Structure of the fingers
Hand trauma is very common in the clinic. Due to the special structure of the fingers: the skin of the finger pulp has thick keratinized layer, and the deep surface has vertical fiber bundles connecting the skin with the superficial fascia, deep fascia, tendon sheaths and other deep structures, so that the skin of the finger pulp lack elasticity and is not easy to move, but is conducive to grasping, gripping, and holding objects, and the pulp of the finger has abundant nerve endings and sensory bodies; the dorsal side of the finger has thin subcutaneous soft tissues, which can easily lead to the skin defect when trauma occurs, exposing the tendons and bones, so it is very necessary to repair the middle and distal part of the finger when it is defective [1,2,3].
Research status of flap repair for finger defects
Repair of finger injuries has always been a challenge for hand surgeons. In order to preserve the function, appearance, and sensation of the finger, a simple skin graft cannot meet the needs of finger injuries, and flap repair is often required. There are many methods of repair with varying results. Traditional repair methods include the V-Y flap, the adjacent finger flap, the abdominal flap, the island flap of the finger artery, and the dorsal fasciocu taneous flap, etc. The V-Y flap has a limited scope of repair and does not provide adequate coverage for defects larger than 1 cm2 in size. Neighboring finger flaps and abdominal flaps require prolonged forced positional immobilization, which is difficult for most patients to tolerate and does not allow reconstruction of sensation. The adjacent finger flap requires sacrifice of the integrity of the adjacent finger, but in this cases, the defects were located in the mid-distal segment of the adjacent finger, making this approach unfeasible. Abdominal flaps are also not optimal because of their bulky appearance, poor abrasion resistance, and severe hyperpigmentation. Finger artery island flaps have a reliable blood supply, but the sacrifice of one of the finger arteries makes the finger less cold-tolerant and does not allow for the reconstruction of sensation. In addition, the large size of the defects and the fact that some of the defects crossed the distal transverse finger stripe in the present patients made it impossible to perform the retrograde island flap technique in the finger arteries. The dorsal finger fasciocutaneous flap has poor blood supply, is prone to blistering, and has mild atrophy in the later stages of the flap, and in the case of large dorsal finger defects, this technique is not feasible. The dorsal metacarpal artery perforator flap has been reported by some authors to have a fair efficacy in multiple finger injuries, but it has a large postoperative scar in the donor area on the dorsal part of the hand, which is often a major obstacle in patients with high demands on the appearance of the hand. Patients with high demands on the appearance of the hand are often difficult to accept [7,8,9,10,11,12,13, 28].
Flap from the foot is used to repair finger defects
The skin of the toes and fingers are similar tissues, and due to this natural similarity, tissue flap transplantation from the foot is often used to repair finger defects. By grafting the fibular side of the great toe or the tibial side of the second toe, it is possible to maximize the restoration of finger shape and sensation. This method keeps the donor area hidden, maintains constant vascularity, causes minimal damage to the donor foot, and does not affect walking. This approach aligns with the principle of tissue transplantation, aiming to restore and reconstruct the recipient area while minimizing traumatic loss to the donor area [14,15,16]. Therefore, some scholars have tried to solve this problem by designing a free first metatarsal dorsal artery bilobed flap with good results. Although the free first dorsal metatarsal artery bilobed flap had become a classic technique for repairing the proximal skin and soft tissue defects of two adjacent fingers, the combined transplantation of the fibular side of the great toe and the tibial side of the second toe with the first dorsal metatarsal artery as the pedicle for repairing the middle and distal defects of adjacent fingers has a lot of difficulties, because the transplanted fingers need to share the vascular pedicle, and there is the problem of insufficient vascular span, and it is often necessary to make two tissue flaps separately, which makes the surgical difficulty and the risk is higher. At the same time, when the toe tissue flap is cut, improper operation will often leave bone and tendon exposed, and it is not easy for the skin graft to survive, and it is often necessary to close the trauma by using a skin flap or amputation of the toe, and even if the skin graft survives, it is not wear-resistant, and the effect is less satisfactory.
In order to solve the problem of insufficient vascular span when the first and second toe tissue flaps share vascular pedicle for repairing mid-distal defects in adjacent fingers, many people have carried out a lot of explorations. Based on the type of anastomosis between the 1st dorsal metatarsal artery and the first plantar artery and the thickness of the arteries entering the great toe and the second toe, Xu YJ et al. used to cut off the plantar artery entering the lesser toe or the 2nd toe and then anastomosed with the plantar deep branch of the dorsal artery of the foot, respectively [16]. Although this method can increase the length of the vascular pedicle between one tissue flap, it is also necessary to do the vascular anastomosis in two places, and the surgical difficulty and risk is not reduced with the cutting of two tissue flaps respectively, which is not convenient for clinical promotion. Some scholars also use the free second toe of the first dorsal (basal) artery pedicle to reconstruct the fingers. at the same time carrying great toes fibular flap repair adjacent finger defects, the great fibular toe bottom artery surface with a skin bridge or suture into the skin tube, the same three weeks later cut off the skin bridge to break the tip [17]. Although the operation requires two times, it significantly reduces the risk and difficulty of the operation. However, cutting the skin between the toe webs of the 1st and 2nd toes or rolling it into a skin tube to cover the exposed vascular tip is easy to cause vascular compression or spasm due to swelling or exposed vascular tip, resulting in vascular complications of one side of the flap. At the same time, it is wasteful to the skin between the toe webs.
Surgical exploration
In clinical practice, we have used the cell scaffold to cover the donor area after the foot flap has been cut in the clinical phase I. The skin is implanted after the dermis grows to cover the exposed tendon and phalanx about three weeks after surgery. This method greatly improves the survival rate and quality of the implanted skin and solves the problem of handling the donor area. At the same time, using of pedicle island flap skin grafting to repair wounds in the distal area in clinical practice, breaking the routine that the pedicle of the vascular pedicle flap needs to be buried under the skin. So that the repair has become more casual, and good results have been achieved. Combined with the previous experience, we use the free bilobed flap with the first dorsal (plantar) metatarsal artery pedicle repair the mid-distal defects in adjacent fingers, and apply the cell scaffold to cover the donor area of the foot, and at the same time, the excess cell scaffold is sewn into a leather tube to wrap the pedicle between the flaps. This surgery not only reduces the damage of the donor area and solves the embarrassment of the skin grafted of the donor area that is not abrasion-resistant and not easy to be viable, but also solves the defect that the bifurcation between the first and second toe base arteries is short, and the flap cannot be co-trunked to reach the middle distal segment through the subcutaneous tunnel. The use of a single vessel pedicle to supply blood to both traumas saves surgical time and reduces the risk and difficulty of the procedure.
Mechanism of action of the cell scaffold
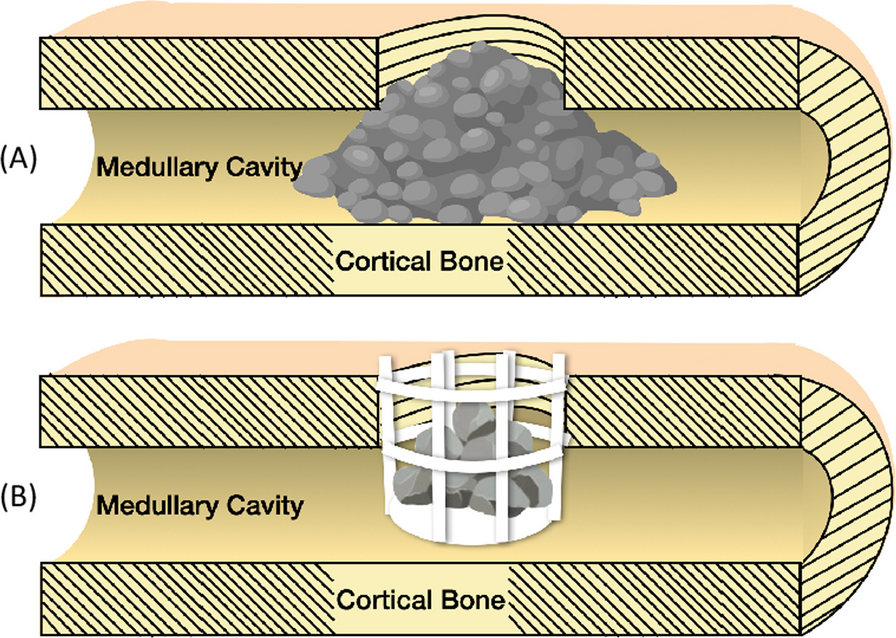
The silicone film on the outer layer of the cell scaffold mimics the epidermis, providing some resistance to infection and preventing water evaporation. Meanwhile, the inner layer consists of a collagen sponge with a porous reticular three-dimensional structure, capable of temporarily replacing dermal tissue. This structure can stimulate wound fibroblasts and capillary to grow and produce extracellular matrix, ultimately forming new tissue similar to the dermis. Overall, the cell scaffold’s structure closely resembles that of human skin, and the inner layer’s mesh scaffold creates a microenvironment conducive to the organized growth of capillaries, fibroblasts, and other components around the wound [29].
2–3 weeks later, the collagen will degrade and be replaced by new granulation tissue, forming visible pink granulation tissue in the clinic, which establishes blood circulation with the bone or tendon it covers, effectively covering the wound. When the cell scaffold provides enough matrix for skin grafting, we will perform a skin graft, which greatly improves the survival rate of the skin. The transplanted skin is elastic, durable, and scar-free.
Advantages and disadvantages of surgeryAdvantages
1. The trauma of adjacent fingers is repaired by a bilobed flap, only one set of blood vessels need to be anastomosed, which reduces the risk, time and difficulty of the operation. 2. The length of the exposed vessel pedicle between the bilobed flap can meet the the activity of finger splitting (two adjacent fingers can be separated in the coronal and sagittal plane), which is more conducive to the flexion and extension of the patient’s two injured fingers in a sagittal plane, so as to avoid the vascular pedicle being torn. 3. After the cell scaffold is covered, the granulation tissue under the wound surface of the donor area grows quickly, the quality is good, this improves the repair effect of the supply area. which avoids the trauma of toe amputation and flap repair in the donor area. 4. The vascular pedicle between the flaps is narrow, and it is easy to cut the pedicle and trim the shape, which can make the fingers get a satisfying look and good functionality. 5. The root of the toe nerve anastomosed with the nerve stumps of the fingers, giving a satisfactory restoration of sensation to the fingers.
Disadvantages
(1) The pedicle of the blood vessel between the flaps needs to be cut off twice. (2) The cell scaffold is expensive, requires a second surgical skin grafting. However, compared with other methods currently used in clinical practice, this method has obvious advantages and is worthy of clinical promotion. (3) Although the.
length of our vascular pedicle is longer than before, it still cannot meet the normal range of activity required for adjacent fingers. The movement of the two fingers needs.
to be synchronized to some extent, which may cause some patients to experience a temporary syndactylization effect. Therefore, we will promptly sever the pedicle to reduce the risk of syndactyly in patients. 4. The harvesting of the first dorsal ( plantar) metatarsal artery reduces the possibility of toe transfer on the same side due to the primary vascular deficiency during toe transplantation. (Table 3)
Table 3 Advantages and disadvantagesIntraoperative and postoperative points
In order to obtain a better clinical effect, we should pay attention to the following points: (1) The donor area of the foot should completely stop bleeding, rinse the wound with normal saline, and try to maintain the sterility of the wound in the surgical area (2). For larger wounds, the cell scaffold needs to be compressed to ensure good contact between the cell scaffold and the wound (3). The time of the skin graft should be 3 weeks after the phase I surgery. When the silica gel film separates from the collagen sponge layer, the amount of granulation tissue is sufficient and turns from dark red to pink (4). Generally, 7–9 days postoperatively, after the risk period of the flap blood vessels, the patients should be actively instructed to carry out finger flexion and extension exercises to promote the maximum functional recovery of the joint. (Table 4)
Table 4 Intraoperative and postoperative pointsThere are certain limitations in this article: (1) It is a single-center study and has a small sample size. (2) Some cases have a short follow-up period. Further multicenter large-scale prospective studies are necessary to further confirm the efficacy and safety of this procedure. Despite some of the limitations, we believe that our study is still instructive.









留言 (0)