The Induction/Consolidation Setting
While many studies have used MRD as a primary endpoint, few have incorporated MRD as part of the study design to investigate treatment efficacy, duration, and/or the transition to maintenance therapy.
One of the most influential recent studies, the MASTER trial (NCT03224507) [18] was a multicenter single-arm phase II study in the US. Here, a response-adapted platform was utilized to modulate frontline therapy. In 123 NDMM patients treated with Daratumumab, Carfilzomib, Lenalidomide, and Dexamethasone (Dara-KRD), MRD was tested post-induction (4 cycles), post autologous hematopoietic stem-cell transplantation (post-ASCT) and every 4 cycles of consolidation (maximum 8 cycles). Participants who reached 2 consecutive MRD-negative tests stopped treatment and began observation with MRD surveillance (MRD-SURE). 71% reached 2 consecutive MRD negativity, entering treatment-free surveillance. The two-year progression-free survival was 87%. Among those who achieved MRD-SURE, the 24-month cumulative incidence of progression after stopping therapy was 9% for individuals with no high-risk chromosomal abnormalities (HRCAs) such as t(4;14), t(14;16), or del(17p), 9% for those with one high-risk (HRCA), and notably, 47% for those with two or more HRCAs. Notably, there was no strong association between achieving MRD negativity after induction therapy or post-ASCT and progression-free survival, even with using a threshold of 10–6.
With longer follow-up, MASTER also showed that MRD resurgence precedes disease progression, highlighting the necessity to study early intervention. Some issues with the study include that with MRD-SURE, the time interval between negative MRD tests may have been too short to capture MRD dynamics and may have led to premature de-escalation of therapy. This played the largest role for those with the highest risk of disease in the study (2 + HRCA) who were not well-served by cessation. The suggestion here is that at least for standard-risk disease, MRD-adapted induction and consolidation is feasible and efficacious. However, we would also argue that in those with ultra-high risk disease, even lengthening the duration of the same therapies may not be the answer to overcoming intrinsically biologically resistant and aggressive disease features. With this in mind, these patients likely would still have poor outcomes with more extended therapy and, in the future, will likely benefit from more aggressive or multimodal (e.g., immunotherapeutic) combinatorial approaches [40].
A multicenter phase II clinical trial (NCT02969837) [41] conducted by Derman and colleagues in the US enrolled 46 NDMM patients treated with elotuzumab and weekly carfilzomib, lenalidomide, and dexamethasone (Elo-KRD) without ASCT. MRD (10–6) by NGS was used to guide the duration of Elo-KRD and the transition to Elo-RD (no carfilzomib) until disease progression. 19 out of 43 (44%) patients achieved two consecutive MRD-negative assay after cycles 8 and 12 and were transitioned to maintenance. Patients who achieved MRD-negativity at 12 cycles received 6 additional Elo-KRD cycles and patients who remained positive after 12 cycles received an additional 12 Elo-KRD cycles before transitioning to maintenance. Patients who achieved MRD negativity (10–6) by cycle 8 (C8) displayed remarkable 3-year progression-free survival (PFS) and overall survival (OS) rates, with estimates of 92% and 100%, respectively. For those with standard-risk disease, the 3-year PFS rates were 86%, while those with high-risk disease experienced a 3-year PFS rate of 61%. Similarly, the 3-year OS rates for standard-risk patients were 91%, whereas patients with high-risk disease had a 3-year OS rate of 64%. These data demonstrate the feasibility of response-adapted therapy and recapitulate the data seen in MASTER regarding the standard-risk patient population such de-escalation is best suited to assisting. The question remains as to whether those with high-risk disease and residual disease after a course of combination therapy should be subjected to repeated cycles of the same therapy or explore an alternate approach.
Based on these data, as well as robust prospective and retrospective analyses, our main adaptive use of MRD in the frontline setting is to inform the decision to pursue ASCT as a consolidation strategy. We first draw on the data from IFM-2009 and DETERMINATION [42] to indicate that frontline, as opposed to salvage, transplantation affords no additional survival benefit. A retrospective analysis of patients in the IFM-2009 study [43, 44] showed that for patients who had achieved MRD-negativity (10–4 sensitivity) before commencing maintenance, PFS outcomes in the transplant vs delayed-transplant arms were similar. Given the results of the IFM-2009 and DETERMINATION studies, we feel that the decision to pursue consolidative ASCT is a discussion between patient and physician considering treatment goals and patient values. The addition of MRD data allows for a more nuanced discussion that indicates that for a patient who has already achieved MRD-negativity, there is little added benefit to consolidative ASCT, and proceeding to maintenance can be elected. To this end, in the MANHATTAN trial, 24 out of 29 (82.7%) patients who achieved MRD-negativity by the end of Dara-KRD induction chose to forego upfront ASCT [45]. The trial also reported 1-year PFS and OS of 98% and 100% respectively.
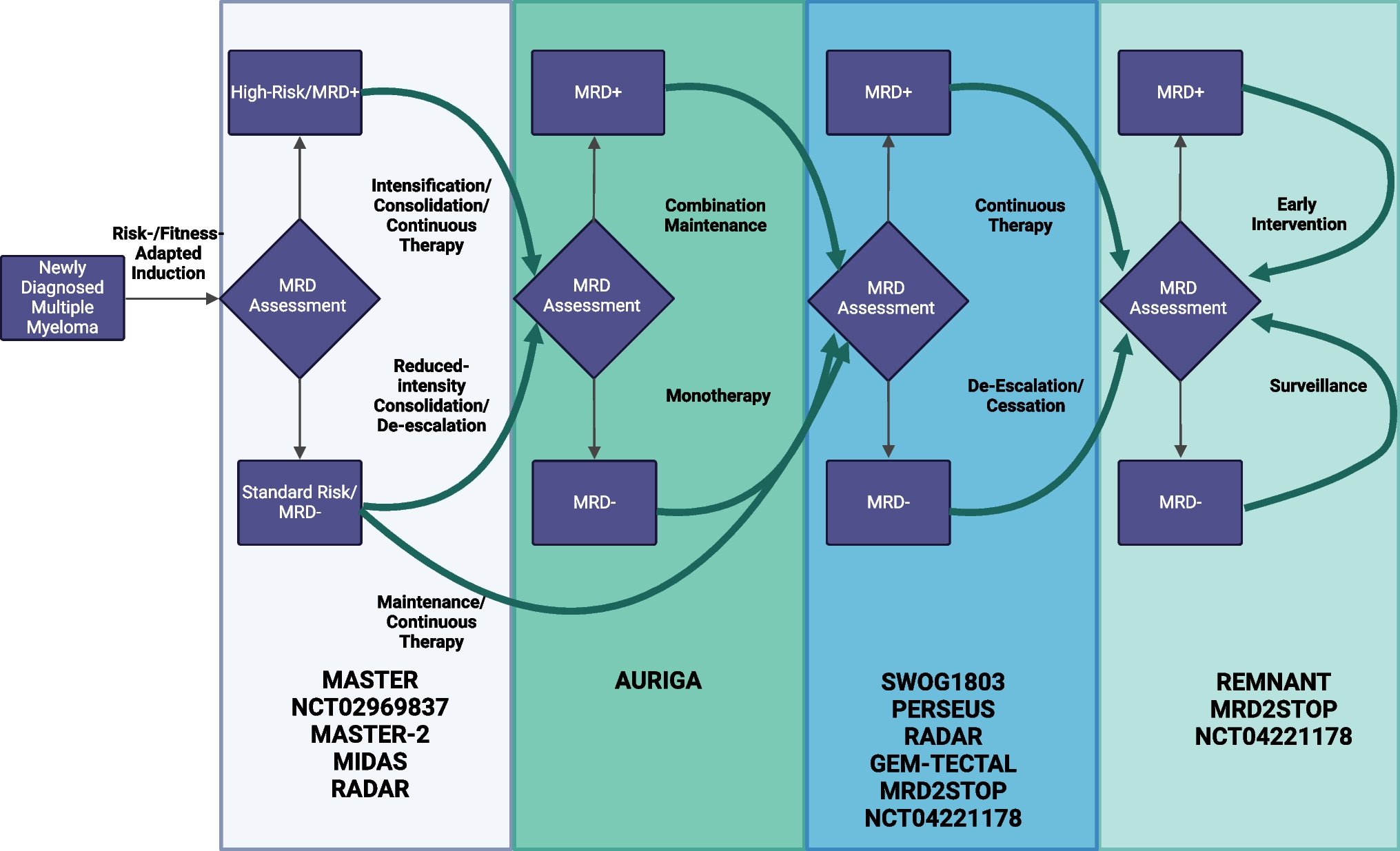
There are several ongoing clinical trials to adapt treatment toward MRD status in the induction/consolidation setting (Table 2). The MASTER-2 trial (NCT05231629) uses a response-adapted approach to consolidative therapy and helps to answer whether the addition of a novel immune therapy can alter outcomes for those with residual disease after efficacious combination induction. All eligible patients receive Dara-VRD induction for 6 cycles followed by MRD testing. The MRD-negative cohort is randomized to consolidation with either of 3 cycles of Dara-VRd followed by 13 cycles of Dara-R maintenance or ASCT followed by 13 cycles of Dara-R maintenance. The MRD-positive cohort is randomized to ASCT intensification, 3 cycles of Dara-Teclistamab consolidation, and 13 cycles of Dara-Teclistamab maintenance or ASCT intensification, 3 cycles of Dara-R consolidation, and 13 cycles of Dara-R maintenance. The MIDAS trial (NCT04934475) is a phase 3 clinical trial that aims to enroll 761 patients for induction with Isatuxamab-KRD followed by randomization to 4 arms based on MRD status measured by NGS (10–6). Subsequent 3-year maintenance includes Revlimid (arm A, B) or Isa-Iberdomide (arm C, D).
The Maintenance Setting
In current clinical practice, a paradigm of maintenance therapy until progression has become dominant, at least in the US. The rationale for the benefit of lenalidomide maintenance was established in a time of less efficacious frontline therapy. In fact, three main studies leading to our current practice were predicated on induction with therapies not reflective of current practice patterns [46,47,48]. Given advances in induction regimens, the benefit of continuous maintenance for all patients may be less clear. In the absence of updated randomized data with modern frontline combination therapies, and with the advent of more tolerable and less frequently administered therapies (i.e., antibody-based therapies), MRD-adapted maintenance therapy may better individualize maintenance strategies. MRD is being used as a tool to determine the intensity of maintenance as well as provide insights into de-escalation or even cessation. While we do not yet have strong prospective data to determine whether MRD can be used to adapt the strength or duration of maintenance, it is important to consider the existing evidence for using MRD and MRD dynamics to guide our approach to maintenance de-escalation, especially given the financial and medical toxicities of indefinite maintenance [49,50,51,52,53].
Myeloma XI [16] is a multicenter phase 3 trial in the UK that showed that MRD is a predictor of survival outcomes at 3 and 9 months post-ASCT (ASCT + 3 and ASCT + 9, respectively). 1,248 post-ASCT patients were randomly assigned to lenalidomide maintenance or observation at ASCT + 3. MRD was assessed by flow cytometry (median sensitivity 4 × 10−5) before maintenance at ASCT + 3 and ASCT + 9. At ASCT + 3, those who achieved MRD negativity had longer PFS compared to those who did not (44 vs 24 months). Furthermore, those who had MRD negativity at ASCT + 9 had prolonged PFS when compared to those who were MRD positive (50 vs 13 months). OS at 3 years increased from 69.5% of MRD-positive patients to 86.9% of MRD-negative patients. Patients who had a deepening response from MRD positive to MRD negative at ASCT + 9 had similar PFS outcomes as patients who were negative at both points. Valuable information has been gained from a recent analysis [54] with an updated follow-up: Landmark analyses revealed a consistent PFS advantage for all-comers at various time points. However, PFS benefits were no longer statistically significant for those patients with MRD-negativity at 3 years. These data suggest that the magnitude of the benefit of extended maintenance for those patients with the deepest long-term responses may not offset medical and financial toxicities.
In a similar vein, NCT02538198 [15] was a single-arm phase 2 clinical trial in the USA that studied the dynamics of MRD in patients on continuous lenalidomide maintenance. 108 patients underwent annual MRD tests by flow cytometry for up to 5 years (1 × 10–5). Most MRD-negative-to-positive resurgences happened within the first 2 years and no progression events were recorded for those who maintained sustained MRD negativity at a 2-year landmark analysis. Additionally, patients who experienced an MRD resurgence exhibited inferior outcomes compared to those who maintained a stable MRD-positive response, signifying imminent disease progression. Importantly, other studies on MRD dynamics below have conversely reported similarly poor outcomes for those with both persistent MRD-positivity and conversion from -negative to -positive state. In a separate study by Mohan et al., [55] a retrospective cohort of 568 patients who were in deep remission [achieved sustained MRD-negativity post-ASCT at least 3 months apart, had negative PET-CT or whole-body MRI and sustained a very good partial response of higher] and were receiving immunomodulator plus proteasome inhibitor for maintenance (IMiD plus PI). The findings revealed that, during a median follow-up of 9.9 years from diagnosis, 61% of patients maintained MRD negativity, while 39% had MRD resurgence at a median of 6.3 years subsequently leading to a clinical relapse within a median of 1.0 years. The study identified that the highest risk of MRD resurgence occurred within the initial 5 years post-treatment and extended up to 15 years from the time of diagnosis. Notably, only 27% of those with MRD resurgence had not experienced clinical relapse at a median follow-up of 9.3 years. These studies highlight both the potential of MRD assessment to detect imminent progression (~ 1 year at 10–5) and also call into question the utility of continuous maintenance for those with durable and prolonged sustained MRD-negative responses.
Two simultaneously published analyses examined MRD resurgence [56,57,58]. In an analysis from the FORTE study, some important findings included that of 118 patients who lost MRD-negativity: 1) 1-year sustained MRD-negativity had been previously achieved by 36%; 2) 16 patients with a recent MRD-negative assay had skeletal/extramedullary relapse without biochemical progression; 3) median time from MRD resurgence to biochemical progression (at 10–5) was 22.3 months. Features associated with unsustained MRD-negativity included HRCA, baseline high circulating tumor cell burden, late timing (i.e., post-consolidation) of MRD-negativity, and monotherapy (R) maintenance (vs. KR). The second report was a combined analysis of GEM2012MENOS65 and GEM2014MAIN. GEM2014MAIN51 de-escalated maintenance therapy based on MRD status at 2 years. Patients were randomized following GEM2012menos65 (VRD induction with busalfan/melphalan vs melphalan ASCT) onto maintenance with either of Ixazomib Plus Lenalidomide/Dexamethasone (IRd) vs Rd maintenance. At 2 years, those with MRD-negativity by MFC (sensitivity 3 × 10–6) would stop maintenance and those with residual disease would continue Rd. Parallel findings to the aforementioned FORTE analysis included: 1) Median PFS from MRD resurgence to progression or death was 39 months; 2) 47% who had MRD resurgence had previously sustained MRD-negativity; and 3) Late achievement of MRD- and 4) high baseline circulating tumor cells were similarly seen to be associated with MRD resurgence. Furthermore, a higher level of MRD at the time of resurgence (i.e.; < 10–5, in between ≥ 10–5 and < 10–3, and ≥ 10–3) was associated with worse PFS. Contrary to the FORTE analysis, however, high ISS was associated with MRD resurgence while HRCA (aside from 1q +) was not. Additionally, an interim report of 332 patients on GEME2014MAIN revealed that while there was no PFS benefit to the addition of ixazomib in the maintenance setting, those with MRD-negativity at 2 years that had discontinued therapy had lower rates of relapse than those with positive MRD, despite the fact that the latter group received an additional 3 years of extended therapy [59]. Altogether, these studies emphasize that the duration and the depth of sustained MRD-negativity will need to be revisited depending on baseline risk factors and the nature of any planned intervention (i.e., de-escalation/cessation).
A recent combined analysis of TOURMALINE-MM3 and -MM4 [13], in which transplant-eligible and ineligible patients (total n = 1280), were randomized to 2 years of ixazomib maintenance vs placebo provides more granularity into MRD dynamics on maintenance. Patients with CR (and/or VGPR in MM3) had MRD testing by flow cytometry (estimated sensitivity 4 × 10−6 with 5 million cell acquisitions) at randomization, 14 months, and end of treatment (∼24 months). The pooled analysis revealed several important findings. First, patients who were MRD-negative at enrollment had similar outcomes whether they received maintenance or placebo with 2-year PFS rates of 67.2% and 61.7% (p = 0.288). Second, about half of MRD resurgence happened within 2 years of starting maintenance, and resurgence was associated with an increased risk of progression in a 14-month landmark analysis compared to those with sustained MRD-negativity (34.2 vs 75%). Third, those with persistent MRD-positivity at 14 months had the worst outcomes with a PFS rate of 27.6%. This data pertains to upcoming trials investigating early intervention with treatment intensification when minimal residual disease (MRD) reappears. While ixazomib maintenance is no longer a relevant treatment modality, the combined analysis further emphasizes the importance of MRD dynamics, rather than MRD status assessed at a single time point, in the maintenance setting.
An important interim analysis comes from the ATLAS trial [60] in which NDMM patients were randomized following ASCT to maintenance with either up to 36 cycles of KRD or Revlimid alone. The risk and response-adapted study design allowed patients in the KRD arm to de-escalate to lenalidomide monotherapy after cycle 6 provided they had standard-risk cytogenetics and MRD-negativity was reached (IMWG 10–5). In the interim analysis of 180 patients, 35 patients met de-escalation criteria and compared to 20 patients in the lenalidomide monotherapy arm, there was a PFS benefit to combination maintenance/de-escalation (HR 0.25) providing evidence that MRD-adapted therapy can be efficacious while reducing excess toxicity of combination regimens.
Looking forward with these de-escalation data in mind, two prospective trials aim to determine the safety and efficacy of maintenance cessation. MRD2STOP [12] allows patients who have received at least 1 year of maintenance and are negative for residual disease by PET-CT, flow (10–5), and NGS (10–6) to discontinue maintenance under careful observation. Of note, one innovation is the prospective assessment of CD138 enriched bone marrow aspirate with NGS to achieve MRD sensitivity of 10–7. Preliminarily, 84% of enrolled patients sustained MRD-negativity at 10–6 1 year after enrollment and discontinuation. In preliminary data from a study being conducted by Korde et al., [14] patients who sustained MRD negativity by MFC for 3 years transitioned to close surveillance with BM MRD testing every 6 months and an annual PET-CT. The rates of sustained MRD negativity at 6 months and 12 months are reported as 94% and 88%, respectively. Here, the protocol recommends that for patients who convert to MRD positivity, [lenalidomide] maintenance should be re-initiated.
Based on the data presented here, we may develop individualized plans for the duration of therapy. Generally, our strategy in both fit and frail patients is to provide continuous [maintenance] therapy until progression. For those patients who feel their quality of life would be improved by ceasing therapy, we use MRD to guide cessation. The strongest evidence as indicated by the above studies, is for modulating the length of lenalidomide maintenance in fit patients. Our first recommendation for those seeking a treatment holiday is to do so on a clinical trial. In the absence of trial availability, for patients with sustained MRD-negativity for at least 2 years (and imaging is negative for active disease) we may stop lenalidomide maintenance under careful observation. Monitoring plans are individualized but at the least consist of serum paraprotein surveillance to monitor for biochemical relapse but ideally include serial marrow MRD assessment.
Further ongoing clinical trials are in place to adapt treatment towards MRD status [17, 55] (Table 2).








留言 (0)