
記住我

Alcohol dependence (AD) is highly prevalent, frequently chronic and has significant negative effects on the health and quality of life for affected individuals and their families. Alcohol use has been estimated to account for 4.6% of lost global disability-adjusted life-years.1 Alcohol use disorder (AUD) has a point prevalence of 14% in the U.S.2 and is notably undertreated.3 Pharmacotherapy options for alcohol use disorder include only 3 Food and Drug Administration (FDA)-approved compounds (disulfiram, naltrexone, and acamprosate), which have modest effect sizes compared with placebo.4
Recent studies highlight the potential for medications approved for the treatment of other indications (e.g., topiramate, ondansetron, zonisamide, baclofen) to be applied to the treatment of AUD (reviewed in references [5–7]). Study of additional agents, particularly those that act through novel mechanisms, is needed to expand the range of pharmacotherapy options for AUD. The neuroactive steroid system represents one such novel mechanism, and dutasteride, which blocks a key step in the production of 5α-reduced neuroactive steroids, is a promising candidate for treating AUDs based on pre-clinical studies.
5α reduced 3α-hydroxy-pregnane and 3α-hydroxy-androstane neuroactive steroid metabolites of progesterone and testosterone, respectively, are endogenous, highly potent, positive allosteric modulators of GABAA receptors8 that are produced both peripherally and in the brain. An extensive body of pre-clinical research in rodents supports the hypothesis that endogenous neuroactive steroids mediate some of the behavioral and electrophysiological effects of alcohol [reviewed in9,10]. Blockade of ethanol-induced increases of neuroactive steroids in rats using the 5-alpha reductase (5AR) inhibitor finasteride attenuates several behavioral effects of alcohol11–13 and blocks the effects of alcohol on GABAA currents in brain slice preparations.14 In mice and rats trained to self-administer 10% ethanol, treatment with low doses of the endogenous GABAA receptor neurosteroid agonist allopregnanolone (5α-pregnan-3α-ol-20-one)15 or the synthetic neurosteroid GABAA receptor agonist ganaxolone16 increase alcohol self-administration while high doses of these agents reduced alcohol self-administration. In addition, blockade of neuroactive steroid production by the 5AR inhibitor finasteride attenuates the acquisition of alcohol preference in mice17 and reduces alcohol self-administration in mice previously trained to self-administer it,18 as well as in naïve mice.19 Data from human studies supporting neuroactive steroids as mediators of alcohol's effects are more limited. In humans, the plasma concentration of allopregnanolone has been reported to increase after severe intoxication,20,21 but not moderate doses of alcohol.22–24 In a postmortem study of brain tissues from alcohol dependent and control subjects, 2 key neuroactive steroid precursors dehydroepiandrosterone and pregnenolone were reported to be elevated in several limbic regions in tissues from the alcohol dependent group.25 Another group reported increased allopregnanolone immunoreactivity in the ventral tegmental area of post-mortem brain from alcohol dependent subjects compared with age-matched controls.26 Finally, in a randomized placebo-controlled human laboratory study of male social drinkers, a single 4-mg dose of the 5-alpha reductase inhibitor dutasteride reduced the sedative effects of alcohol and also reduced drinking in the natural environment for 1 to 2 weeks after this single-dose treatment.27
Finasteride, which has been widely used as a pharmacological tool in animal studies of neuroactive steroids, blocks both type I and II 5AR in rodents. However, in humans, finasteride at clinical doses blocks only type II 5AR, the 5AR isoenzyme most abundant in prostate and skin but absent in adult brain. Dutasteride, a second FDA-approved 5AR inhibitor for the treatment of prostatic hyperplasia by reducing 5α-dihydrotestosterone, irreversibly inhibits both type I (brain, adrenal, liver and adipose tissue) and type II (liver, skin and prostate) 5AR enzymes at clinically relevant dosages, leading to a greater reduction in 5α-dihydrotestosterone (DHT) levels than finasteride without suppressing testosterone.28 This broader 5AR inhibition profile, together with good tolerability and safety, make dutasteride an excellent candidate medication for potentially reducing drinking in humans.
In the current study, we examine the efficacy and tolerability of dutasteride in male participants who drink heavily and have a goal to reduce or stop drinking. To identify potential drinking related measures associated with dutasteride treatment efficacy, we also examined in post hoc exploratory models alcohol cravings, a family history of alcohol problems, drinking to cope and drinking to enhance motives as potential moderators of treatment effects. We also examined smoking as a potential moderator as smoking has been identified as an important moderator of alcohol treatment effects,29–32
METHODS Study DesignThe study was a 12-week randomized placebo-controlled parallel-groups trial of dutasteride for reducing drinking in men. Patients also received brief alcohol counseling and medication management at each of 5 biweekly treatment visits to enhance medication use and treatment participation and the assist participants in setting goals to stop or reduce drinking. The study was conducted in the clinical research center at the University of Connecticut Health Center and was approved by the Institutional Review Board. The study was registered with www.clinicaltrials.gov (NCT01758523) in December 2010. Participants were enrolled beginning January 2013 and ending in April 2017.
Patients attended a screening and baseline visit for assessment of eligibility and collection of baseline characteristics. Study medication was dispensed beginning at the baseline visit and refills provided at 5 biweekly study visits. Unused medication doses, if any, were returned at biweekly study visits and logged by the study nurse. Telephone calls during nonvisit weeks were made to patients by study staff to encourage medication use and respond to any side effect concerns. An end-point assessment visit was conducted at the end of the 12-week treatment period.
PatientsMale drinkers who wanted to reduce or stop drinking were recruited using advertisements in local media (including radio ads, text ads in newspapers, and weekly community circulars) and by posting recruitment materials at medical and dental clinics. Women were excluded from this first RCT examining dutasteride for reducing drinking, pending results in men, at the recommendation of the FDA reviewer for our initial Investigational New Drug (IND) application due to concerns regarding potential negative effects of 5α-reductase inhibition on fetal development of external genitalia in male offspring.
Inclusion criteria were: men aged 18 to 70 years; an average weekly alcohol consumption of >24 drinks per week; ability to read English at the 8th grade or higher level; no evidence on clinical examination of significant cognitive impairment; a treatment goal to either stop drinking or reduce drinking to nonhazardous levels (not more than 4 drinks/day and not more than 14 drinks per week) and willingness to provide signed, informed consent to participate in the study.
Exclusion criteria included: a current, clinically significant physical disease or abnormality on the basis of medical history, physical examination, or routine laboratory evaluation; a serious psychiatric illness on the basis of history or psychiatric examination (i.e., schizophrenia, bipolar disorder, severe or psychotic major depression, organic mental disorder, current clinically significant eating disorder, or substantial suicide or violence risk); a current DSM-IV diagnosis of drug dependence (other than nicotine dependence); a history of serious alcohol withdrawal symptoms (e.g., substantial tremor, autonomic changes, perceptual distortions, seizures, delirium, or hallucinations or of prior inpatient treatment of alcohol withdrawal).
Patients were not paid for attending screening or treatment visits. They were paid to complete end of treatment research assessments.
Treatments CounselingBiweekly medical management based on that used in the Combine Study33,34 was provided by a study nurse or physician at the baseline visit and 5 subsequent biweekly treatment visits. Goals of medical management include enhancement of medication use and treatment participation. The initial session included review of any identified medical concerns related to drinking and review of a self-help brochure “Cutting Back—A sensible approach to drinking and health”35 to encourage patients to self-evaluate their drinking and set goals to stop or reduce drinking. Patients who identified a goal of reduction rather than abstinence were advised that an appropriate goal would be to consume no more than 14 drinks per week and not more than 4 drinks on a single day.
MedicationParticipants were randomly assigned to dutasteride or placebo using an urn randomization program to balance participants on age and baseline alcohol use measures (HDD frequency, drinks per drinking day and number of DSM-IV AD criteria). Patients in the dutasteride group took a loading dose of 4 mg dutasteride at the baseline visit followed by 1 mg daily for 12 weeks. Commercially sourced dutasteride 0.5 mg capsules were over-encapsulated to blind participants, placebo group participants took an equal number of identically appearing placebo (lactose powder) capsules. Dutasteride is not FDA approved for AD and our use of dutasteride in this study is investigational. The corresponding author holds an IND for investigating the use of dutasteride in alcohol use disorder.
AssessmentsThe Structured Clinical Interview for DSM-IV (SCID-I/P)36 was administered at the in-person screening visit to classify participants according to the presence or absence of psychiatric disorders including AD. The alcohol section of the Family History Assessment Module FHAM37 was used to provide information concerning biological relatives' history of alcohol use. The timeline follow-back method38 was used to estimate drinking at intake (past 60 days) and at each biweekly study visit. The Penn Alcohol Craving Scale (PACS) was used at baseline to capture the frequency, intensity, and duration of craving over the past week.39 The State version of the Spielberger State-Trait Anxiety Inventory (STAI),40 was administered at the baseline visit. Baseline smoking status was based on self-reported smoking during the 30 days before screening. Participants using 1 or more cigarettes daily were considered smokers.
To assess drinking motives, the Cooper Drinking Motives Questionnaire [DMQ41,42;] was administer at the baseline visit. This instrument contains 5 items for each of 4 subscales, capturing drinking to: (a) cope motives (e.g., “Because it helps when you are feeling nervous or depressed”), (b) enhancement motives (e.g., “Because it's fun”), (c) social motives (e.g., “Because it makes a social occasion more enjoyable”), and (d) conformity motives (e.g., “Because it helps me fit in”). The percentage of total motives score for coping and enhancement motives subscales were used in statistical analysis. Social motives and conformity were not included as participants reported predominately drinking alone.
Laboratory TestingSerum 3α-androstanediol glucuronide (3α-diolG) was measured at screening and after 6 and 12 weeks of treatment using a commercial ELISA kit (Alpco Diagnostics, Salem, NH) as a biochemical measure of 5AR inhibition by dutasteride. 3α-diolG is a major metabolite of testosterone and the primary metabolic end-product of 5α,3α-androstane neuroactive steroids, which has been used to monitor the reduction of 5AR activity in both men43 and women treated with finasteride.44,45
Statistical AnalysisStatistical analysis was performed using SPSS (v27; IBM, Armonk, NY). For the planned primary statistical tests, P < 0.05 was considered significant, whereas for the exploratory post-hoc secondary analysis of potential moderators, P < 0.05 was considered nominally significant. Group differences in continuous measures were analyzed using independent-samples t-test and for categorical variables χ2 tests were used.
Drinking data during the 12-week treatment were collected using the timeline follow-back method46 and were aggregated to the weekly level. The number of heavy drinking days (HDD; 5 or more drinks in a day) per week and the total number of standard drinks (SD) per week were the primary outcomes. Generalized linear mixed models were used to examine medication group differences in these outcomes. Models included fixed effects for medication group, week, the interaction between medication and week as well as a random effect for intercept and an unstructured covariance term. Week was recoded by subtracting 12 so that the test of treatment effect compared groups at the conclusion of the study (week 12). For HDD/week outcomes a binomial distribution with logit link function was used while for the SD/week outcome a negative binomial with log link function was used. The number of HDD or SD/week for the 2-week interval preceding start of medication was included as a fixed-effect variable. Generalized linear models included all available data from the modified intention to treat (ITT) sample of 135 patients who attended at least 1 visit after initiation of medication. For the post-hoc exploratory evaluation of moderation effects, GLM models also included the interaction of medication separately with each of 5 potential moderator variables.
Responder analysis used χ2 tests (2-sided) to compare the number of patients in each group with clinically meaningful reductions in drinking including a 60% reduction in SD/wk and no hazardous drinking (0 HDD and <15 SD/wk) during the last 4 weeks of treatment.
RESULTS Study SampleOne hundred eighty-nine treatment seeking men attended the screening visit, of which 24 were screen failures and 23 failed to return for the baseline visit leaving 142 participants randomized to medication (dutasteride, n = 74). Seven participants did not return after the baseline randomization visit providing a modified ITT sample of 135 participants (68 dutasteride and 67 placebo) who provided drinking data post-randomization, Figure 1. One hundred seven participants (79.3%) completed the entire 12 weeks of treatment (dutasteride arm n = 53, 77.9%; placebo arm =54, 80.6%; x2=0.15, df = 1, P = 0.7) providing 80% power to detect a between groups medium effect size (0.55) for change in drinking with α = 0.05. The mean number of treatment weeks completed were not different between arms (dut 10.2 vs pbo 10.7). There was a high level of medication adherence among participants in both arms. Dutasteride arm participants reported taking 94.2% of doses (s.d. = 13.3) and placebo participants 94.9% of doses (s.d. = 9.0). Self-reported medication use was verified from biweekly visit pill counts. 3α-androstanediol glucuronide levels (a measure of 5α-R activity) were decreased compared with baseline by 81% and 80% in the dutasteride group at 6 and 12 weeks versus −1% and 1% in the placebo treatment group.
 FIGURE 1:
FIGURE 1: Consort diagram showing flow of patients in the protocol.
Participants were on average 53 years old (range, 30–70 years), primarily White (97%), most were married (67%) and working full- or part-time (81%). Twenty-one percent of participants were current smokers and 65% reported a life-time history of smoking. Demographic features did not differ between participants randomized to dutasteride versus placebo (see Table 1). There were no significant differences between groups (dutasteride vs placebo) for measures of alcohol consumption during the 60 days before screening including the number of SDs per week (48.8 vs 47.3), number of HDD per week (5.2 vs 5.2), abstinent days per week (0.67 vs 0.62) or percentage of men with a treatment goal to stop drinking (49.3% vs 48.5%). While the dutasteride group were more likely to have had a prior episode of treatment for alcohol use (59% vs 40%, P = 0.03) the number of DSM-IV AD criteria did not differ between groups (4.3 vs 4.0). Four participants (3%) had current cannabis use, none had current cocaine or opioid use. Lifetime history of a drug use disorder was reported by 37% of participants and 10% reported a history of conduct disorder. Lifetime history of a mood or anxiety disorder were reported by 30% of participants. Rates of lifetime psychiatric disorders did not differ between participants randomized to placebo versus dutasteride, Table 2.
TABLE 1 - Demographics and Pretreatment Clinical Measures Placebo (n = 67) Dutasteride (n = 68) P* Demographics n % n % Race 1.00 White 65 97.0 66 97.1 Black 1 1.5 1 1.5 South Asian (Indian) 1 1.5 1 1.5 Age (yr)† 53.1 9.4 53.0 7.9 0.97 Weight (lbs)† 216.3 34.5 210.1 36.1 0.29 Current smoker 15 22.4 14 20.6 0.80 Lifetime smoker 43 64.2 45 66.2 0.81 Married/partnered 45 67.2 47 69.1 0.81 Employment status 0.31 Full-time 52 77.6 46 67.6 Part-time 5 7.5 7 10.3 Retired 6 9.0 4 5.9 Other 1 1.5 5 7.4 Not working 3 4.5 6 8.9 Years of education† 15.0 3.0 14.7 2.5 0.53 Income‡ 0.49 Less than $40,000 5 7.6 7 10.5 $40,000–$79,999 12 18.2 17 25.3 $80,000–$119,000 16 24.3 18 26.8 $120,000 or more 33 50.0 25 37.3 Clinical Measures SAI score† 36.1 9.9 36.7 11.5 0.73 Abstinent days per week†,§ 0.62 1.1 0.67 1.1 0.78 Heavy drinking days per week†,§ 5.2 2.1 5.2 2.2 0.99 Standard drinks per week†,§ 47.3 20.4 48.8 24.0 0.70 DSM-IV criteria† 4.0 1.6 4.3 1.6 0.29 SIP score† 16.8 8.8 17.2 8.2 0.78 Prior alcohol treatment(s) 27 40.3 40 58.8 0.03 Treatment goal—stop drinking 33 49.3 33 48.5 0.93The P value with significant findings is set in bold.
*t Test for continuous measures and χ2 test for categorical measures.
†Values are mean and standard deviation.
‡Income data for one dutasteride and one placebo patient were missing.
§Based on TLFB for 60 days preceding the screening visit.
SAI, Spielberg Anxiety Inventory (state); SIP, Short Index of Problems.
* χ2 test.
† Generalized anxiety, panic, obsessive compulsive disorder or social phobia.
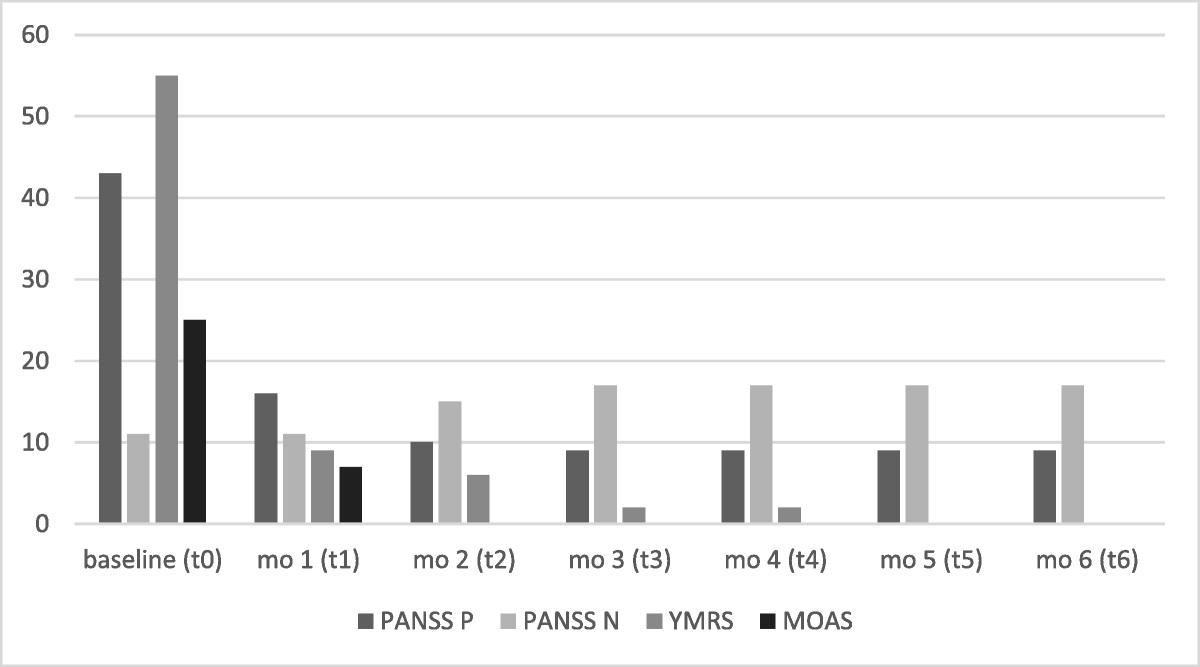
Comparison of treatment groups (68 dutasteride and 67 placebo) on the primary outcomes of HDD per week and SD per week using generalized linear mixed models (GLMM) that included baseline drinking levels, treatment condition, and treatment-time as predictors identified significant 2-way interactions of treatment-time for HDD/week (F = 9.2, df = 11406, P = 0.002) and for SD/week (F = 4.8, df = 11405, P = 0.028) such that dutasteride-treated participants reduced drinking over time more than placebo participants (see Fig. 2).
 FIGURE 2:
FIGURE 2: Heavy drinking days per week (left) and standard drinks per week (right) for placebo-treated (n = 67) vs dutasteride-treated (n = 68) men. The number of participants providing data at each 2-week study visit is indicated on the left panel. The mean and standard error of the mean are represented.
During the last 4 weeks of the 12-week treatment, the proportion of participants with a ≥ 60% reduction in SD/wk compared with screening, representing a clinically meaningful reduction from a group average of 48 SDs/wk to less than 20, was significantly greater for the dutasteride versus the placebo group (45% vs 24%; χ2 = 5.3, P = 0.021; odds ratio = 2.6 [95% confidence interval = 1.1–6.0]). In addition, for per protocol completers (dutasteride = 53; placebo = 54), 25% of participants in the dutasteride arm had no hazardous drinking (no HDDs and not more than 14 SD/wk) during the last month of treatment compared with 6% of placebo-treated subjects respectively (χ2 = 7.6, P = 0.006; odds ratio = 5.5 [95% confidence interval = 1.5–20.7] NNT = 6). Although abstinence was not one of the primary outcomes examined, the dutasteride treatment group had a numerically greater percent days abstinent during the last 4 weeks of treatment (dutasteride 29% vs placebo 23%) which was not statistically significant.
Associations of Baseline Phenotype Measures With Treatment ResponseIn an exploratory post hoc effort to identify potential drinking-related moderators associated with treatment response we examined 5 measures collected at study entry, including drinking to cope and drinking to enhance motives, self-reported alcohol cravings, the proportion of first-degree relatives with a history of AD (a surrogate for genetic loading) and smoking. Among these features, only drinking to cope (DTC) and smoking interacted with medication group to predict drinking over the 12-week treatment period. For the drinking to cope measure, there was a nominally significant interaction of medication group and baseline DTC for HDD/wk (F = 6.0, df = 1,1380, P = 0.015). The form of the interaction is illustrated in Figure 3 by contrasting HDD over time using a median split in the sample based on the baseline DTC score. A similar form of interaction was observed for SD/week which was not statistically significant. For the higher DTC group there were very limited reductions in drinking among placebo compared with dutasteride-treated participants. For the high drinking to cope group there was a significant medication-time interaction for the HDD/wk measure (F = 8.5, df = 1653, P = 0.004).
 FIGURE 3:
FIGURE 3: Heavy drinking days per week for dutasteride vs placebo subjects stratified by low vs high drinking to cope as a percentage of total drinking motives score (0–25% vs 26–63%). The number of participants providing data at each 2-week study visit is indicated for each group. The mean and standard error of the mean are represented.
There was also a nominally significant interaction of medication group and smoking (baseline cigarettes/day) for HDD/wk (F = 4.2, df = 11,404, P = 0.040) and SD/wk (F = 5.6, df = 11,403, P = 0.018) such that smokers treated with dutasteride (n = 14) reported numerically more HDD and SD/wk than smokers treated with placebo (n = 15) during most of the treatment period, while for nonsmokers treated with dutasteride (n = 52) there was a nominally significant reduction in HDD/wk (treatment-time—F = 5.1, df = 11,133, P = 0.024) and SD/wk (treatment-time—F = 4.3, df = 1,1132, P = 0.038) compared with the placebo group (n = 54) Figure 4.
 FIGURE 4:
FIGURE 4: Heavy drinking days and number of drinks per week for dutasteride-treated vs placebo-treated participants stratified by smoking status with 29 smokers (left graphs) vs 106 nonsmokers (right graphs). Panel A depicts HDD/wk and panel B SD/wk. The number of participants providing data at each 2-week study visit is indicated for each group in panel B graphs. The mean and standard error of the mean are represented.
Adverse EffectsSerious adverse events included 4 patients who entered inpatient detox programs (1 before randomization, 2 in the week after randomization to dutasteride and 1 subject after 4 weeks of treatment with placebo). Three participants were briefly hospitalized for medical conditions none of which were considered related to study treatment (two dutasteride arm participants, one for treatment of a tonsillar abscess and one for exacerbation of chronic obstructive pulmonary disease; one placebo arm subject for treatment of chronic back pain).
The proportion of participants exposed to study medication who reported at least one nonserious adverse effect was not significantly different for the dutasteride versus placebo groups 71.6% versus 67.1% (χ2 =0.32 P = 0.57). Adverse events that were reported by more participants in the dutasteride compared with the placebo arm included stomach discomfort (16.4% vs 4.5%, P = 0.04) and reduced libido (9.0% vs 0%; P = 0.03) (see Table 3). Among dutasteride-treated participants who reported stomach discomfort, the proportion who completed the 12-week treatment (81.8%) or achieved a 60% reduction in SD/wk (44.4%) did not differ compared with those who did not report this side effect (77.2% and 45.5%, respectively). More participants in the dutasteride arm (n = 4) than the placebo arm (n = 1) stopped medication due to side effects.
TABLE 3 - Adverse Effects in Descending Order of Frequency in the Dutasteride Group Placebo (n = 67) Dutasteride (n = 68) P* Stomach discomfort 3 (4.5) 11 (16.2) 0.04 Muscle or joint pain 7 (10.4) 11 (16.2) 0.45 Headache 11 (16.4) 10 (14.7) 1.00 Reduced libido 0 (0.0) 6 (8.8) 0.03 Fatigue 7 (10.4) 5 (7.4) 0.76 Change in sleep 3 (4.5) 5 (7.4) 0.72 Nausea 5 (7.5) 4 (5.9) 1.00 Impotence 2 (3.0) 4 (5.9) 0.49Data shown reflect adverse effect incidence in the dutasteride or placebo group ≥5%.
Number of subjects (%) based on the modified ITT sample.
*Fisher exact test.
The P values with significant findings are shown in bold.
In this first randomized placebo-controlled study of dutasteride for the reduction of heavy drinking, we observed that treatment with dutasteride, 1 mg daily, was associated with reduced heavy drinking days and total drinks per week compared with placebo over a 12-week treatment period. These results support the potential clinical utility of dutasteride beyond its effects on lowering DHT levels in treatments for prostatic hypertrophy and alopecia. Our current results builds on the extensive preclinical literature investigating the potential role of neuroactive steroids in moderating alcohol use.
The efficacy of dutasteride compared with placebo was greater in participants reporting higher drinking to cope motives at study entry. Comorbid symptoms of anxiety and/or depression are common among treatment seeking drinkers and are associated with worse treatment outcomes.47 Drinking to self-medicate anxiety and mood symptoms increases the risk of AUD incidence and persistence48,49 and drinking to cope appears to be a keystone feature linking internalizing symptoms with adverse drinking-related outcomes.50,51 Drinking to cope has been proposed as a genetic endophenotype based on findings of a statistically significant association of alcohol use related genetic loci and drinking to cope motives.52
Epidemiologic, preclinical and clinical studies have documented bidirectional effects of stress and drinking problems.53–57 The association of dutasteride response with baseline measures of drinking to cope with negative emotions and distress suggest that the effects of dutasteride to reduce drinking may include a mechanism of action involving the stress response system including the HPA axis. In addition to the well-known role of 5AR enzymes in conversion of testosterone to dihydrotestosterone, 5AR (and 5α-reductase) enzymes convert cortisol to 5-dihydrocortisol, which is then metabolized to the inactive cortisol metabolite 5-tetrahydrocortisol (5a/b-THF) by 3-hydroxysteroid dehydrogenase. 5α-THF and 5α-THF each represent ≈20% of total daily urinary excretion of cortisol metabolites.58 Dutasteride and finasteride treatment for 3 months in healthy subjects reduced levels of 5α-reduced cortisol urinary metabolites by over 95% without an increase in 5α-reduced cortisol metabolites resulting in an overall reduction of 24-hour urinary cortisol metabolites but without a change in morning cortisol.59 This finding suggests that 5AR inhibitors may reduce overall adrenal cortisol output by reduction in rates of elimination without significant changes in plasma cortisol levels. Hence, a second mechanism by which dutasteride could moderate alcohol intake may relate to changes in HPA axis reactivity, which may be relevant to AUD patients with elevated perceived stress, anxiety, or trauma.60
Other investigators have suggested that neuroactive steroid agonists may be useful in the treatment of AUD.61 In a recent human subject laboratory study of patients with AUD, Milivojevic et al,62 reported that supraphysiologic doses of the neurosteroid precursor pregnenolone, 300 or 500 mg twice daily for 7–10 days, reduced alcohol craving in response to listening to personalized scripts of
留言 (0)