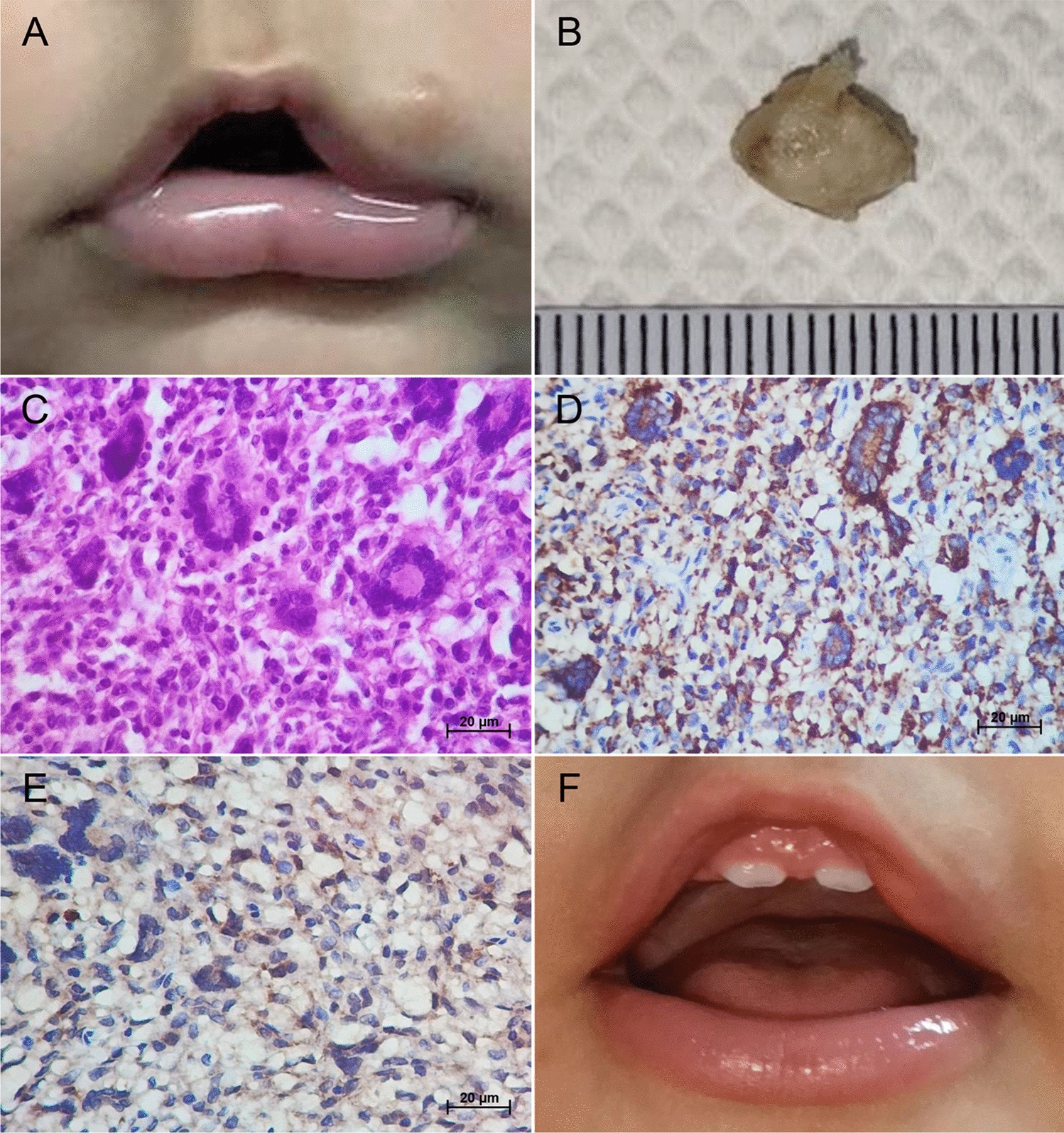
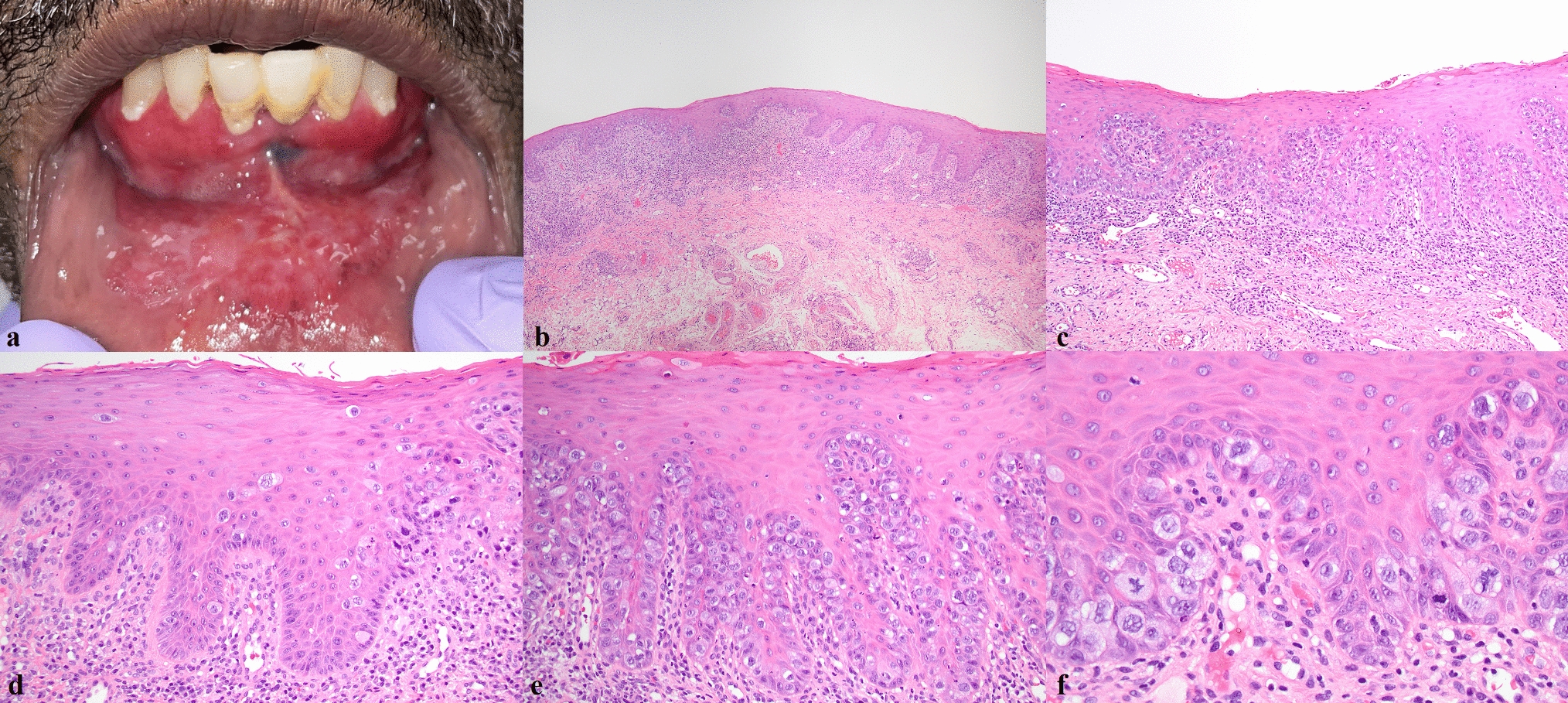
EMPD is exceptionally rare in the oral mucosa, with only nine cases having been reported in the English-language literature, including the present case (Table 1) [6,7,8,9,10,11,12,13]. EMPD has been reported in six males and three females at a median age of 65.5 years old. Clinically, all patients presented with variably erythematous, ulcerated or keratotic lesions bearing resemblance to lichen planus, with an identifiable mass usually absent. Mucosal involvement is typically extensive, ranging from 3.0 to 12.0 cm when measured and sometimes demonstrating pan-mucosal involvement. Nearly any oral mucosal subsite may be involved, with one case documenting perioral skin involvement as well. The extensive presentation of oral EMPD, mimicking an inflammatory process, is comparable to the presentation of PD at mammary and other extramammary sites [2].
Table 1 Clinical characteristics of oral EMPDHistologically, underlying invasive adenocarcinoma was documented in four cases of oral EMPD (diagnosed as anaplastic adenocarcinoma, salivary duct carcinoma, adenocarcinoma not otherwise specified, and poorly differentiated carcinoma). MPD is almost uniformly associated with underlying breast carcinoma, with nipple/areolar involvement representing extension from ductal carcinoma in situ (DCIS) involving underlying lactiferous ducts. EMPD, on the other hand, is accounted for by extension from an underlying primary cutaneous adnexal carcinoma in only approximately 25% of cases [5]. A further 10–15% of patients have carcinoma involving gastrointestinal or genitourinary sites with pagetoid spread of tumor cells into mucocutaneous surfaces of the anogenital region, resulting in a disease presentation classified as secondary EMPD. For the majority of cases of EMPD, however, the pathogenesis remains unclear.
It has been hypothesized that these cases of EMPD as well as rare cases of MPD not associated with underlying breast carcinoma may originate from Toker cells (clear cells of Toker), clear cells occasionally identifiable in the basal layer of squamous epithelium of the nipple and vulva [14, 15]. Toker cells (TC) bear some morphologic resemblance to Paget cells, as well as CK7 immunopositivity, and have been postulated to represent potential precursor cells to PD, though their exact origin and function remain unknown [16]. TC have historically been suggested to represent abortive mammary differentiation or intraepithelial extension of lactiferous duct cells but more recent studies have demonstrated localization of TCs to underlying sebaceous glands instead of to lactiferous ducts [17, 18]. If TCs are indeed related to underlying folliculo-sebaceous/apocrine units instead of to lactiferous ducts, this could potentially help to understand the occurrence of purely intraepithelial PD in the absence of underlying carcinoma, as well as the occurrence of EMPD outside of the milk line, including oral mucosa where sebaceous glands (Fordyce granules) may be present. However, the pathogenesis of primary EMPD remains speculative.
The management of oral EMPD is primarily surgical, frequently complicated by local or occasionally regional recurrence, as is the case for EMPD in general [19]. Tendency for local recurrence is interpreted in light of propensity of pagetoid cells to spread laterally beyond clinically visible disease, as was noted during frozen section examination of the present case. Local recurrence was documented in 5/9 patients with oral EMPD, one of which also demonstrated regional recurrence [6], over periods of 6–48 months. All four patients with invasive carcinoma also underwent radiation therapy and two of these patients also received chemotherapy. The two patients with oral EMPD and an invasive adenocarcinoma component died of disease after periods of 1.5 years and 10 years. One patient with pan-mucosal disease who was not a candidate for surgery and who declined radiation and chemotherapy was administered thalidomide [10]. This patient demonstrated reduction in lesion size over 5 months of therapy and clinically stable disease over 36 months follow-up.
Oral epithelial dysplasia (OED) and melanoma in situ (MIS) are two important differential diagnoses for EMPD. OED, MIS, and EMPD all present as an intraepithelial proliferation of cytologically atypical cells, and EMPD may show surface keratinization, as in this case, further mimicking OED. Accurate diagnosis requires immunohistochemical assessment, which should be considered whenever encountering enlarged, pleomorphic cells with abundant amphophilic cytoplasm. Immunohistochemically, ductal differentiation in EMPD can be demonstrated by expression of low-molecular weight cytokeratins (Cam5.2, CK7), CEA, EMA, AR, and Her2. Conventional squamous and melanoma markers such as CK5/6, p40, S100, and SOX10 are consistently negative (Table 2). It is important to highlight that TRPS1 immunohistochemical marker is commonly expressed in breast carcinoma, MPD and EMPD, as the present case demonstrates, but has been reported to be positive in cutaneous carcinoma in situ as well [20]. More work is needed to determine whether TRPS1 is expressed in OED and whether this may represent a diagnostic pitfall in this setting.
Table 2 Commonly reported immunohistochemical findings in oral EMPDA recently sequenced clinical cohort of vulvar EMPD identified targetable alterations in PIK3CA or ERBB2 in > 25% of patients, raising the possibility of novel therapeutic approaches, though whether these alterations occur in oral EMPD remains to be validated [21]. TP53 mutations were also identified in a subset of that cohort, as was identified in the present case by p53 IHC as diffuse nuclear overexpression in Paget cells. p53-mutant IHC may be a pitfall in the differential diagnosis with OED, in which patterns of p53-mutant immunoexpression have been recently described, including diffuse overexpression in tumor cells, null expression and, rarely, cytoplasmic expression in tumor cells [22]. Careful histologic and immunohistochemical evaluation is necessary for the diagnosis of oral EMPD.
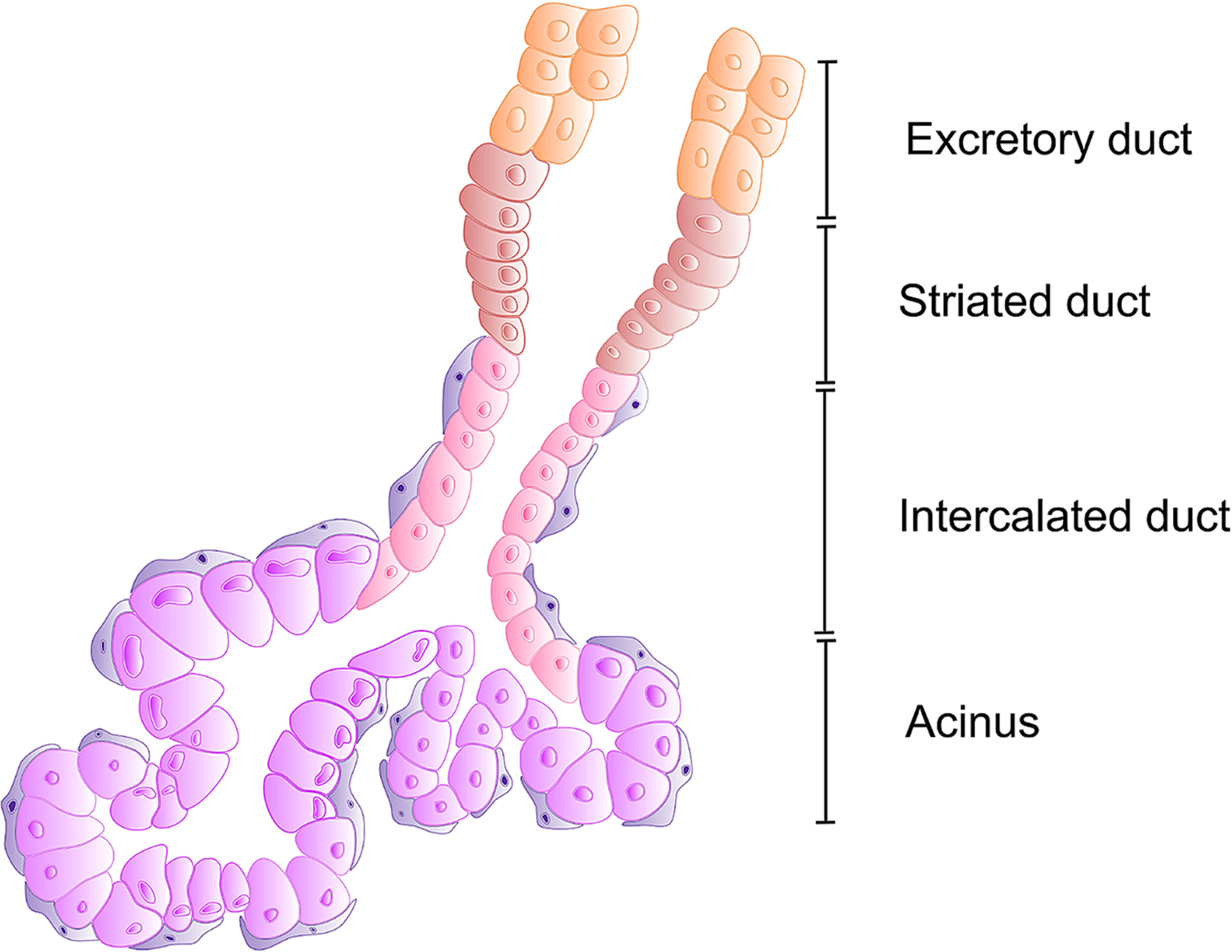
In the present case, extensive involvement of multiple salivary ducts was documented by ADH5 IHC, which demonstrated the intraductal CK7/18 + Paget cells to be surrounded by an intact layer of CK5/14 + and p63 + myoepithelial cells, with no evidence of invasive adenocarcinoma. The involvement of multiple salivary ducts in the present case was interpreted to favor surface origin followed by colonization of multiple salivary ducts, though such a determination remains academic. It is difficult to rule out the possibility of origin within one salivary duct followed by pagetoid surface involvement and then subsequent colonization of adjacent salivary ducts. Intraductal involvement in oral EMPD is not uncommon, having been reported in five cases total, including the present case.
In conclusion, EMPD has been documented exceptionally rarely in the oral mucosa and diagnosis requires familiarity with the diagnosis as well a high index of suspicion in light of significantly more commonly occurring conditions such as lichenoid mucositis and oral epithelial dysplasia. More work is needed to identify targetable alterations in oral EMPD as well as to understand the pathogenesis of cases not associated with an underlying primary adenocarcinoma.






留言 (0)