
記住我






In this prospective interventional study, 50 patients candidates for radiofrequency were evaluated for treating symptomatic lumbar disc prolapse. They were recruited from the Pain Centre in Beni-Suef governorate and the Neurology clinic in Beni-Suef University Hospital from January 2022 to December 2022. The study was registered in ClinicalTrials.gov on 18/1/2022 (the identification number is NCT05193461).
Eligibility criteria: poor response to conservative pharmacological treatment and physiotherapy in patients with more than three months of lumbar disc prolapse.
We excluded patients with other medical disorders that might account for their pain-related disability such as those with radiological evidence of hip or facet osteoarthritis, sacroiliitis, paravertebral abscess, Pott’s disease, osteomyelitis or neoplastic lesion affecting the vertebrae. Patients candidates for surgery who had severe lumbar disc herniation affecting sphincteric or motor functions, patients having contraindications to radiofrequency (sepsis or coagulopathy), and pregnant patients were also excluded.
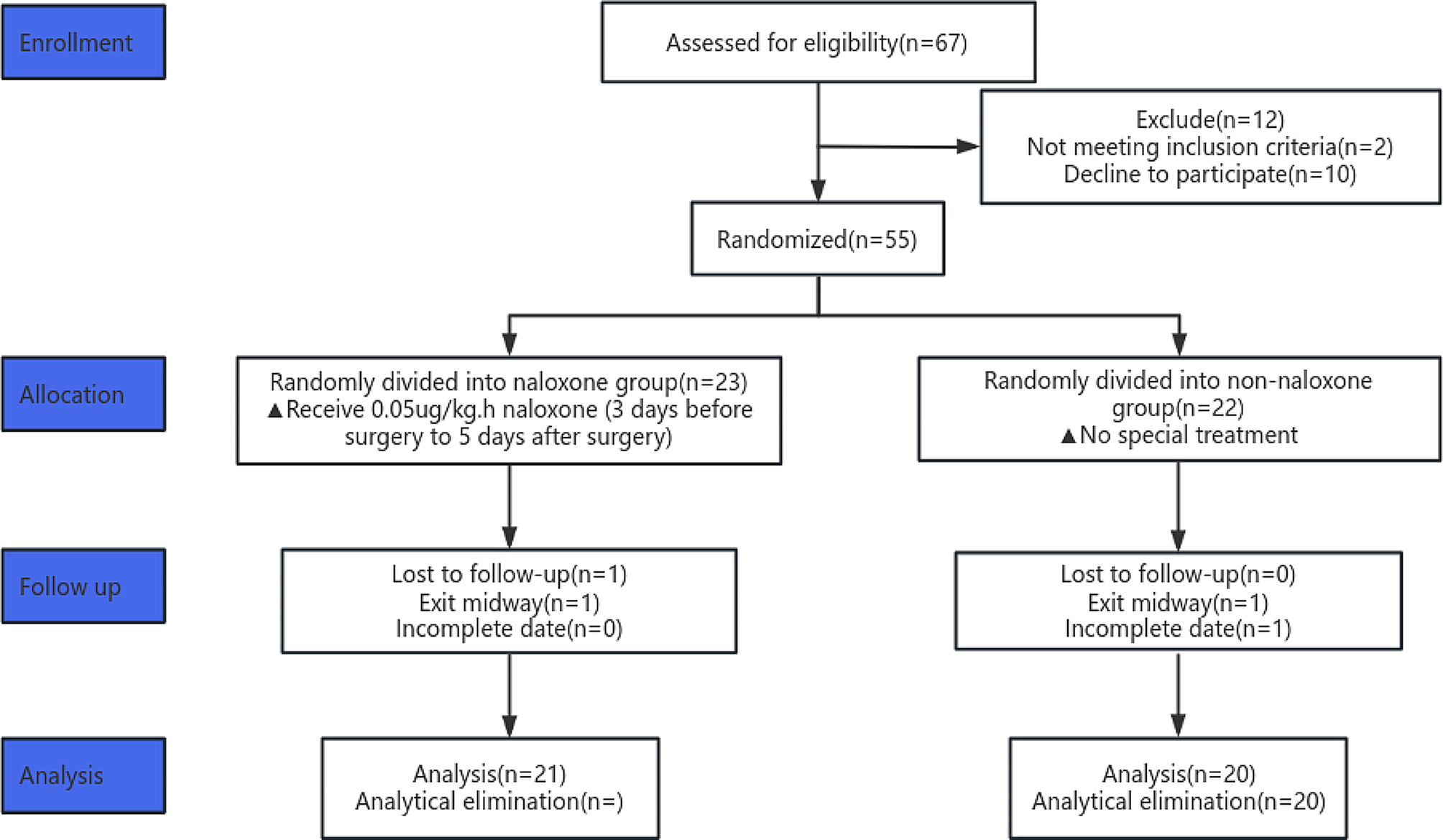
Regarding the flow of the participants through the study, out of 95 patients assessed for eligibility, forty-five cases were omitted (38 didn’t fulfill the inclusion criteria, and seven refused to participate). Fifty patients received the allocated intervention, and six were lost to follow-up (Fig. 1).
Fig. 1
Flow diagram for the included and excluded patients
Clinical assessmentThe included patients were subjected to detailed history and neurological assessment to confirm the diagnosis of lumbar disc prolapse.
Pain severity and functional disability were assessed using the Numeric Rating Scale (NRS) and Functional rating index (FRI) by a skilled neurologist before as well as two weeks, 1, 3, and 6 months after the radiofrequency.
NRS is an 11-point numeric scale used to assess pain severity (0–10), where 10 indicates the worst possible pain, and 0 indicates no pain [16].
FRI was used to assess functional disability, including ten items; two concerning pain intensity and eight concerning daily activities. Each item scored from 0 to 4 (no pain to severe pain). The total score ranged from 0 to 100% (no evidence of disability to severe disability) [17].
Interventional pain procedureThe included patients were requested to stop any medications used for the lumbar disc prolapse two days before the interventional pain procedure. At the time of radiofrequency, the selected patient was brought to the operating room and connected to a monitor. The selected patient was placed in a prone position, and a sterile drape was put over the involved back area. Fluoroscopic guidance was used to identify the affected spinal segment(s) and direct the pulsed RF to the targeted DRG in the intervertebral foramen. Pulsed RF offers the advantage of pain control without the tissue destruction and painful sequelae associated with conventional continuous RF. The used device was the Neurotherm NT2000iX. It delivers electrical current in very brief pulses. The recommended protocol involves delivering a current of 50,000 Hz in 20-millisecond pulses, at a frequency of 2 per second. The relatively long pause between pulses allows any heat generated to dissipate and thus prevent the development of any thermal lesion. This will alter the transmission of pain signals in the nerve without creating a histological lesion [18].
Minimal sedation was done using 0.02 mg/kg midazolam intravenously. 1% lidocaine was infiltrated into the skin at the site of injection. RF needle (22 G, 10 cm, curved, with a 10 mm active tip) was inserted into the targeted location, and the position was verified using fluoroscopic lateral and AP views. The final definite position of the radiofrequency probe was determined by sensory stimulation (50 Hz), producing numbness in the radicular pain distribution. Motor stimulation was done at 2 Hz to avoid injury of the anterior nerve root. Pulsed RF was performed at 42 °C for 120 s twice. After RF lesioning, we confirmed the location inside the epidural space by examining the spread pattern of contrast. Then, we injected a total dose of 80 mg of methylprednisolone acetate with 2 ml of 1% lidocaine. After the procedure, the patient is monitored and managed for any possible procedural complications such as neural trauma, dysesthesia, paresthesia, or haematoma formation.
Laboratory assessmentQuantitative determination of serum S100B levelIt was done one day before the radiofrequency procedure by applying a sandwich enzyme-linked immunosorbent assay (ELISA) (MyBioSource com. Catalog No: MBS3503148). We carried out the assay at the clinical pathology department on an automated ELISA platform at Beni-suef University hospital.5mL of venous blood was collected from the participants in a plain tube. Centrifugation of blood samples at 1000 rpm speed for 15 min was done. The supernatant serum was collected and stored at -20 C for the assay. We applied 100 µL of standard or serum samples into each well, then incubated at 37 C. for 90 min. The liquid was removed, 100µL Biotinylated Detection Ab was added to each well and incubated for 60 min at 37 C. The wells were washed four times with a wash solution (Phosphate _ Buffered Saline, PBS, pH 7.4). We added 100 µL of Avidin-horseradish peroxidase (HRP) conjugate to each well and incubated for 30 min at 37 C. Each well was washed five times by adding a Washing Solution. We applied 90µL of Substrate Reagent to each well, covered and incubated for 15 min at 37 C. The last step, We added 50 µL of Stop Solution to each well and read the optical density at 450 nm within 5 min.
Validity of the ELISA techniques for S100BThis kit recognizes Human S100B in samples. No significant cross-reactivity or interference between Human S100B and analogues was observed.
ReliabilityCoefficient of variation (CV) is < 10%. Intra-assay Precision (Precision within an assay): 3 samples with low, mid range and high level Human S100B were tested 20 times on one plate, respectively. Inter-assay Precision (Precision between assays): 3 samples with low, mid range and high level Human S100B were tested on 3 different plates, 20 replicates in each plate.
Quantitative determination of serum BDNF levelIt was done one day before the radiofrequency procedure by applying a sandwich ELISA technique (MyBioSource com. Catalog No: MBS700602). We carried out the assay at the clinical pathology department on an automated ELISA platform at Beni-suef University Hospital. 5 mL of venous blood was collected from the participants in a plain tube. Centrifugation at 1000 rpm speed for 15 min was done. The supernatant serum was collected and stored at -20 C for the assay. We applied 100 µL of standard or serum samples into each well, then incubated for two hours at 37 C. The liquid was removed, added 100µL Biotinylated Ab to each well. Incubation for 60 min at 37 C. was done. Washing The wells three times with a wash Solution. We applied 100µL of Avidin-horseradish peroxidase (HRP) conjugate to each well and incubated for one hour at 37 C. Each well was washed five times by adding a Washing Solution. We applied 90µL of TMB Substrate to each well, covered and incubated it for 15 min at 37 C. The last step, We added 50 µL of Stop Solution to each well and read the optical density at 450 nm within 5 min.
Validity of the ELISA techniques for BDNFThis assay has high sensitivity and excellent specificity for detection of human BDNF. No significant cross-reactivity or interference between human BDNF and analogues was observed.
ReliabilityIntra-assay Precision CV%<8% and Inter-assay Precision CV%<10%.
Outcomes of the studyThe primary outcome was to investigate the potential role of S100B and BDNF in predicting outcomes from using radiofrequency in treating lumbar disc-related radicular pain. Such laboratory biomarkers were known to be potentially impacted in lumbar disc prolapse, so they were expected to have a predictive value of outcome from treatment.
The secondary outcome was to study the role of age, duration of pain, number of prolapsed discs, pain intensity, and functional disability before radiofrequency, in predicting the outcome of using radiofrequency in treating lumbar disc-related radicular pain.
Sample sizeThe sample size was calculated using G*Power version 3.1.9.7 Software based on the provisional results of a pilot study before starting the current study. The probability of type I error (α) was 5%, effect size = 0.463, critical t = 2.011, df = 48, and non-centrality parameter λ = 3.69. So, a sample size of 50 patients was requisite to attain a statistical power (1–β) of 95%.
Statistical analysisIBM SPSS Version 25 was used to analyze the data. Categorical variables such as sex and degree of the most prolapsed disc were presented as numbers and percentages. Quantitative variables such as age, duration of pain, number of prolapsed discs, NRS and FRI were presented as mean and standard deviation (SD). Paired sample t-test was used to compare pre-and post-interventional NRS and FRI. Pearson correlation was used to test the relationship between the included patients’ age, clinical, imaging, and laboratory characteristics and both NRS and FRI 6 months after radiofrequency. A multiple linear regression model was done to identify predictors of NRS and FRI 6 months following radiofrequency after being adjusted for their potential mutual confounding effect. Age, duration of pain, number of prolapsed discs, NRS and FRI before radiofrequency, and BDNF and S100B serum levels before radiofrequency were used as the independent variables. P-value ≤ 0.05 was considered statistically significant. All tests were two-tailed.
留言 (0)