
記住我

Antipsychotics are commonly used in the treatment of acute psychosis and psychotic symptoms of severe mental illness (SMI) such as schizophrenia or bipolar disorder. Therapeutic drug monitoring (TDM) of antipsychotic blood levels is sometimes applied to optimize individual therapy. By determining the individual blood concentration of antipsychotics in 1 or more samples, more information about the absorption, distribution, metabolism, and excretion of the drug in individual patients is obtained.
The Arbeitsgemeinschaft fur Neuropsychopharmakologie und Pharmakopsychiatrie published in 2017 an updated guideline with recommendations regarding therapeutic drug monitoring in neuropsychopharmacology.1 In their guideline, several situations are outlined in which TDM of antipsychotics is recommended. In general, TDM is used for dose titration and prevention of a relapse. In addition, in specific situations like insufficient response or adverse drug reactions at a therapeutic dose of an antipsychotic, suspicion of noncompliance or possible drug-drug interactions, TDM is recommended.1
Currently, TDM is usually performed by measuring drug concentrations in venous blood samples collected by antecubital phlebotomy, even though this technique contains several disadvantages. By antecubital venipuncture, a relatively large blood sample of several milliliters is collected and the sampling technique is quite invasive.2,3 In addition, trained medical personnel is required to collect these blood samples.2 As specific equipment for preparing serum or plasma is required, psychiatric patients often have to go to a medical center for venous blood sampling. This is not only a burden for the patient but also impossible in certain remote rural areas. Furthermore, timing of blood sampling in relation to drug intake needs to be coordinated for a reliable interpretation of the drug concentration and this can often not be achieved in outpatients. Refrigerated storage and the transport of blood or serum tubes are also cumbersome and expensive.
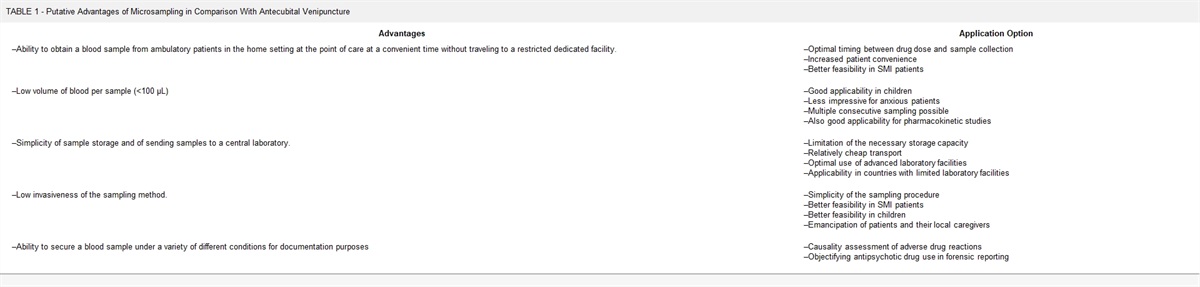
Because the sensitivity of analytical equipment has been improved over the past decades, the required sample volume for biomarker detection became significantly smaller. This has led to a growing interest in the development of microsampling techniques.4 Microsampling techniques are minimally invasive sampling techniques focusing on the collection of small sample volumes (<100 μL) of body fluids like blood or plasma.4,5 Most of these techniques are suitable for home sampling to decrease patient burden. Advantages of microsampling techniques are summarized in Table 1.
TABLE 1 - Putative Advantages of Microsampling in Comparison With Antecubital Venipuncture Advantages Application Option –Ability to obtain a blood sample from ambulatory patients in the home setting at the point of care at a convenient time without traveling to a restricted dedicated facility. –Optimal timing between drug dose and sample collectionSeveral microsampling techniques for therapeutic drug monitoring of a wide range of drugs are developed to date.4,5 Dried blood spot sampling is the oldest and best studied technique so far. This method is already available for several groups of drugs, such as antidiabetic drugs,6 antiepileptic drugs,7,8 immunosuppressants,9,10 tuberculosis drugs,11–13 and psychoactive drugs.14,15
More recently developed microsampling techniques for TDM are volumetric absorptive microsampling (VAMS), dried plasma spots, plasma extraction cards, and capillary microsampling methods.4,16
Before one of these techniques can be used for TDM in daily practice, the method must be developed for this specific drug, preferably according to international standards.17,18 This includes establishing the selectivity, reproducibility, linearity, precision, recovery, and stability of the technique for the specific drug. In addition, a clinical validation study for implementation of a method in daily practice is highly recommended to gain confidence in the method by clinicians.19
The aim of this review is to summarize the currently available microsampling techniques for antipsychotic drugs in blood, serum, or plasma and to evaluate if these techniques are already sufficiently validated for application in TDM in daily practice.
METHODS Literature SearchesNo specific filters were used in selecting the records. The electronic databases PubMed and EMBASE were used for literature search. PubMed (NIH/NLM platform) and Embase (Elsevier platform) were searched, for the last time on January 1, 2024. MEDLINE (NIH/NLM platform) was searched with: ((Antipsychotic Agents) OR (antipsychotic agent*) OR (antipsychotic drug*) OR (antipsychotics) OR (neuroleptics) OR (neuroleptic agent*) OR (neuroleptic drug*) OR (Antipsychotic Agents)) AND ((Drug Monitoring) OR (monitor*) OR (determin*) OR (level*) OR (concentration*) OR (quantif*) OR (quantita*) OR (TDM) OR (identif*)) AND ((Dried Blood Spot Testing) OR (dried blood spot*) OR (dried plasma spot) OR (DBS) OR (microsampling*) OR (micro sampling*) OR (mitra) OR (microneedle)). Embase (1974 – Present) was searched with: (‘Antipsychotic Agents’ OR ‘antipsychotic agent*’ OR ‘antipsychotic drug*’ OR ‘antipsychotics’ OR ‘neuroleptics’ OR ‘neuroleptic agent*’ OR ‘neuroleptic drug*’ OR ‘Antipsychotic Agents’) AND (‘Drug Monitoring’ OR ‘monitor*’ OR ‘determin*’ OR ‘level*’ OR ‘concentration*’ OR ‘quantif*’ OR ‘quantita*’ OR ‘TDM’ OR ‘identif*’) AND (‘Dried Blood Spot Testing’ OR ‘dried blood spot*’ OR ‘dried plasma spot’ OR ‘DBS’ OR ‘microsampling*’ OR ‘micro sampling*’ OR ‘mitra’ OR ‘microneedle’).
The final inclusion of the studies was performed by LG and checked by AL. In case of disagreement, DT checked the article and gave the final decision. In addition, general information about the individual microsampling techniques was collected.
Inclusion and Exclusion CriteriaStudies focusing on determining antipsychotic concentrations in whole blood, plasma or serum using microsampling techniques such as (but not exclusively) dried blood spot sampling, dried plasma spot sampling, volumetric absorptive microsampling, or capillary microsampling were included. This includes method validation studies, proof of concept studies, clinical validation studies, and clinical implementation studies.
Studies performed in nonhumans, nonhuman materials, or human materials other than whole blood, serum, or plasma were excluded. In addition, studies using postmortem collected blood were excluded.
Data Screening and ExtractionIn this review, literature was screened to summarize which microsampling techniques are developed today to measure antipsychotic drugs in blood, plasma, or serum. Method validation studies were screened to check if they were in compliance with the international guidelines for method validation.17,18 Subsequently, we checked if stability and selectivity were sufficiently tested to enable routine use of the microsampling technique. In addition, the lower (LLOQ) and upper (ULOQ) limit of quantification of the developed technique were compared with the published therapeutic range for the antipsychotics.1 We also checked if method specific parameters like spot volume and hematocrit effect were studied. Whether a clinical validation study was performed and the number of included patients and samples was also taken in account. The information extracted from included articles was categorized based on microsampling technique.
RESULTS Study SelectionIn the PubMed search, 90 articles were found and in the Embase search 362. After removal of duplicates and reading title and abstract, 19 individual articles were included in this study. The other articles did not meet the inclusion criteria, in particular because many articles focused on deep brain stimulation, which is abbreviated the same way as dried blood spot (DBS). Of one of these 19 publications, we only had an abstract available.20 We therefore had to disregard this one. All 18 included articles were original studies. The majority of the studies focused on development of a DBS method for antipsychotic drugs. Other articles described VAMS and Dry Plasma Spot (DPS) techniques.
Dried Blood Spot Sampling General ConsiderationsDried blood spot sampling is a relatively old microsampling technique, originally developed in the 60s for blood sampling in newborn infants for metabolic diseases.21 Because of the sensitivity of the analytical techniques, DBS methods were initially limited to drugs with a concentration in the mg/L range, but the availability of more sensitive analytical techniques has renewed interest.22 The DBS samples are collected by means of a simple fingerpick after which a few drops of blood are collected on special adsorbent filter paper. After a sufficient drying time, samples can be analyzed, easily transported, or stored with little space required.23
One of the disadvantages of regular blood sampling is the complicated transport. Within hospitals and in the Western world, this is reasonably well regulated. However, in less well-developed countries, transport chains are much longer and transport of plasma tubes sometimes requires preanalytical sample processing techniques and refrigerated transport. The simplicity and low invasiveness of the DBS sampling technique, the high sample stability for many drugs and simple storage and transport requirements make DBS sampling an interesting microsampling technique for TDM of many different drugs. Dried blood spot sampling is also considered an interesting tool for home sampling, because no qualified personnel is required for collecting the DBS samples.
Dried blood spot sampling also has some disadvantages. Most important are the expensive analytical technique to process these very small samples, the so-called hematocrit effect and the measurement in whole blood and not serum. The expensive techniques usually are concentrated in central laboratories or academic centers. The hematocrit value influences blood's viscosity and thus distribution of the blood spot on the paper. Moreover, because of uneven distribution of the drug between red blood cells and plasma, DBS levels generally differ from plasma levels. Differences in hematocrit, caused by sex, age, or health issues, also affect the spread of the blood drop on DBS paper and so the quantitative amount of blood punched out for analysis if not the whole spot is punched. In addition, a nonhomogenous distribution of the compound itself in a DBS spot is observed and influences the analytical accuracy.24–26
Identified StudiesBecause therapeutic drug monitoring is highly recommended for clozapine therapy, several articles focused on developing a DBS method for clozapine. Saracino et al27 were the first to develop an analytical method for measuring clozapine concentrations in DBS samples. The method was validated according to the USPXXVIII and Crystal City guidelines.28 The DBS samples were made by applying 25 μL of previously collected venous EDTA blood on a DBS filter paper from both healthy volunteers and psychiatric patients treated with clozapine. The DBS spots were analyzed in total. The method was found suitable for analysis of clozapine, N-desmethylclozapine and clozapine N-oxide.
In 2014, Pateet et al29 developed a DBS method for the quantification of 16 antipsychotics and 8 metabolites, including clozapine and metabolites. Dried blood spot samples were collected by use of a fingerpick, after several drops of blood were collected in a 25 μL precision capillary. Subsequently, the capillary was emptied on the DBS filter paper to make a DBS spot. The entire spot was analyzed. Validation of the method was performed according to in house guidelines based on the international guidelines of the European Medicines Agency (EMA)17 and the Food and Drug Administration (FDA).18 The method was found valid for detection of 22 of the selected compounds. Only olanzapine and its metabolite were rejected since these compounds were found instable in the aqueous reconstitution solvent. A proof-of-concept study was performed for 10 antipsychotics in 10 patients. In addition, Patteet et al30 performed a clinical validation study in 2015 to compare the antipsychotic concentrations in venous whole blood, serum, and capillary DBS samples. The DBS samples were collected with the same method as was used in the first study.29 No significant difference between DBS and conventional whole blood analysis was found for 11 individual antipsychotics. The included number of samples was, however, relatively low and does not meet the current recommendations for a clinical validation study.19
A method and clinical validation study for therapeutic drug monitoring of clozapine was published by our Groningen group in 2017.31 Dried blood spot samples were collected at several time points before and after drug intake by means of a fingerpick. Subsequently, a few drops of blood were collected on DBS filter cards. After drying, an 8-mm disc was punched out of each DBS spot for analysis. The analytical method was validated based on the FDA guidance for bioanalytical method validation.18 Dried blood spot samples were compared with DBS spots made from venous blood and venous plasma samples taken at the same time points. Clozapine and norclozapine concentrations in the DBS spots showed good agreement with the corresponding plasma concentrations. A conversion factor was established to recalculate the clozapine whole blood DBS concentrations to plasma concentrations to compare with TDM results in venous plasma samples.
In 2022, Bernardo et al32 developed and validated a DBS method for monitoring of aripiprazole, clozapine and paliperidone including their metabolites. Dried blood spot samples were collected by fingerpick, where several drops of blood were collected in a 25 μL precision capillary. Subsequently, the capillary was emptied on the DBS filter paper to make a DBS spot. The entire spot was analyzed. Validation of the method was performed according the EMA guidelines.17 The developed DBS method provided good analytical performance for TDM of all 3 antipsychotic drugs.
A method for detection of clozapine and norclozapine in dried plasma and dried blood spots was developed by Carniel et al in 2022.33 For DBS and DPS samples, 10 μL blood or plasma spiked with different concentrations clozapine and norclozapine was spotted on Whatman 903 paper. The method was clinically validated with DPS and DBS through samples collected from 13 schizophrenic patients. The clozapine and norclozapine levels in the dried samples highly correlated with serum levels, with greater accuracy for DPS compared with DBS.
The research group of Kloosterboer et al34 and Tron et al35 focused on developing a DBS method for TDM of risperidone, aripiprazole, pipamperone, and their metabolites. First, the DBS assay was validated. Dried blood spot samples were prepared by spotting 50 μL of spiked blood onto DBS filter paper. The method validation was performed according to the international FDA and EMA guidelines for bioanalytical method validation.17,18 The hematocrit value of the blood was standardized at 35%. In addition, the influence of spot volume and punching location were investigated in this study. Stability of the antipsychotics in DBS was tested for a wide temperature range and the influence of a wet atmosphere on the stability was also taken into account. The method was found successful for simultaneous quantification of risperidone, aripiprazole, pipamperone, and metabolites in DBS samples.
Kloosterboer et al34 subsequently performed a clinical validation study of the DBS method by quantification of the three antipsychotics in 81 patients (18 years or older). Dried blood spot samples were collected using a fingerpick, and venous samples were collected simultaneously. Samples were compared by using Deming regression and Bland-Altman analyses, which are commonly used analytical methods for this purpose. In contrast to the result from the analytical validation study, the clinical validation study results did not meet the criteria of the Bland-Altman analysis for a successful validation.
Weber et al36 developed a method for simultaneous quantification of risperidone, mirtazapine, and citalopram in DBS samples. Fifty microliters of whole blood was spotted on DBS cards to make DBS samples. The analytical validation was performed according to the international FDA and EMA guidelines. Whole DBS spots were analyzed to exclude the hematocrit effect on homogeneity and to fix the spot volume. No clinical validation study was performed for risperidone. The analytical validation was found successful.
A DBS method for ziprasidone was analytically validated by Mercolini et al37 in 2014. Blank DBS spots were collected by use of a finger puncture from 10 volunteers not treated with ziprasidone. Subsequently, fixed concentrations of ziprasidone solution were added to the wet spots. The analytical method was validated according to Crystal City guidelines.28 A 5-mm diameter partial spot was punched out the DBS spot for analysis. The method was clinically validated in 10 patients using ziprasidone. The developed method was found suitable for detection of ziprasidone in DBS samples.
Protti et al38 developed a High-performance liquid chromatography (HPLC) diode array detection method for asenapine and measured asenapine levels in the following 4 micro matrixes: dried blood spots, dried plasma spots, VAMS from whole blood, and VAMS from plasma. Dried blood spots were collected from healthy volunteers and from patients by fingerpick. For DPS, 20 μL plasma obtained from healthy volunteers or patients was spotted on DBS paper. For VAMS, the VAMS tips were held in respectively blood or plasma for 5 seconds. The microsampling techniques were compared with results obtained by regular plasma analysis. All microsampling techniques showed good correlation with the correlated plasma results. The recovery, precision, and correspondence with plasma of the VAMS technique were, however, consistently better than the DBS and DPS results.
In addition to quantitative analysis, the DBS method can also be used for toxicology screening. Joye et al39 developed a broad-spectrum screening procedure, able to detect several antipsychotics in dried blood spot samples. For method evaluation, the lower limit of identification of 30 individual substances, including haloperidol, risperidone, and quetiapine, in DBS samples was determined. The LOI's for all 3 antipsychotics was 1 ng/mL that is below the therapeutic ranges of the individual antipsychotics.
Volumetric Absorptive Microsampling General ConsiderationsVolumetric absorptive microsampling is a newly developed microsampling technique, designed for home sampling of biological substances. The VAMS devices have a porous tip that absorbs a fixed volume of 10, 20, or 30 μL of blood. The technique is often combined with a fingerpick to allow capillary blood sampling. The samples can be stored in corresponding cartridges or clamshells.24
The VAMS tips were designed to overcome some of the drawbacks of the DBS technique. Most important advantage is that a fixed sample volume is absorbed by the tips independent of the hematocrit level. Although the VAMS technique seems to eliminate the hematocrit effect on the sampling volume, the extraction efficiency of drugs from the VAMS tips is variable and probably still affected by the hematocrit.24,40
Identified StudiesBecause the VAMS technique is relatively new, we initially found only 3 published articles—apart from the already cited study of Protti et al38—regarding the VAMS method for antipsychotics. Stern et al40 performed a validation study of the VAMS technique for 14 psychiatric drugs. Blood from the blood donation service was spiked with several antipsychotics, after which the VAMS tips were held into the blood according to the instruction of the device. After drying, the blood was extracted from the device and analyzed. Method validation was performed according EMA and FDA guidelines for bioanalytical method validation.17,18 A clinical validation study in a limited number of patients was also performed for the antipsychotics quetiapine, norquetiapine, risperidone, and paliperidon. The method validation met the criteria for all the antipsychotics tested, with exception of norclozapine and norquetiapine. Storage time and hematocrit seemed to influence the extractability by the solvents. Before implementation of the VAMS method for routine TDM, a broader clinical validation study has to be conducted.
Nakahara et al41 developed a sampling device comparable with VAMS called a volumetric absorptive paper disc (VAPD). This device contains a filter paper disc—like the DBS technique—that absorbs a fixed volume instead of a porous tip. The device was validated using clozapine and its metabolites. The influence of hematocrit on sampling volume was evaluated. Clozapine concentrations measured in VAPD samples were compared with the concentrations measured in whole blood spots. The VAPD samples were found to collect an accurate volume of blood independent of hematocrit.
Recently, Jacobs et al42 developed a VAMS strategy for monitoring of antipsychotic adherence for 13 commonly used antipsychotics. Whole blood from healthy, drug-free volunteers was spiked with samples from a stock solution of each compound. The VAMS tips were held into the blood as per instructions of the manufacturer until the whole tip turned red with an additional 2-second waiting time. After drying for 3 hours at room temperature, the samples were prepared for analysis. Differences in hematocrit value were tested. Method validation was performed according EMA and FDA guidelines for bioanalytical method validation.17,18 The method was successfully validated for all 13 antipsychotics but the stability was for some antipsychotics, like cyamemazine, melperone, prothipendyl, promethazine, and olanzapine was not optimal.
Millán-Santiago et al43 developed a VAMS strategy for TDM of cariprazine. Whole blood samples from healthy volunteers, not receiving any drug treatment, were collected by fingerpick. Afterward, a standard solution containing cariprazine was used to spike the samples. For clinical validation, VAMS samples and whole blood samples were collected from 3 patients treated with cariprazine. Differences in hematocrit value were also tested. The developed method was concluded to be suitable for TDM of cariprazine using VAMS application.
Marasca et al44 developed a HPLC detection method for detection of clozapine and its metabolites N-desmethylclozapine and clozapine N-oxide in the following 3 micro matrixes: VAMS from whole blood (b-VAMS), VAMS from plasma (p-VAMS), and microfluidic generated dried blood spots (mfDBS). The b-VAMS and p-VAMS samples were prepared by dipping the tip of the VAMS device in spiked blood or plasma until the tip was completely saturated. The mfDBS microsamples were prepared by filling HemaXis microfluidic channels with 10 μL of spiked matrix and transferred to a DBS card. The method was clinically validated with blood and plasma collected from 5 psychiatric patients. The concentrations measured with the dried microsampling technologies were in good agreement with the concentrations measured in normal plasma.
Capillary MicrosamplingAnother recently developed device for accurate blood sampling comparable to the VAMS principle is the hemaPEN (Trajan Medical and Scientific).45 This device contains 4 end-to-end capillaries, which enable the collection of 4 identical DBS samples with an accurate volume by fingerpick. The samples are stored within the pen-like device until analysis. To our knowledge, the hemaPEN device is not yet validated for antipsychotics. Protti et al,46 however, developed and validated a sampling method using the hemaPEN device for the antidepressant drugs sertraline and fluoxetine.
Dried Plasma/Serum SpotDried plasma or serum spots are prepared by pipetting a fixed volume of plasma or serum on filter paper. After drying, the spots have the same advantages regarding transport and storage as DBS cards. However, before DPSs can be created, venous blood must be collected and centrifuged to obtain plasma or serum. This makes the technique unfit for home sampling. The use of DPSs is, therefore, of particular interest if sampling and analysis of a blood sample do not take place at the same location because transport of DPS is far more easy than transport of blood tubes. In addition, when a large number of blood samples require a long storage period after sampling, DPSs are a practical solution to save storage space. A drawback may be the need for investigating stability of the analytes before sampling and the unknown stability of yet unknown analytes in DPS.
Ruggiero et al47 developed a DPS method for TDM of the following 7 antipsychotic drugs: aripiprazole, clozapine, haloperidol, olanzapine, paliperidone, quetiapine, and risperidone. Commercially available human plasma containing different concentrations of the antipsychotic agents were used for the development and validation of the analytical method. A volume of 100 μL was spotted onto paper cards for each concentration of each antipsychotic. For the clinical validation, 30 venous blood samples per agent were collected from patients in EDTA tubes at various times points. The blood was centrifuged and after equilibration for 30 minutes at room temperature, 100 μL aliquots were spotted on filter cards to make DPS. Whole spots were analyzed. A good correlation between antipsychotic concentration in DPS and in the corresponding liquid plasma samples was found for all tested agents. Stability of the DPS was also tested at room temperature for a maximum of 8 days. Haloperidol and risperidone were found to be instable when saved for 8 days at room temperature.
Plasma Extraction CardsThe previous described DPS sampling method is not feasible outside a clinical setting. A few research groups,48,49 therefore, focused on the possibility to filter plasma from whole blood samples collected by fingerpick. This technique uses special multilayer filtration cards to separate plasma from whole blood. The devices contain 2 or 3 layers. Whole blood drops are applied on the upper layer of the card. The upper membranes filter off the erythrocytes, while plasma migrates through the membranes and is collected on the collection disk at the bottom of the card. After a few minutes, the upper layers can be removed from the card leaving a plasma spot on the bottom membrane. After drying, the DPS can be stored or analyzed.
To our knowledge, plasma extraction cards are not yet tested for collecting dried plasma spots of antipsychotic drugs. The device was validated by Li et al using guanfacine.48
DISCUSSIONThis article provides an overview of the microsampling techniques available for TDM of antipsychotic drugs. Fourteen articles were identified in a preliminary review in 2021, involving method validation and clinical validation studies. In an update, 4 new studies were identified, bringing the total to 18 original studies. Most studies focused on the development of a DBS technique for several antipsychotic drugs. However, because of the disadvantages of the DBS technique and new developments in this field, more interest in other microsampling techniques has arisen the past few years.
Microsampling techniques are of growing interest since they have several advantages (Table 1). They require only a small sampling volume (<100 μL) and are collected in a less invasive manner compared with regular sampling techniques. Most of these techniques are suitable for home sampling what makes them particularly interesting for usage in SMI patients who often experience suspicion, withdrawal behavior, and negativism. Especially when necessary they can have the help of a family member, friend, or their own case manager, sampling at home is many times more feasible than to achieve this by other means. A second advantage of home sampling is that timing of the sampling can simply be optimized in relation to drug dosing for a proper interpretation of the result.
Before a microsampling technique can be used for TDM of antipsychotics, a proper method validation is important to ensure that the results that are obtained are valid. In most studies the traditional EMA17 or FDA18 guidelines for validation of bioanalytical methods were applied, but these are in general not sufficient for microsampling techniques. Capiau et al19 developed in 2019 an additional guideline for DBS that is also applicable for other microsampling techniques like VAMS, VAPD, and DPS. This guideline is not (yet) used in the majority of the included studies. Nevertheless, most method validation articles were developed according to international guidelines17,18 and also took additional parameters of special interest for microsampling techniques like hematocrit and spot volume into account.
To make microsampling techniques feasible for TDM of antipsychotics, method validation implies assessment of far more key parameters than strict analytical validity. First of all, the stability of the antipsychotic and for the interpretation relevant metabolites in the sample during transport and storage until analysis should be assessed. Most studies examined the stability of microsampling techniques for at least 1 week at room temperature. This might be too short in large countries with a poor infrastructure. In addition, extreme weather conditions where samples can be exposed to by transport with regular mail are often not examined.
To enable TDM of antipsychotics with a microsampling technique, the method must be suitable for quantification of antipsychotics in a “therapeutic” reference range and preferably also in a certain extend below and above this range. This means that the LLOQ and ULOQ must be accurately identified, as well as the linearity of the quantification. The LLOQ and ULOQ used in the included studies are compared with the therapeutic range of the included antipsychotics (Table 2).
TABLE 2 - Overview of Microsampling Techniques Available for Antipsychotics and Current State of Development Article Antipsychotic Article Type Stability LLOQ – ULOQ (ng/mL) Reference Range (ng/mL) Method Specific DBS Spot Production Clinical Validation, No. Patients Clinical Validation, No. Samples Dried blood spot Saracino et al, 201127 Clozapine N-desmethyl-clozapine
留言 (0)