
記住我



Health literacy (HL) describes a patient's comprehension of their medical condition and the ability to make decisions about their care.1 Previous studies have illustrated limited HL in orthopaedic trauma patients and that educational intervention by the treating orthopaedic team can make a difference.2–4 A systematic review by Berkman et al linked low HL in elderly patients with poorer overall health status and increased all-cause mortality.5 There is currently no literature investigating geriatric HL as it relates to post-acute care (PAC) and subsequent outcomes or length of stay (LOS).
PAC services include skilled nursing facilities (SNFs), inpatient rehabilitation facilities (IRFs), and home health services (HHSs) used after an inpatient hospital stay.6 PAC has become an integral part of the healthcare system, providing extended rehabilitation and care to transition patients back into the community. PAC accounts for notable healthcare expenditures, but there is large variation in quality and outcomes. In 2017, Medicare spending for all PAC services totaled 58.9 billion.6,7 Despite this notable cost, 6-month mortality after hip fracture remains as high as 30% and Medicare patients have poorer functional outcomes and longer LOS in PAC compared with those with private insurance.8,9
To ensure appropriate use of PAC, Medicare mandates that all new admissions are assessed by a provider (physician, nurse practitioner, or physician assistant) who then develops and communicates a care plan within 8 days. The care plan should include health goals and specific steps to reach them, and all patients/families have the right to participate in care planning.10 Despite this, many geriatric fracture patients arrive for their first orthopaedic follow-up with minimal knowledge of their facility or treatment plan. Our objective was to investigate patients' and families' HL of their PAC treatment plan and whether intervention by the treating orthopaedic surgeon would after HL or LOS.
MethodsThis study was approved by the institutional review board of our medical center. Orthopaedic trauma patients 65 years and older treated surgically or nonsurgically at a single level 1 trauma center from April 2018 to -November 2020 and then discharged to either IRF or SNF were eligible to participate in the study. Patients with dementia were included if they had family involved in their care and available to participate. Subjects were prospectively enrolled at their first orthopaedic clinic follow-up visit and divided chronologically into two cohorts. The first group enrolled represented the control group. We developed a survey of five questions seeking basic information about the patient's PAC facility and whether that facility met Medicare guidelines for developing a care plan. Subjects completed this survey at their first postoperative visit (approximately 2 to 3 weeks post injury), and the questions included (1) name of the facility, (2) met a provider, (3) met a case manager/social worker, (4) specific goals for discharge (activity, self-care, etc.), and (5) anticipated discharge date. All families were encouraged to assist with the survey, and their participation was recorded. Demographics were also recorded as part of the survey and included race, highest education level, household income, and any history of experience working in health care by either the patient or a family member.
Beginning in January 2019, the second group of patients was prospectively enrolled and served as the intervention cohort. This group was given written and verbal instructions from orthopaedic ancillary staff before hospital discharge, detailing Medicare requirements and important questions to ask upon arrival at their facility. These included their right to provider assessment within 8 days of admission, periodic reassessments, and their right to participate in care planning. Patients and their families then completed an identical survey at their first orthopaedic follow-up appointment.
The primary outcome of this study was the HL score of geriatric fracture patients, with a maximum score of 5 based on the five-question survey. We compared the mean HL scores between the control and intervention groups. A secondary outcome was facility LOS, which was obtained by contacting each facility to obtain a discharge date. A retrospective chart review was performed on all patients to obtain further background information including preinjury ambulatory status and living situation (home alone, home with family, assisted living facility/SNF) as well as weight-bearing status on discharge. Bivariate comparisons were performed with Fisher exact test, Student t-test, and Wilcoxon rank-sum test.
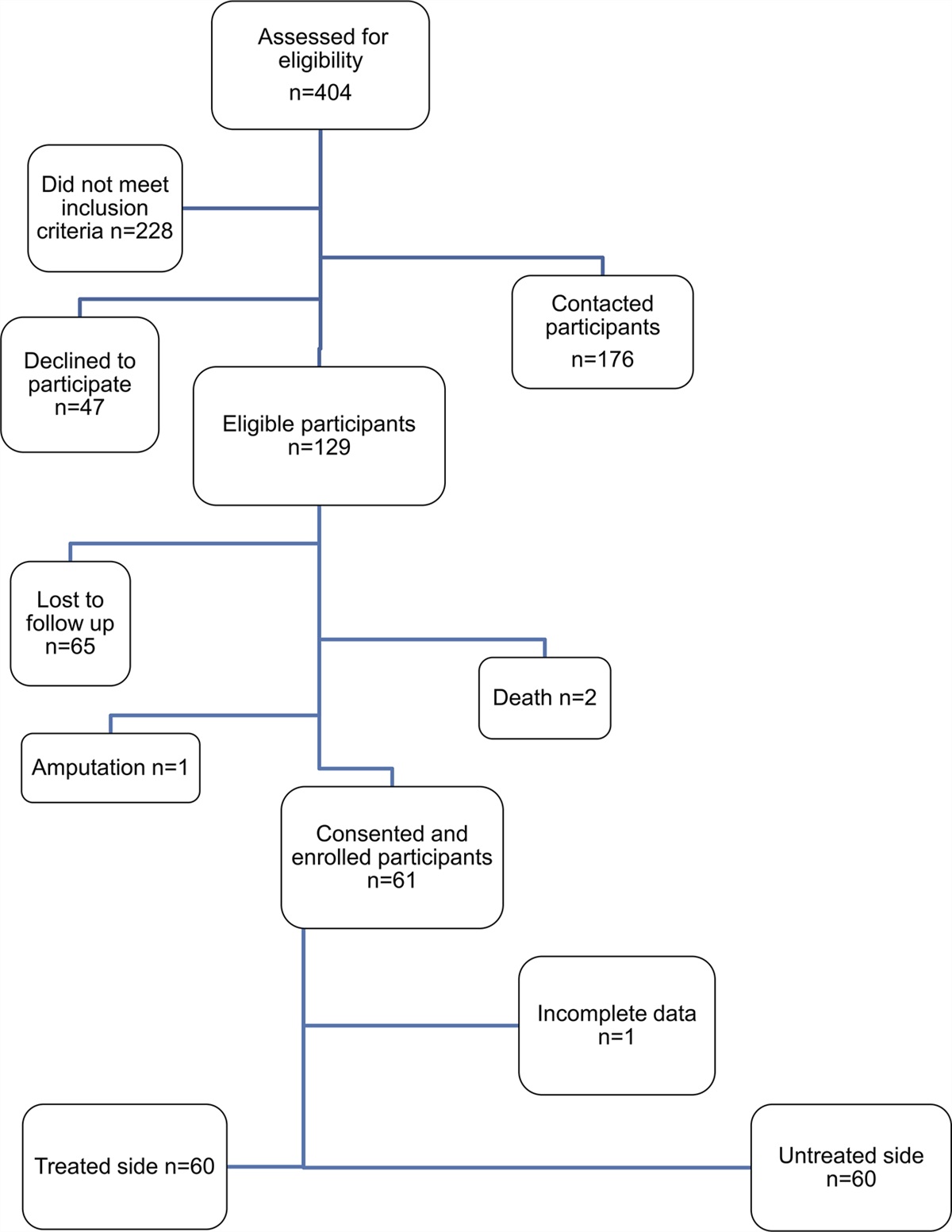
ResultsA total of 207 patients were prospectively enrolled in the study, with 106 and 101 in the control and intervention groups, respectively. The mean age was 79 years (range 65 to 98). The mean HL score for all patients/families was 2.4 of 5. Overall, 93.7% were able to correctly identify the facility, 44.9% met their provider, and 28.0% met their social worker by the time of their first orthopaedic follow-up (approximately 2 to 3 weeks post injury). Only 37.2% could identify goals for discharge, and only 35.7% were aware of their anticipated discharge date (Figure 1). Comparing the control and intervention groups, there were no differences in demographics (age, race, education level, income, healthcare experience) or preinjury functional status. See Table 1. No significant difference was observed in HL score (mean 2.4 versus 2.3, P = 0.49) or facility LOS (median 22 versus 28 days, P = 0.14; Table 2).
 Figure 1:
Figure 1: Graph showing combined survey results including all enrolled participants
Control (n = 106) Intervention (n = 101) P Age, mean (SD) 79 (8) 79 (8) 0.74 Sex, male 22 (20.7) 31 (30.7) 0.11 Race 0.35 White 89 (84.8) 83 (82.2) African American 6 (5.7) 9 (8.9) Latino 5 (4.8) 8 (7.9) Asian 2 (1.9) 1 (1.0) Other 3 (2.9) 0 Education 0.36 < High School 11 (10.4) 13 (13) High School/GED 29 (27.4) 30 (30) Some College 40 (37.7) 28 (28) College grad 15 (14.1) 11 (11) Masters or higher 11 (10.4) 16 (16) Income 0.20 <$5K 1 (1.7) 5 (6.9) $5-10K 6 (10.5) 8 (11.1) $10-20K 17 (29.8) 20 (27.8) $20-30K 7 (12.3) 11 (15.3) $30-50K 8 (14.0) 17 (23.6) $50-80K 9 (15.8) 8 (11.1) >$80K 9 (15.8) 3 (4.2) Health experience 33 (31.1) 29 (28.7) 0.76 Family Assistance 75 (70.7) 65 (65) 0.45 Insurance 0.50 Medicare 104 (98.1) 101 (100) Private 2 (1.9) 0 Previous living situation 0.28 Live alone 34 (32.1) 42 (41.6) With family 55 (51.9) 48 (47.5) ALF/SNF 17 (16.0) 11 (10.9) Previous Ambulatory State 0.27 Wheelchair 8 (7.6) 16 (16.7) Walker 45 (42.9) 37 (38.5) Cane 11 (10.5) 10 (10.4) Ambulatory 41 (39.0) 33 (34.4) Discharge location <0.001 IRF 24 (22.6) 3 (3.0) SNF 82 (77.4) 98 (97.0)Including all 207 enrolled patients, we analyzed the effect of family involvement and type of PAC facility. Family participated in care and completion of questionnaires for 68%. Family involvement led to improved HL scores (2.6 versus 1.9, P < 0.001), but did not affect LOS (median 24 versus 35 days, P = 0.21). See Table 3. Most of the patients (n = 180, 86.9%) were discharged to SNF, with the remaining (13.0%) discharged to IRFs. Those discharged to IRFs had better HL scores (3.4 versus 2.2, P < 0.001), shorter LOS (median 15 versus 30 days, P = 0.2), and trended toward improved knowledge of discharge goals (48.1% versus 35.6%, P = 0.2) than those in SNFs (Table 4).
Table 3 - Health Literacy Scores and Length of Stay, Stratified by Family Involvement Family Involved P Family Not Involved P Control (n = 75) Intervention (n = 65) Control (n = 31) Intervention (n = 35) N (%) N (%) N (%) N (%) Do you know the name of the facility? 74 (98.6) 64 (98.5) 0.919 29 (93.5) 26 (74.3) 0.037 Met the Provider (physician, NP, or PA)? 66 (88) 42 (64.6) 0.001 25 (80.6) 25 (71.4) 0.391 Met a case manager/social worker? 64 (85.3) 56 (86.1) 0.891 22 (71) 26 (74.3) 0.767 Know the goals you must meet for discharge? 27 (36) 32 (49.2) 0.115 6 (19.3) 11 (31.4) 0.270 Do you know how long you will be in the facility? 28 (37.3) 27 (41.5) 0.614 9 (29) 9 (25.7) 0.767 Total, mean (SD) 3.45 (0.93) 3.40 (1.12) 0.760 2.94 (1.23) 2.77 (1.35) 0.610 Length of Stay, Median (Range) 20 (1-498) 28 (8-599) 0.069 36.5 (7-457) 31.5 (3-307) 0.562HL is a facet of orthopaedic care that is vital to optimizing outcomes, but rarely acknowledged.5 Increasing age is associated with lower HL in orthopaedic trauma patients, and among community-dwelling seniors older than 65 years, inadequate HL is an independent risk factor of mortality.4,11 This study illustrates poor overall HL in this population, specifically regarding the common setting of post-acute care. Our results show an overall mean HL score of 2.4 of 5 with particularly poor knowledge of discharge goals (37.2%) and anticipated discharge date (35.7%). In this vulnerable population, family involvement (68%) did markedly improve HL, but overall knowledge of care plans remained poor.
This study highlights the effect of poor HL in the vulnerable geriatric trauma population, particularly as it relates to post-acute care. The effect of PAC on postoperative outcomes has been studied in geriatric arthroplasty and fracture care. Compared with discharge home, patients discharged to PAC facilities after arthroplasty had markedly increased risk of 30-day complications and hospital readmissions.12,13 To control for confounding variables, Owens et al12 conducted multivariate analysis on a database of 34,610 SNF-eligible patients after total joint arthroplasty and found that discharge to SNF versus home was an independent risk factor of adverse outcomes. Of patients admitted to SNFs, longer LOS has also been associated with higher 30-day hospital readmissions in hip fracture patients.14 Although we found no notable difference in LOS from the intervention in this study, patient education by the treating orthopaedic team has been effective in improving HL in other populations.3,4 This may be because of inadequate power, failure to control for confounding variables, or persistently poor communication by PAC facilities. Regardless, it is clear from this study that improving geriatric HL about post-acute care could help expedite our patients' successful return to the community.
Post-acute care is widely used in geriatric fracture rehabilitation, but outcomes vary substantially based on facility. In a prospective study of postoperative hip fracture patients, only 31% were discharged back into the community from SNF within 30 days, and there was a significant difference in successful discharge between high-volume and low-volume SNFs.15 The literature shows that this variation in outcomes extends to differences between inpatient rehabilitation and SNFs. Patients discharged to IRFs following acute stroke or cardiopulmonary illness had superior mobility and self-care at final discharge to those in SNF.16,17 It is widely documented that IRF patients tend to be younger, have fewer comorbidities, higher preoperative function, and fewer in-hospital complications.15,18 However, multiple studies comparing the two facility types using matched control subjects in arthroplasty and hip fracture patients found shorter LOS, better functional scores, and less requirement for assistive device in IRF patients.19,20 In this study, patients discharged to IRF had markedly better knowledge of discharge goals and shorter LOS than those discharged to SNF. Although we did not control for demographics or preoperative function, these results support the literature that there are gaps in quality of post-acute care based on the type of facility, and this disparity extends to patient communication. Another potential factor may be the difference in finances for IRF (days 1 to 60: paid in full by Medicare as a lump sum) versus SNF (days 1 to 20: paid in full by Medicare at a daily rate; days 21 to 100: patient pays $200 per day and Medicare pays the remainder daily; days 100 and beyond: full daily rate is patient’s responsibility to pay) and the possible financial motives that each type of facility may have in providing information and decreasing versus extending LOS.
HL is both a function of the patient's inherent capacity to understand their care and the way in which providers communicate information to them.1 Although the scope of this study did not include a direct assessment of care delivered in PAC facilities, the poor HL scores noted may reflect poor communication by PAC facilities. Medicare mandates a provider assessment and discussion of a treatment plan within 8 days of admission, yet only 37.2% of patients were aware of their goals for PAC discharge by the time of orthopaedic follow-up at 2 to 3 weeks, which may reflect suboptimal communication from facility providers to patients and families.
The primary strength of this study is that it highlights a current deficiency in the care and education of a vulnerable group that may affect health outcomes. However, there are several limitations to this study. The small sample size may have limited power to detect a difference between our control and intervention groups. We were underpowered to detect a difference in surgical versus nonsurgical patients, however, all included patients were limited enough in their mobility or function to be deemed unsuitable for direct home discharge from the hospital. We did not control for patient variables that may be confounding factors in LOS including medical comorbidities, preexisting function, or severity of injury such as polytrauma. Although the five-question patient questionnaire was developed based on Medicare requirements for PAC facilities, it is not a validated survey or scoring system. The study did overlap with the COVID-19 pandemic, which may have had some effect on discharge disposition and LOS.
In conclusion, geriatric fracture patients and families discharged to PAC have poor overall HL regarding their care plans (mean 2.4 out of 5) and long LOS (median 26 days). Family involvement and discharge to IRF showed improved HL scores and decreased LOS, but orthopaedic intervention at hospital discharge had no notable effect. Systemic changes (eg, multidisciplinary coordination of care and patient/family education through programs such as bundled payments) are necessary to improve geriatric HL and PAC and get patients back to their homes and lives as quickly, safely, and economically as possible.
References 1. Baker DW: The meaning and the measure of health literacy. J Gen Intern Med 2006;21:878-883. 2. Kadakia RJ, Tsahakis JM, Issar NM, et al.: Health literacy in an orthopedic trauma patient population: A cross-sectional survey of patient comprehension. J Orthop Trauma 2013;27:467-471. 3. Tsahakis JM, Issar NM, Kadakia RJ, Archer KR, Barzyk T, Mir HR: Health literacy in an orthopaedic trauma patient population: Improving patient comprehension with informational intervention. J Orthop Trauma 2014;28:75-79. 4. Cosic F, Kimmel L, Edwards E: Health literacy in orthopaedic trauma patients. J Orthop Trauma 2017;31:e90-e95. 5. Berkman ND, Sheridan SL, Donahue KE, Halpern DJ, Crotty K: Low health literacy and health outcomes: An updated systematic review. Ann Intern Med 2011;155:97-107. 6. Commission, M.P.A Healthcare Spending and the Medicare Program. Data Book, 2019, pp 1–24. 7. Chandra A, Dalton MA, Holmes J: Large increases in spending on postacute care in Medicare point to the potential for cost savings in these settings. Health Aff (Millwood) 2013;32:864-872. 8. Neuman MD, Silber JH, Passarella MR, Werner RM: Comparing the contributions of acute and postacute care facility characteristics to outcomes after hospitalization for hip fracture. Med Care 2017;55:411-420. 9. Haghverdian BA, Wright DJ, Schwarzkopf R: Length of stay in skilled nursing facilities following total joint arthroplasty. J Arthroplasty 2017;32:367-374. 10. U.S. Department of Health & Human Services: Centers for Medicare & Medicaid Services: Medicare Coverage of Skilled Nursing Facility Care. Baltimore, MD, MEDICARE, 2015. 11. Baker D, Wolf MS, Feinglass J, Thompson JA, Gazmararian JA, Huang J: Health literacy and mortality among elderly persons. Arch Intern Med 2007;167:1503-1509. 12. Owens JM, Callaghan JJ, Duchman KR, Bedard NA, Otero JE: Short-term morbidity and readmissions increase with skilled nursing facility discharge after total joint arthroplasty in a Medicare-eligible and skilled nursing facility-eligible patient cohort. J Arthroplasty 2018;33:1343-1347. 13. Keswani A, Tasi MC, Fields A, Lovy AJ, Moucha CS, Bozic KJ: Discharge destination after total joint arthroplasty: An analysis of postdischarge outcomes, placement risk factors, and recent trends. J Arthroplasty 2016;31:1155-1162. 14. Kumar A, Rahman M, Trivedi AN, Resnik L, Gozalo P, Mor V: Comparing post-acute rehabilitation use, length of stay, and outcomes experienced by Medicare fee-for-service and Medicare advantage beneficiaries with hip fracture in the United States: A secondary analysis of administrative data. Plos Med2018;15:e1002592. 15. Gozalo P, Leland NE, Christian TJ, Mor V, Teno JM: Volume matters: Returning home after hip fracture. J Am Geriatr Soc 2015;63:2043-2051. 16. Hong I, Goodwin JS, Reistetter TA, et al.: Comparison of functional status improvements among patients with stroke receiving postacute care in inpatient rehabilitation vs. skilled nursing facilities. JAMA Netw Open 2019;2:e1916646. 17. Vincent HK, Vincent KR: Functional and economic outcomes of cardiopulmonary patients: A preliminary comparison of the inpatient rehabilitation and skilled nursing facility environments. Am J Phys Med Rehabil 2008;87:371-380. 18. Xian Y, Thomas L, Liang L, et al.: Unexplained variation for hospitals' use of inpatient rehabilitation and skilled nursing facilities after an acute ischemic stroke. Stroke 2017;48:2836-2842. 19. Walsh MB, Herbold J: Outcome after rehabilitation for total joint replacement at IRF and SNF: A case-controlled comparison. Am J Phys Med Rehabil 2006;85:1-5. 20. Herbold JA, Bonistall K, Walsh MB: Rehabilitation following total knee replacement, total hip replacement, and hip fracture: A case-controlled comparison. J Geriatr Phys Ther 2011;34:155-160.
留言 (0)