
記住我








This study was a prospective study of patients with uncontained medial proximal tibial defects undergoing primary TKA between March 2015 and March 2020. Written consent from participants was obtained, along with approval from the institutional review board (IRB). Surgeries were performed by a single surgeon (A.A.D.).
Inclusion criteria were patients with Kellgren and Lawrence grade 4 (KL4) OA with varus deformity and uncontained medial proximal tibial defects ≥ 10 mm deep after the proximal tibial cut. Patients should have completed at least 36 months of follow-up to be included.
Patients with previous knee surgery, valgus OA, rheumatoid arthritis, infection, osteonecrosis, defects after tumor resection, contained defects, associated significant distal femur defects, Charcot knee, defects less than 10 mm depth, or use of metal augmentations were excluded.
Preoperative assessmentHistory taking was done, including analysis of symptoms of pain, stiffness, instability, up-stairing, down-stairing, gait, and rising from chair. The body mass index (BMI) was calculated, and patients were classified based on the World Health Organization (WHO) classification [17] as underweight (BMI < 18.5 kg/m2), healthy (18.5–24.9 kg/m2), overweight (25–29.9 kg/m2), and obesity class I (30–34.9 kg/m2), class II (35–39.9 kg/m2) or class III (≥ 40 kg/m2).
Complete limb examination was done with assessment of the varus deformity regarding the degree, whether correctable or fixed, and the associated deformities (flexion or rotatory). Additionally, the mediolateral instability and the lateral ligament laxity were assessed. Active and passive ranges of motion and patellar tracking were also evaluated.
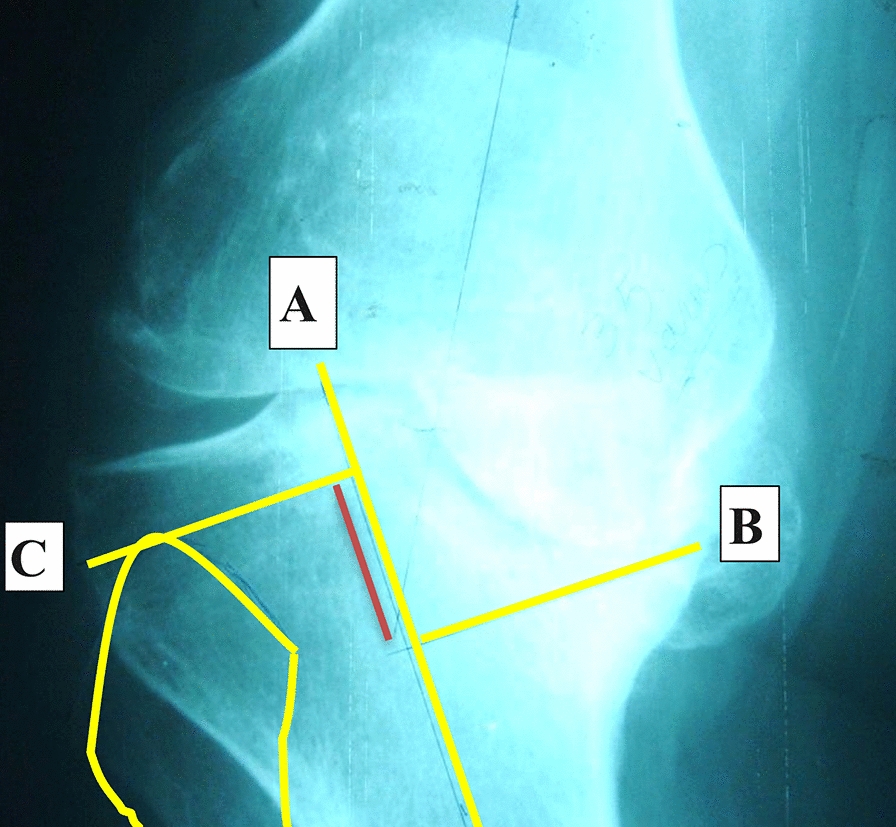
Knee anteroposterior (AP) and lateral standing plain X-rays were done to confirm the clinical diagnosis of advanced arthritis and assess the site, size, containment, shape, and slope of the bone defects. The depth of bone defect from the expected level of the proximal tibial cut was preliminary assessed in the preoperative AP X-ray, Fig. 1.
Fig. 1
Knee plain X-ray AP view showing measurement of the medial tibial defect. Line A is through the anatomical axis of the tibia. Line B passes through the deepest point of the defect and is perpendicular to line A. Line C passes through the highest point of the head fibula and is perpendicular to line A, representing the expected resection line of the tibial plateau. The red line is the size of the defect
Long-film AP weight-bearing X-ray was done to evaluate the anatomical and mechanical axes and quantify the degree of varus deformity by measuring the anatomical femorotibial angle (aFTA).
Additional X-rays included a skyline view at 30 degrees flexion for evaluation of the patellar maltracking and stress views for evaluation of the coronal instability due to bone stock loss or ligamentous insufficiency.
Surgical techniqueSurgeries were done under combined epidural and spinal anesthesia. A standard medial parapatellar approach was used with traditional steps for preparation of the tibia and femur.
The proximal tibia was displaced anteriorly, and the tibial cut was done through the nondeficient lateral tibial plateau which was our reference in tibial cut by using a special stylus adjusted at 10 mm, with either intramedullary or extramedullary alignment guides. The tibial cut was done using an oscillating saw taking 10 mm from nonworn lateral tibial plateau leaving a defect in medial tibial plateau.
Dealing with the deficient medial tibial plateau was done using bone graft blocks from the proximal tibial or distal femoral bone cuts. Firstly, the concave and irregular surface of the defect was flattened by minimal bone removal using the oscillating saw with exposure of healthy bone to enhance further healing with the graft. The depth of the defect was evaluated and measured using a sterilized ruler.
The graft was fashioned using bony rongeur, placed over the flattened defect, and secured provisionally by Kirschner wires (K-wires). The K-wires were then replaced by 3.5 mm cancellous screws, making sure that they did not interfere with the tibial component keel or stem. The protruding part of the graft was then removed by an oscillating saw to create a flat upper tibial surface, Fig. 2.
Fig. 2
Intraoperative images of the bone graft preparation and insertion into the defect. A Evaluation of the defect after the proximal tibial cut. B Placement of the graft into the defect and provisional fixation by two K-wires. C Replacement of the two K-wires with two 3.5 mm partially threaded cancellous screws. D Removing the protruding part of the graft with an oscillating saw to create a flat upper tibial surface
Before cementation, the interface of the bone graft and the tibia was filled by impaction bone graft to avoid the extrusion of cement into this interface.
Trial components were inserted for assessment of size, prosthesis fitting, position, equality of bone gaps, and traditional restoration of neutral mechanical alignment was important as it had great effect on bone graft survival and prosthesis loosening. Tibial stem was used in all cases to protect the bone graft from stress.
The definitive prosthesis was inserted by the routine cementing technique. Posterior-stabilized (PS) TKA with a stemmed tibial component was used to unload the deficient metaphyseal bone. In cases with severe lateral collateral ligament laxity, Legacy Constrained Condylar Knee (LCCK) prosthesis (Zimmer-Biomet, Warsaw, Indiana, USA) was used.
Patelloplasty was done by removing all the osteophytes by the nibbler and denervation of the patella by applying cautery circumferentially around the patella (patellar circumcision).
Good hemostasis was achieved after the release of the tourniquet, followed by closure of the wound after application of a suction drain.
Postoperative care and follow-upEpidural postoperative analgesia was given in the ward using a continuous syringe pump system for sustained analgesia for 48 h postoperatively. Additionally, intravenous antibiotics were given for 48 h postoperatively. Static quadriceps and hamstring muscle strengthening exercises and straight leg raising exercises were commenced from day one, in addition to active and assisted flexion–extension range of motion (ROM) exercises. Weight-bearing was permitted without limitations.
Patients were followed up at 6 weeks, 3 months, and 6 months, then yearly, and were evaluated clinically with Knee Society Score (KSS) [18] and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) [19]. Follow-up knee X-rays were also done at 6 weeks, 3 months, 6 months, and then yearly to assess component stability and bone graft union, Fig. 3.
Fig. 3
A 58-year-old male with advanced left knee OA. A Preoperative X-rays showing advanced OA and the medial proximal tibial defect. B Preoperative standing photographs showing varus deformity. C Postoperative X-rays after TKA using LCCK and reconstruction of the defect using structural autograft block fixed with two screws. D Three-year follow-up X-rays showing complete union of the graft
Statistical analysisData were analyzed using IBM SPSS software package version 20.0. (Armonk, NY: IBM Corp).
Qualitative data were expressed as numbers and percentages. Quantitative data were expressed as mean, and standard deviation (SD) when normally distributed and as median and interquartile range (IQR) when not normally distributed.
Comparison of preoperative and postoperative continuous data was done using the paired samples t-test or the Wilcoxon signed-rank test when appropriate. Comparison of the effect of different variables on the functional and radiological outcomes was done using the Student’s t-test, the Mann–Whitney U-test, the one-way ANOVA, or the Kruskal–Wallis H-test, when applicable. Significance of the obtained results was judged at the 5% level.
留言 (0)