, and participants acclimated in the test room for more than 30 min in a seated position with their hands at roughly heart level.
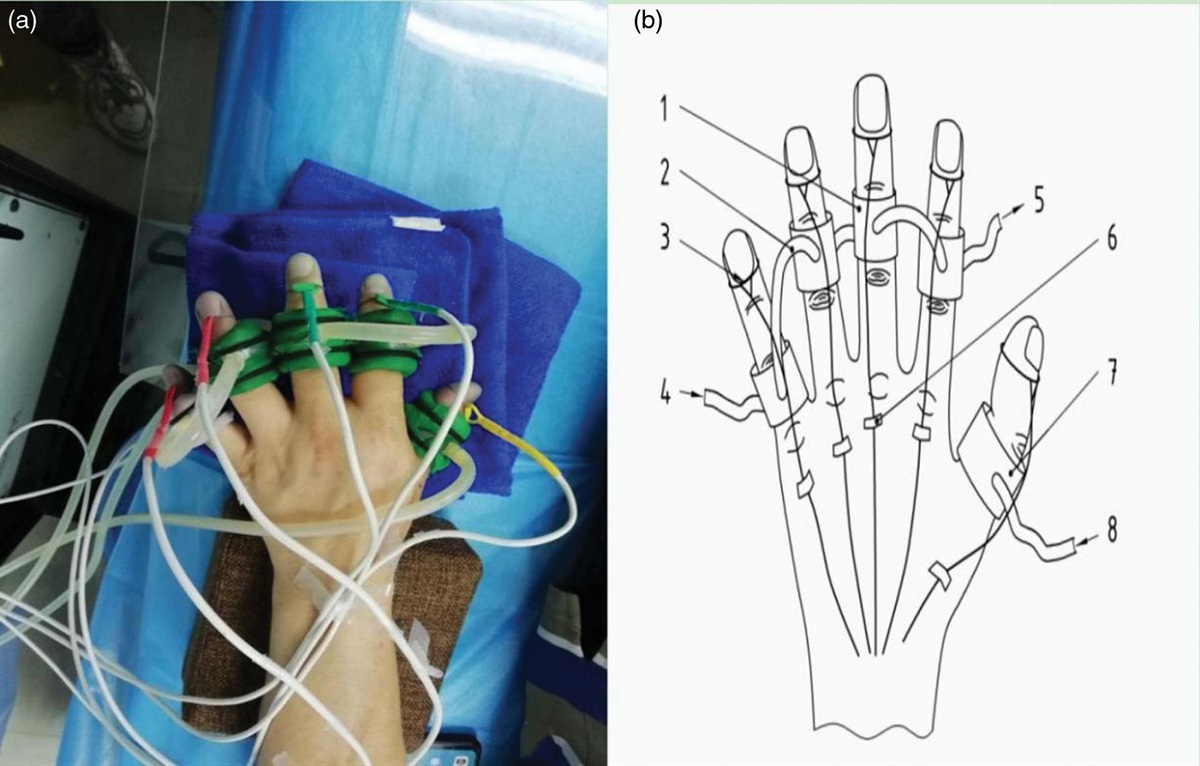
The FSBP of the fingers in their right hands was measured simultaneously, while the thumb was used as the reference point. How to set up the cuffs and strain gauges is shown in Fig. 1. In brief, a separate air cuff was put around the thumb, and water-perfusable cuffs were positioned around the mid-phalanx of each finger. Then, the mercury strain gauges were placed at the root of the cuffed fingers’ nails. The tips were compressed to reduce blood volume, and perfusion cuffs were perfused with thermostated water. The cuff pressure was decreased at a rate of 0.5 mmHg/s after 5 min of ischemia. The measurement pressure was 150–260 mmHg. The second knuckles of the other four fingers (index, middle, ring and little finger) were stimulated with 30 and 10 °C water for 5 min. The cuff inflation pressure captured when arterial inflow returned was recorded as FSBP30 and FSBP10. Percentage changes (%FSBP) were calculated by the formula below, and the results were recorded as the FSBP index. Participants whose %FSBP was lower than 80.0% were considered abnormal in FSBP measurements.
 Fig. 1:
Fig. 1: Setup for FSBPs measurements using strain-gauge plethysmography. (a) Photo of FSBP setup in practice; (b) Diagram of setup.
FSBP Index=FSBPt,10FSBPt,30−(FSBPref,30−FSBPref,10) ×100.0%
FSBP index means %FSBP of the test finger after thermal stimulation at 10 °C;
FSBPt,10°C means the FSBP measured on the test finger after thermal stimulation at 10 °C;
FSBPt,30°C means the FSBP measured on the test finger after thermal stimulation at 30 °C;
FSBPref,30°C means the FSBP measured on the thumb after thermal stimulation at 30 °C;
FSBPref,10°C means the FSBP measured on the thumb after thermal stimulation at 10 °C.
Statistical analysesData analysis was performed by SPSS software (version 21.0, SPSS Inc., Chicago, Illinois, USA). We presented statistics corresponding to a normal distribution as mean and SD. In small samples, statistics were presented as mean and SEM. Student T-test and Fisher’s exact test were used to compare FSBP or %FSBP between two or multiple groups. A paired sample t-test was used to compare the %FSBP of different fingers. The criterion for statistical significance was P < 0.05 (two-tailed).
The diagnostic accuracy of the FSBP test was evaluated by a receiver operating curve (ROC). Hanley’s method was used in the comparison of the areas under the ROC curves. The fitting degree of the linear regression model was evaluated by the coefficient of determination (R2), while the significance of each model was calculated by analysis of variance (ANOVA).
Results Basic and vibration-induced white finger-related statistics of subjectsThe mean age of the control group was 37.9 ± 7.6 years. The mean of their BMI was 23.6 ± 3.2 kg/m. In total 33 had a smoking history (82.0%), while 34 had a history of alcohol (68.0%). The VWF group’s mean age was 38.8 ± 6.4 years, and their mean BMI was 24.1 ± 3.0. We found no age, BMI, or education differences between groups. The VWF group’s service length was significantly longer than the control group (P = 0.014). The incidence of finger numbness, fibrillation, swelling and arm weakness in VWF was higher than that in the control group (P < 0.05). Notably, all VWF patients had the symptom of finger numbness. The other details of those participants are shown in Supplementary Table 1, Supplemental digital content 1, https://links.lww.com/BPMJ/A215.
Comparison of finger systolic blood pressure between two temperaturesThe Q-Q graphs of the FSBP of each finger in two temperatures were roughly on a straight line, which showed that they were all normal variables. The FSBP of the middle and ring finger at 10 °C were lower than those at 30 °C in the control group (P < 0.001). In the VWF group, the FSBP of the thumb and ring finger under 10 °C was lower than 30 °C (P < 0.01). On the other hand, FSBP in the VWF group was lower than the control group, especially at 10 °C (P < 0.05 in all fingers), while only thumb and index finger FSBP was found lower in the VWF group at 30 °C (P < 0.001). At 10 °C, the FSBP of all fingers in the VWF group was lower than those of the control group (P < 0.05). Detailed data is shown in Table 1.
Table 1 - Finger SBP in 10 °C and 30 °C of vibration-induced white finger patients and healthy control Group Temperature FSBP Thumb finger little finger Index finger Middle finger Ring finger Control group 10 124.8 ± 25.6 127.3 ± 14.0 109.6 ± 19.3a 114.6 ± 15.7a 126.1 ± 19.8 30 114.1 ± 20.2 127.5 ± 27.2 113.0 ± 20.3 101.5 ± 23.2 100.1 ± 23.0 VWF group 10 111.8 ± 26.3c 96.2 ± 36.1c 97.5 ± 29.9b,c 93.3 ± 11.5b,c 100.3 ± 21.9c 30 105.1 ± 20.8d 96.5 ± 19.9d 107.0 ± 27.4 108.3 ± 35.6 104.1 ± 29.8FSBP, Finger SBP; VWF, vibration-induced white finger.
aSignificant difference in comparison of FSBP between 10 °C and 30 °C in control group;
bSignificant difference in comparison of FSBP between 10 °C and 30°C in the VWF group;
cSignificant difference in comparison of FSBP between the control group and VWF group at 10°C;
dSignificant difference in comparison of FSBP between the control group and VWF group at 30°C;
According to the %FSBP calculated by the above formula, the %FSBP of the index, ring and little finger in VWF was significantly lower than that in the control group (P < 0.05). The detailed data are shown in Table 2. The results were consistent with the FSBP results above.
Table 2 - %FSBP value in vibration-induced white finger patients and healthy control Group N Index finger Middle finger Ring finger Little finger Control group 50 89.2 ± 15.8 83.3 ± 12.3 97.2 ± 17.5 108.7 ± 23.1 VWF group 50 79.9 ± 19.5a 77.3 ± 19.4 79.6 ± 28.9a 83.5 ± 20.6a Z −2.316 −0.931 −5.563 −5.880 P 0.021 0.352 <0.001 <0.001VWF, vibration-induced white finger.
aSignificant difference in comparison of %FSBP between the VWF group and control group.
We further studied the occurrence of abnormal %FSBP, which was lower than 80.0%, the results are shown in Table 3. Interestingly, there were some participants whose %FSBP was abnormal in the healthy control group. Among them, there were nine abnormal cases in index fingers (18.0%), 32 in middle fingers (64.0%), 13 in ring fingers (26.0%) and four in little fingers (8.0%). In the VWF group, the ring finger obtained the most abnormal reports (78.0%) followed by the little finger (36.0%). The abnormal index, ring, and little finger rates in VWF patients were higher than in healthy control (P < 0.05).
Table 3 - Abnormal rate of %FSBP in vibration-induced white finger patients and healthy control Group N Index finger Middle finger Ring finger Little finger Mount (N) rate (%) Mount (N) rate (%) Mount (N) rate (%) Mount (N) rate (%) Control group 50 9 18.0a 32 64.0 13 26.0a 4 8.0a VWF group 50 22 44.0 25 50.0 39 78.0 32 64.0 X 2 7.901 1.99 27.08 31.27 P 0.005 0.157 <0.001 <0.001VWF, vibration-induced white finger.
aSignificant difference in comparison of abnormal rate between control and VWF.
We could preliminarily deduct that the %FSBP of the index, ring and little finger might have a specific application value for VWF detection. So, we performed an ROC curve analysis, shown in Fig. 2. The area under curve (AUC) of the index finger, middle finger, ring finger and little finger were 0.542, 0.640, 0.902 and 0.737, respectively. Other parameters are shown in Table 4.
Table 4 - Parameters of %FSBP diagnostic accuracy to distinguish vibration-induced white finger Fingers AUC (95% CI) Cutoff (%) Sensitivity (%) Specificity (%) Youden Index +LR −LR Index 0.542 (0.324–0.759) 79.92 53.33 73.33 0.266 2.000 0.636 Middle 0.640 (0.428–0.852) 76.68 53.33 86.67 0.399 4.000 0.538 Ring 0.902 (0.769–1.000) 77.60 86.67 86.67 0.732 6.500 0.154 Little 0.737 (0.556–0.919) 96.58 53.33 73.33 0.266 1.800 0.636±LR, positive/negative likelihood ratio.
 Fig. 2:
Fig. 2: Diagnostic accuracy of each finger’s %FSBP.
Assessments of effects of %FSBP influence factorsWe conducted a multiple linear analysis employing VWF or not as the dependent variable and age, duration of service, smoking, drinking, BMI, as well as %FSBP of each finger as the independent variables. We used’ stepwise’ to enter those variables into the regression model. Finally, the %FSBP of four fingers was all entered into the analysis, and we came out with four models. The parameters of those regression models are shown in Table 5. We chose Model 4 as the regression model for its great quality (R2 = 0.624) and capacity for fitting the relationship between variables (F = 39.454; P < 0.0001 in ANOVA). So the regression equation we obtained was:y−=4.515−0.822x1−1.433x2−1.783x3−0.623x4. x1-4 stood for %FSBP of four fingers. The normalized beta showed the influence of the independent variables (%FSBP of four fingers) on the dependent variable (VWF or not). %FBSP of the ring finger (normalized beta = −0.723) had the greatest effects on VWF.
Table 5 - Selection of vibration-induced white finger diagnosis indexes by linear regression analysis Model Variables that the model contains R 2F2, index finger; F3, middle finger; F4, ring finger; F5, little finger; β, regression coefficient.
According to the present analysis, the ring finger performed well in ROC and regression analysis, so we chose it to analyze further. The association of bad living habits and %FSBP of the ring finger are shown in Table 6. %FSBP of the VWF group was lower than the control group in smokers or nonsmokers (P = 0.009, 0.002). %FSBP of drinkers in the control group was higher than that in the VWF group (P = 0.002). The commute results were homologous compared to VWF and the control group (P = 0.003). Bad living habits-induced change of %FSBP was NS (P > 0.05).
Table 6 - Effects of living habits on %FSBP (mean ± SEM) Group Control VWF N %FSBP N %FSBP Smoking Smokers 41 98.39 ± 2.83a 34 81.95 ± 5.85 Nonsmokers 9 91.58 ± 4.68b 16 74.44 ± 2.72 Alcohols Drinkers 34 95.55 ± 2.97c 33 77.29 ± 4.82 Nondrinkers 16 100.60 ± 4.50 17 83.93 ± 7.62 Commutes to work Cyclists 33 97.98 ± 3.40d 39 79.36 ± 4.71 Bus/car/walk 17 95.57 ± 3.18 11 80.22 ± 8.49aSignifican difference from VWF workers who had a history of smoking.
bSignificant difference from VWF workers who didn’t have a history of smoking.
cSignificant difference from VWF workers who had a history of drinking.
dSignificant difference from VWF workers who went to work by cycling.
Regarding the other three fingers, no significant evidence was found in the comparison between nonsmokers/smokers, nondrinkers/drinkers and cyclers/noncyclers in the VWF or control group.
DiscussionOur current study has investigated occupational health characteristics and measured the %FSBP values between HTV-exposed workers diagnosed with VWF and workers without HTV exposure. We further analyzed the results and evaluated the diagnostic value of %FSBP in VWF. As an indirect indicator of finger blood flow, the measurement of FSBP during cold provocation has been recommended as a suitable test for identifying the cold-induced vasospasm of VWF [14,15,16]. Although the appearance of VWF is transient, FSBP measurements can still determine whether blood vessels are damaged [17].
Our study took place in Guangdong Province. Dubbed the ‘world’s factory’, southern China’s Guangdong Province is home to nearly 3 million industrial companies. Until now, studies about FSBP applications in China were in urgent need. So our study, which took place in Guangdong province, has great practical significance. Our study can reveal the test characteristics in specific regions compared with other places.
Our study shows that the FSBP of the four fingers of the participant’s dominant hand in the VWF patient group is lower than the control group (P < 0.01). This phenomenon suggests that the peripheral microcirculation function of fingers in the VWF group was damaged after cold provocation, and the contractile and diastolic factors secreted by blood vessels in the fingers are unbalanced. The contractile factor dominates this process, which leads to an increase in finger vessel contraction and stenosis of the vascular lumen, and then the blood flow of blood vessels decreases [18]. This theory can explain why %FSBP falls faster than that measured before cold stimulation. Meanwhile, the results of the comparison between 10 °C and 30 °C did prove our deduction again.
On the other hand, some %FSBP abnormal phenomenon in healthy control existed. The most abnormal case was found on the middle finger (64.0%), followed by the ring finger (26.0%) and index finger (18.0%). It may be because those fingers are liable to be hurt in daily work. It may also be because of the specific usage of the vibrating tools and working positions. The AUC results (AUCindex = 0.542, AUCmiddle = 0.640) also reflect these facts. The possible mechanisms Carpal tunnel syndrome attacks certain office employees who spend much time on computers. Thumb, index, middle and ring finger sensory nerve disruption can occur due to median nerve dysfunction [19,20]. According to existing findings, the middle finger performs worse on sensory and electrophysiological tests than other fingers, indicating that more extensive nerve damage may be produced [21].
The comparison between the abnormal rates of the two groups shows the index, ring and little finger in the VWF group were higher than those in healthy participants (P < 0.05). The abnormal rate of the index and little finger shows a great difference (44.0% vs.18.0%, 64.0% vs.8.0%), indicating that %FSBP < 80.0% as the criterion can enhance the discriminability of VWF detection. Compared with the cold water provocation test, which is the overwhelming method being used in China, FSBP measurements can fix the problem of low sensitivity and specificity well [22].
Unlike the index and little finger, the abnormal rate of ring finger leads in the VWF group (78.0%). Combining the ROC results and linear regression results of the ring finger (AUC = 0.902; β = −1.783), we suggest using the %FSBP of the ring finger as the main parameter of FSBP measurement. As previously stated, the FSBP test was used to guide diagnostics and medical decisions in China. In the laboratory practice of workplace health surveillance, an abnormal FSBP test result may be used as a criterion for either removing symptomatic workers from vibration exposure or following up on a symptomatic subject with objective signs of preclinical RP at the cold test at shorter intervals. The results of a pathological FSBP test enable the development of a clear diagnosis of VWF in people with both a credible history of finger-blanching attacks and a work history of HTV exposure. Our study primarily discovered the relationship between living habits and %FSBP. No results can prove that the %FSBP of participants who drank, smoked or went to work by cycle differs from other participants in both groups. Their relationship needs to be discovered in larger-scale samples and long-term follow-up studies.
Referring to previous studies, some used 60.0% as the cutoff value of %FSBP [9,23]. With the perfection of the research design, a series of Japanese researchers used 75.0%, 80.0%, and 90.0% as the discriminating threshold and acquired great performance in diagnostic value (sensitivity: 73.9, 82.0 and 80.0; specificity: 82.5, 90.0 and 77.0) [24–26]. In our study, we chose 80.0% as the discriminating threshold value and performed well on the ring finger (sensitivity: 86.67%; specificity: 86.67%). Regarding the other three fingers that presented low sensitivity in AUC analyses, one possible explanation is that the patients in studies with higher sensitivity might have a longer course of disease or be diagnosed with more severe HAVD [23]. In FSBP tests, sensitivity can be relatively low in distinguishing mild VWF [16,27].
Even though we conducted the FSBP test in strict conformity with the procedures that ISO 14835-2:2005 recommends, the differences in the climate of study places should not be ignored. Thus, foreign studies may not be suitable for Chinese subtropical regions. On the other hand, we only operated FSBP measurements in VWF patients and healthy controls without HTV exposure history. In further study, we can conduct measurements in different levels of HAVD patients or patients being classified by differences in clinical features.
ConclusionsOur results have proved that VWF is linked to the decrease of FSBP. Our results have also proved that the FSBP measurements are instrumental and feasible for diagnosing VWF in China. Measuring the %FSBP of the ring finger is recommended as the possible indicator, which can reflect the presence of vibration-induced vascular damage to some extent.
AcknowledgementsThe datasets generated during or analyzed during the current study are available from the corresponding author on reasonable request.
Conflicts of interestThere are no conflicts of interest.
References 1. Burdorf A, Hulshof CTJ. Modelling the effects of exposure to whole-body vibration on low-back pain and its long-term consequences for sickness absence and associated work disability. J Sound Vib 2006; 298:480–491. 2. Matsumoto T, Mukohara A. Effects of whole-body vibration on breast cancer bone metastasis and vascularization in mice. Calcif Tissue Int 2022; 111:535–545. 3. Pahl A, Wehrle A, Kneis S, Gollhofer A, Bertz H. Feasibility of whole body vibration during intensive chemotherapy in patients with hematological malignancies - a randomized controlled pilot study. BMC Cancer 2018; 18:920. 4. Krajnak K. Health effects associated with occupational exposure to hand-arm or whole body vibration. J Toxicol Environ Health B Crit Rev 2018; 21:320–334. 5. Gemne G. Diagnostics of hand-arm system disorders in workers who use vibrating tools. Occup Environ Med 1997; 54:90–95. 6. Bovenzi M. Criteria for case definitions for upper limb and lower back disorders caused by mechanical vibration. Med Lav 2007; 98:98–110. https://www.scopus.com/inward/record.uri?eid=2-s2.0-34247541622&partnerID=40&md5=f372b4465ca8e0e81f96c898c9c83f7a. 7. Fedorovich AA, Rogoza AN, Chikhladze NM. Characteristics of the functional state of arteriolar and venular skin microvessels in patients with essential arterial hypertension. Microvasc Res 2014; 93:105–113. 8. Chen Q, Lin H, Xiao B, Welcome DE, Lee J, Chen G, et al. Vibration characteristics of golfclub heads in their handheld grinding process and potential approaches for reducing the vibration exposure. Int J Ind Ergon 2017; 62:27–41. 9. Bovenzi M. Finger systolic pressure during local cooling in normal subjects aged 20 to 60 years: reference values for the assessment of digital vasospasm in Raynaud’s phenomenon of occupational origin. Int Arch Occup Environ Health 1988; 61:179–181. 10. Su AT, Maeda S, Fukumoto J, Miyai N, Isahak M, Yoshioka A, et al. A cross sectional study on hand-arm vibration syndrome among a group of tree fellers in a tropical environment. Ind Health 2014; 52:367–376. 11. Nielsen SL. Raynaud phenomena and finger systolic pressure du
留言 (0)