Study design
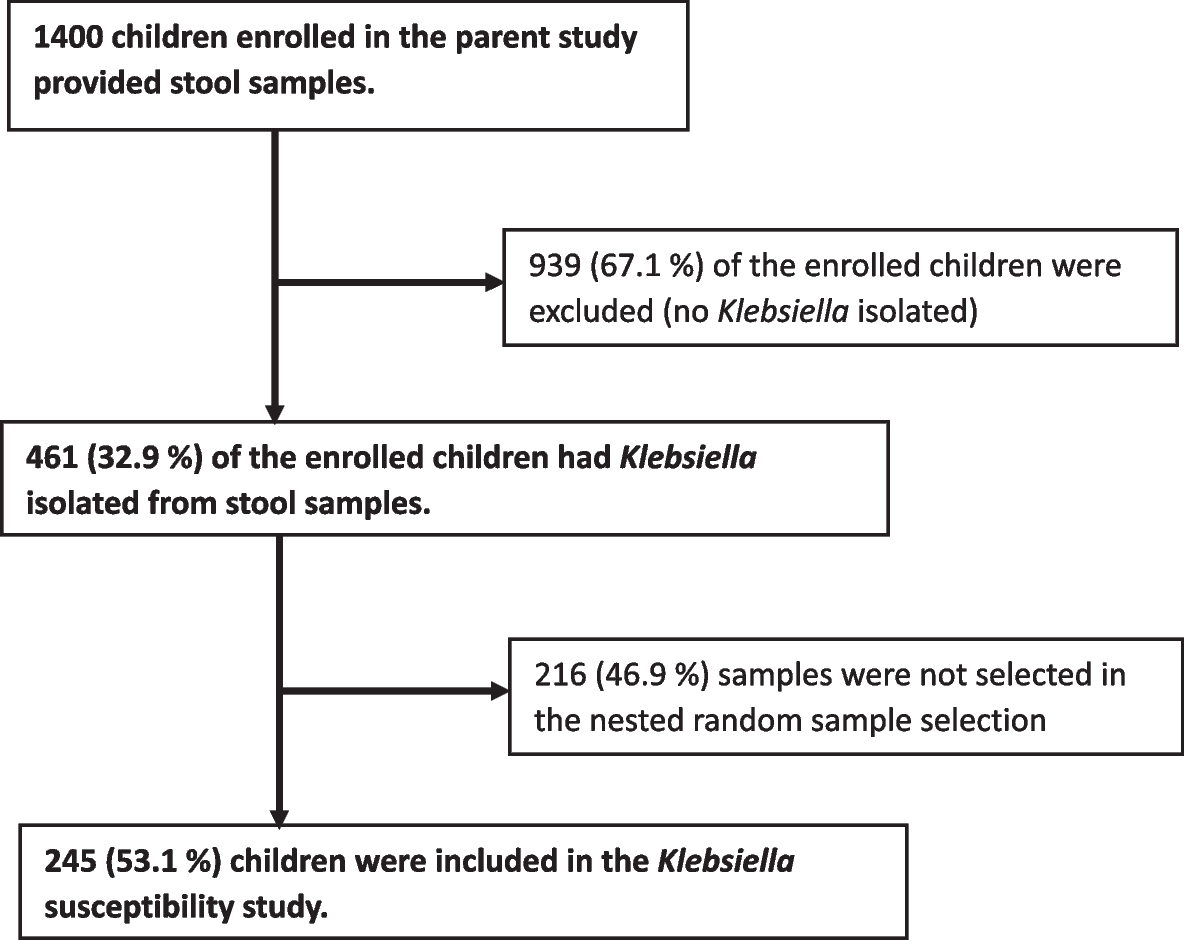
In the parent trial [9], we systematically recruited children aged 1 – 59 months who were discharged from two county referral hospitals in Western Kenya between June 2016 and Nov 2019. In this nested cross-sectional study, we examine Klebsiella isolates collected at enrolment from two county hospitals in Western Kenya. The Kisii Teaching and Referral Hospital is located within the urban center in Kisii town whilst the Homa Bay County Teaching and Referral Hospital is in Homa Bay county. Kisii Teaching and Referral Hospital serves a population of about 1.2 million people with about 220,000 children under five years of age and serves as a major referral hospital in western Kenya [10]. Homa Bay County Teaching and Referral Hospital is classified as a level four healthcare institution, serving a predominantly rural population of around 1.1 million people. Homa Bay county has one of the highest under-five childhood mortality rates and HIV prevalence in the country [11].
Eligibility criteria included children who weighed at least 2 kg, had been hospitalized, recovered, and discharged from hospital, planned to remain in the study area for at least 6 months, had no contradiction to azithromycin, and had not been prescribed any macrolide antibiotics. We excluded children from the study if their hospital admission was solely due to trauma, injury, or birth defect, or if the legal guardian refused consent [9].
Prior to randomization, stool samples were collected from children, processed, and archived. Data on demographics, medical history, underlying medical conditions, clinical examination, and nutritional anthropometry were collected on standardized paper questionnaires by trained study clinicians. In the current nested cross-sectional study, we utilized a random sample of 245 children whose enrollment stool samples had Klebsiella isolated, linked them to clinical data recorded during hospital stay, and demographic and social economic factors collected from the primary caregiver during enrollment.
Sample collection and processing
At enrollment, all children provided whole stool samples, or rectal swabs were used if whole stool collection was not feasible [9]. These samples were preserved in Cary-Blair media to ensure bacterial viability during transportation for microbiological culture. The samples were then promptly shipped to the central laboratory at the Kenya Medical Research Institute-Centre for Microbiology Research (KEMRI-CMR) in Nairobi within a 24-h timeframe. A swab or a sample of stool was streaked on MacConkey (MAC) (Oxoid, United Kingdom) and Eosin Methylene Blue agars (Oxoid, United Kingdom) and incubated in ambient air at 37 °C for 24 h. Morphologically distinct lactose fermenting mucoid colonies were subcultured onto Mueller Hinton (Oxoid, United Kingdom) agar and subjected to API 20E system (bioMérieux, Inc., France) and oxidase reactions for confirmation of Klebsiella spp. Confirmed Klebsiella spp. isolates were stocked in tryptone soy broth supplemented with 15% glycerol (Oxoid, United Kingdom) and frozen at -80 °C. For this analysis, the Klebsiella spp. isolates were thawed, quadrant streaked for isolation onto MAC agar and incubated at 37° C in ambient air to perform antimicrobial susceptibility testing (AST), DNA extraction and genetic characterization.
Antibiotic susceptibility testing
The antibiotic susceptibility profiles of the Klebsiella isolates were determined by the Kirby-Bauer disk diffusion method as described by CLSI [12]. The antibiotics panels used included ceftriaxone (CRO, 30 µg), ceftazidime (CAZ, 30 µg), cefotaxime (CTX, 30 µg), cefoxitin (FOX, 30 µg), chloramphenicol (C, 30 µg), ciprofloxacin (CIP, 5 µg), gentamicin (CN,10 µg), amoxicillin-clavulanate (AMC, 20 µg/10 µg), meropenem (MEM, 10 µg), imipenem (IPM, 10 µg), azithromycin (AZM, 15 µg), and aztreonam (AZT, 30 µg). Zone diameters, measured in millimeters, established by CLSI-2020 M-100 were used to determine susceptibility, resistance, or an intermediate designation [12]. Both intermediate and resistant isolates were classified as non-susceptible [12].
Determination of ESBL–producing Klebsiella spp
ESBL production was determined using the double-disc diffusion synergy test, which utilizes cefotaxime and ceftazidime with and without clavulanic acid [12]. The discs were placed 20 mm apart on a lawn culture of Klebsiella spp. plated on MH agar and incubated at 37 °C for 24 h as described previously [12, 13]. Quality control was assured by simultaneously plating and testing an ESBL-producing Klebsiella strain (ATCC 700603) and an ESBL-negative E. coli strain (ATCC 25922) [13]. ESBL-producing Klebsiella spp. was confirmed if the difference in the zone size between cefotaxime and the zone size of cefotaxime with clavulanic acid was ≥ 5 mm or if the difference in the zone size between ceftazidime and the zone size of ceftazidime with clavulanic acid was ≥ 5 mm as established previously [12].
Genotypic detection of ESBL genes using conventional PCR
Bacterial DNA was extracted from ESBL-producing colonies of Klebsiella spp. using a boiling method. An inoculating loop was placed into bacteria pooled from an overnight culture in MH mixed with 0.5 ml nuclease free water. The cell suspension was heated for 10 min at 100 °C then centrifuged at 15,000 revolutions per minute for 5 min (maintained at 25 °C). The supernatant was used as DNA template for amplification. Extracted DNA was amplified using sets of primers targeting ESBL encoding genes (blaTEM, blaSHV, blaCTX-M, blaOXA) as previously described [14,15,16]. Briefly, a final reaction volume of 25 µl was used in a master mix containing 0.5 µl forward primer (0.2 µM), 0.5 µl reverse primer (0.2 µM), 9.5 µl nuclease free water. A 12.5 µl mix which included Taq DNA polymerase (2.5 units), 1 × PCR Buffer, MgCl2 (0.2 µM), and ultrapure dNTPs (200 µM,) followed by addition of 2 µl template DNA was combined with the PCR master mix. Amplification conditions consisted of 30 cycles of 94°C for 30 s, 50°C, 55 C and 60°C for 30 s, initial extension of 68°C for 1 min and with a final extension step of 68 °C for 5 min [16]. Gel electrophoresis of PCR products was carried out at 200 V on a 1.5% agarose gel, stained with gel red stain and visualized on a Vilber E-Box gel documentation system. All PCR reactions were run with both negative and positive DNA control templates.
Definitions
Detailed descriptions of exposure variables and the derived variables has been provided elsewhere [9]. Briefly, we collected data on sex, child age, study site, HIV exposure, nutritional status, history of exclusive breast feeding, childhood vaccination (included pneumonia, rotavirus, measles, DPT, and BCG), length of hospital stay, antibiotic use during hospitalization, caregiver reported income, caregiver education level, household toilet type, water source and treatment, and household crowding. A household had access to improved water if the caregiver reported access to reliable piped water in the dwelling or community, or if the household primarily used water from a borehole, a protected spring, a well with a pump, bottled water, or rainwater from storage tanks for household chores. Access to treated drinking water was defined as a household whose drinking water is filtered, boiled, or chlorinated before use. Household crowding was defined as a household with more than two individuals sharing a room. The 2006 WHO growth references for children age < 5-years were used to construct anthropometric z-scores. We defined underweight as weight-for-age z-score (WAZ) less than -2SD, stunting as a height-for-age z-score (HAZ) less than -2SD, and wasting as weight-for-height/length z-score (WHZ) less than -2SD. Data on vaccination was derived from childhood vaccination cards if the cards were available at the hospital. However, if the cards were not available, the caregiver provided a report on the child’s vaccination status including the doses taken thus far. We derived an overall vaccine variable that defined children who had completed all essential age-appropriate vaccines, herein referred to “complete age-appropriate vaccination”.
Statistical analysis
We reported the proportion of Klebsiella spp. isolates resistant to each tested antibiotic and carrying ESBL. To evaluate correlates of ESBL-producing Klebsiella spp., we constructed univariate and multivariable Poisson regression models with a robust variance for various child, hospital, and household factors, adjusting for key a priori confounders (age, sex, and site). Associations were considered statistically significant at an alpha < 0.05. All statistical analyses were performed in Stata (Version 17.0, Stata Corp, College Station, TX, USA).




留言 (0)