
記住我






In the United States, more than 1.9 million people are diagnosed with cancer annually.1 Largely due to improved medical management and targeted treatment techniques, there are an estimated 16.9 million survivors of cancer living across the United States.2 With improved survival, the long-term effects of cancer treatment have become evident; chronic health complaints in survivorship may include cardiac impairments, increased body mass index, peripheral neuropathies, and low bone mineral density (BMD).3 As a result of treatment side effects, health-related quality of life is negatively impacted for survivors.4,5 Physical activity improves functional capacity and health-related quality of life for patients during and after cancer treatment6; however, adverse effects associated with antineoplastic agents, including nausea, fatigue, and depression, act as barriers to participation.7 The lack of participation in physical activity results in sarcopenia, furthering the decline of functional capacity and quality of life.8
Whole-body vibration (WBV) is a noninvasive, nonpharmacological modality that can be used to treat impairments caused by cancer treatment without worsening side effects of antineoplastic treatment.9 WBV units consist of flat vibrating platforms that oscillate in various directions at user-defined frequencies and intensities. Closed-chain exercises can be performed in various positions including standing, sitting, and quadruped. Exercise intensity can be adjusted by the therapist to suit the needs of individual patients. Existing studies have demonstrated improved aerobic capacity, pain, muscular strength, BMD, urinary incontinence, balance, and peripheral nerve stimulation.9-18 Mechanical oscillation during WBV results in reactive forces within the body impacting various systems.19 Muscular hypertrophy is thought to be achieved through repetitive contraction and relaxation of fibers and cyclical concentric-eccentric muscle lengthening.19 Acting as an osteogenic stimulus, WBV safely provides benefits for those with lower BMD.20 Animal studies have demonstrated the use of mechanical vibration to be beneficial in the preservation of BMD for mice with ovarian cancer without negatively affecting longevity or promoting tumor progression.21 With the application of low-magnitude, high-frequency stimuli, WBV may safely reduce negative effects of antineoplastic treatment for patients with cancer diagnoses.9-12,14-18,22
Despite promising results in the literature, current utilization and clinician awareness of WBV as a treatment technique for patients with cancer diagnoses are unknown. The aims of this study were to (1) determine the current practices in the use of WBV for cancer rehabilitation across the United States, (2) highlight perceived benefits, indications, and barriers of the use of WBV for patients with cancer, and (3) assess clinician willingness to consider utilization of WBV, particularly for those treating the pediatric population. It is hypothesized that current utilization across the United States will be low, but clinicians will be willing to implement WBV as a treatment method.
METHODSA Web-based survey was created to assess current knowledge, usage, and perceived benefits and barriers of clinicians regarding the use of WBV as a treatment technique. Participants were included if they held a health care license, provide care for patients with cancer diagnoses, and were able to complete the survey in its entirety. Consent was gained prior to completion of the survey. This study was granted exemption following review by the Institutional Review Board at Cincinnati Children’s Hospital Medical Center.
Survey DevelopmentA 28-item survey was developed to observe current practices and clinician perceptions regarding WBV. Visual analog scales (VAS; scaled 0-10) were included to measure current knowledge of, perceived benefits of, and willingness to implement WBV. Knowledge was rated from no knowledge to excellent knowledge, benefits were rated from worsen to improve, and willingness to implement ranged from unwilling to very willing. Appropriateness of various diagnoses and perceived barriers were also assessed (see Survey, Supplemental Digital Content, available at: https://links.lww.com/REHABONC/A57). The survey was assessed for face validity, which was completed by clinicians (occupational therapists and physical therapists [PTs]), administrators, and researchers through a survey feedback form that assessed clarity, response completeness, and navigation. Following assessment of face validity, surveys were distributed to potential respondents in November 2021 and remained accessible for 3 months.
Data CollectionData were collected through the survey built on the Research Electronic Data Capture (REDCap) platform. Recruitment was achieved by sending e-flyers to professional organization’s mailing lists, in addition to social media posts on various professional pages. e-Flyers and social media posts contained a link to the survey.
Data AnalysisAnalysis was performed using R (version 4.1), Microsoft Excel, and SPSS for MacOS (version 28.0; IBM Corp, Armonk, New York). Analysis was completed using frequencies, percentages, mean, and standard deviations (SD) of the data.
RESULTSA total of 98 responses were collected over 3 months, with 72 fully completed survey responses meeting inclusion criteria for analysis.
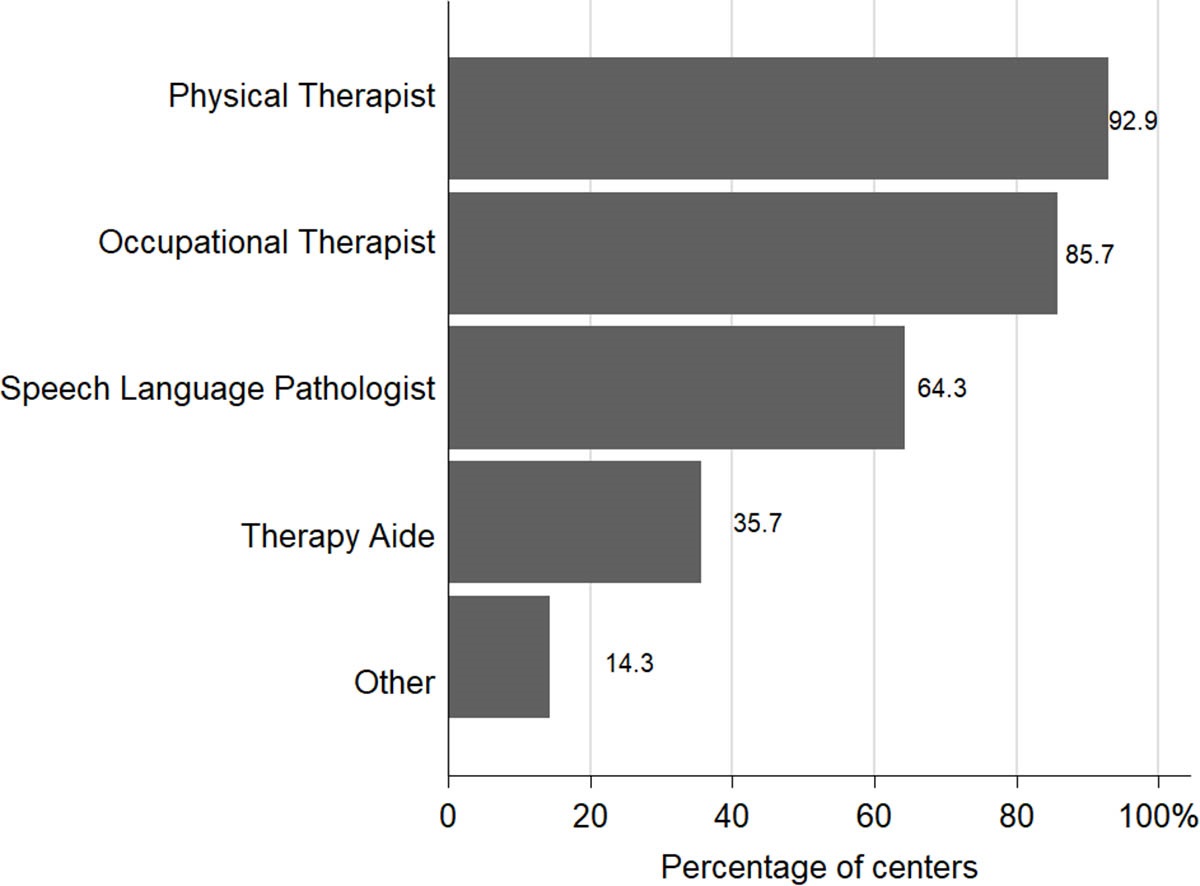
DemographicsRespondent demographics are included in Table 1. Professions included PTs (69.4%), occupational therapists (16.7%), physicians (9.7%), and nurse practitioners (2.8%). Most respondents reported working in inpatient (43.1%) and outpatient (47.2%) practice settings. The majority of clinicians provided care for pediatric populations (41.7%) and had served clinically for 0 to 5 years (27.8%) or 6 to 10 years (25.0%).
TABLE 1 - Survey Respondent Demographics (N = 72) n (%) Profession Physical therapist 50 (69.4) Occupational therapist 12 (16.7) Physician 7 (9.7) Nurse practitioner 2 (2.8) Other 1 (1.4) Practice setting Outpatient 34 (47.2) Inpatient 31 (43.1) Other 7 (9.7) Patient population served Pediatrics 48 (41.7) Adolescents/Young adults 35 (30.5) Adults 32 (27.8) Highest level of education Doctoral degree 39 (54.2) Master’s degree 20 (27.8) MD/DO 7 (9.7) Undergraduate 4 (5.6) PhD 2 (2.8) Years of clinical practice 0-5 y 20 (27.8) 6-10 y 18 (25.0) 20+ y 14 (19.4) 11-15 y 12 (16.7) 16-20 y 8 (11.1)Only 2 (2.78%) respondents were currently using WBV for patients with cancer diagnoses in their clinical practice. The clinicians reported using WBV twice per week. Awareness of WBV as an intervention in patients with cancer diagnoses was low among respondents, with 31% (n = 22) of respondents stating awareness of WBV for patients with cancer diagnoses. Clinicians ranked their level of knowledge of WBV at an average VAS score of 1.89 (SD = 2.36).
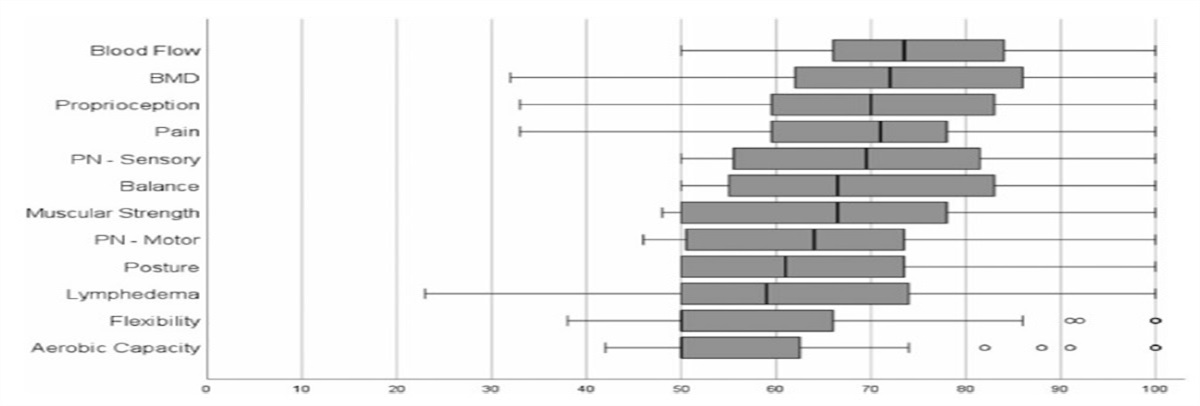
Perceived BenefitsRespondents indicated that WBV could be used safely during both active treatment (outpatient: 76.4%; bone marrow transplantation: 58.4%; inpatient: 48.6%) and survivorship (76.4%). Respondents felt that WBV would be most useful during active outpatient treatment (70.8%).
Perceived system benefits ranked on a 10-point VAS are included in Figure 1. The highest-ranking perceived benefits for WBV included blood flow, BMD, proprioception, pain, and sensory peripheral neuropathy. Respondents rated WBV to be less impactful on aerobic capacity, flexibility, and lymphedema.
 Fig. 1.:
Fig. 1.: Perceived benefits of whole-body vibration on body systems. BMD indicates bone mineral density; PN, peripheral neuropathy.
Perceived BarriersWhen asked to highlight barriers for using WBV for patients with cancer, most respondents reported lack of trained clinicians (81.7%), access to equipment (74.6%), cost of equipment (73.2%), risk of fracture (47.9%), and lack of supportive research (43.7%). Details of all barriers are included in Table 2.
TABLE 2 - Perceived Barriers to WBV Implementation Barrier n (% of Respondents Reporting) Lack of trained clinicians 58 (81.7) Access to equipment 53 (74.6) Cost of equipment 52 (73.2) Risk of fracture 34 (47.9) Lack of supportive research 31 (43.7) Time taken to perform WBV 20 (28.2) Patient perception/Apprehension 20 (28.2) Risk of falls 19 (26.8) Setup time of unit 18 (25.4) Family perception/Apprehension 16 (22.5) Other 5 (7.0) Risk of infection 2 (2.8)Abbreviation: WBV, whole-body vibration.
Responses are included in Figure 2. Respondents selected the most appropriate diagnoses for WBV to be leukemia/lymphoma (63.6%), lymphedema (50.6%), central nervous system cancers (49.4%), and neuroblastoma (46.8%). The 2 diagnoses selected as most inappropriate for WBV were bone tumors (49.4%) and head and neck cancers (24.7%).
 Fig. 2.:
Fig. 2.: Appropriate and inappropriate diagnoses to receive whole-body vibration. CNS indicates central nervous system.
Willingness to Implement WBVClinician willingness to implement WBV on average was ranked at 7.32 (SD = 1.90) on a 10-point VAS.
DISCUSSIONThis is the first study examining clinician knowledge, usage, and perceptions of WBV for patients with cancer diagnoses. Responses suggested low current utilization and awareness of WBV as a treatment technique for patients with cancer diagnoses across disciplines and practice environments. Only 30.6% of clinicians stated that they were aware of WBV, and less than 3% of respondents used WBV for this patient population. Despite low awareness, respondents expressed willingness to use WBV and believed that it was safe to implement across the continuum of cancer care. The results of this study align with literature suggesting that WBV is feasible and safe for patients undergoing active chemotherapy treatment and into survivorship.9-12,14-18,22-24
Perceived appropriateness of WBV varied depending upon diagnosis. Patients with hematological cancers were perceived as the most appropriate candidates to receive WBV. This aligns with existing literature suggesting WBV for patients with hematological cancer diagnoses is feasible, safe, and potentially improves functional ability.9,15 The most commonly studied diagnosis in existing literature, breast cancer,18,22,23 was ranked the sixth most appropriate diagnosis in this survey’s results, falling behind other diagnoses, such as central nervous system cancers and neuroblastoma, which have not been previously studied. Less than 40% of respondents felt that WBV was appropriate for prostate and lung cancers diagnoses, contradicting literature that suggests WBV is in fact safe and feasible for both diagnoses.12,14,17 Bone cancers were the most reported inappropriate diagnosis for treatment with WBV, likely as a result of the increased risk of fracture caused by disruption to bone integrity.25 Patients with bone cancer were also commonly excluded from previous studies,9,16,23 suggesting good agreement between survey and existing literature.
In pediatric populations, such as cerebral palsy, WBV has been demonstrated to be a noninvasive method of providing improved bone health, muscular strength, balance, gait, and motor skills while decreasing spasticity.26-31 Similar benefits have been demonstrated for those with cancer diagnoses; however, results are contradictory between studies. This adds to the confusion as to the true effect of WBV on body systems. Alignment with previous literature is demonstrated, with respondents suggesting BMD, proprioception, and pain are among the systems most likely to benefit from WBV. Surprisingly, respondents identified improved blood flow as the greatest benefit of WBV. To the authors’ knowledge, this has not been empirically studied in patients with cancer diagnoses; however, WBV has been shown to increase blood flow in patients with diabetes and spinal cord injuries.32,33 The effect of increased blood flow in patients receiving intravenous chemotherapy is not known, though animal studies conclude that neither disease progression nor worsening of prognosis occurred using WBV.21 Interestingly, respondents indicated they were less certain about positive effects on aerobic capacity. The average survey response for aerobic capacity was neutral (5/10 on the VAS). In contrast, WBV has been stated to be a practical intervention to improve aerobic capacity post–cancer treatment.13
WBV is used as an adjunct to standard intervention in existing literature and does not appear to substitute for conventional resistive equipment.14 WBV may complement existing therapy interventions, though resistance activities may need to be adapted to allow performance using the vibrating platform. Nearly all studies examining WBV in patients with cancer have examined the effect of WBV with participants performing body weight resisted exercise while standing on the WBV platform, with results varying between studies.9,14,16-18,22 Only one study examined the effects of WBV on participants who stood without actively exercising while on the WBV platform; no significant improvements between the control and intervention groups were demonstrated.23 Further study is needed to examine the parameters and exercise format using WBV that may provide optimal improvements for patients with cancer diagnoses.
The greatest potential that WBV offers for patients with cancer diagnoses is in the prevention of osteopenia, sarcopenia, and other side effects of antineoplastic treatment. Careful investigation for the most appropriate time to implement WBV for optimal effect is key to understanding and harnessing potential positive effects. More than 70% of survey respondents selected active treatment on an outpatient basis and into survivorship as the most useful and safe time to implement WBV. Respondents were less certain that patients receiving active treatment while inpatient would be a useful and safe time for WBV. This is possibly due to the increased acuity of patients admitted for treatment and fear of interference of WBV on the effect of chemotherapy. Although both exercise and WBV have been demonstrated to be plausible interventions during inpatient intensive chemotherapy without side effects or adverse events,9,34 other studies continue to exclude patients concurrently receiving chemotherapy.18
Barriers to using WBV identified by respondents must be overcome to improve clinical application. Risk of fracture was reported as a barrier to using WBV despite no such events being reported in existing literature. Risk of fracture when using WBV, as with exercise, should remain a consideration for clinicians when choosing appropriate patients. Previously reported adverse events include syncope and increased upper extremity edema.23 To overcome barriers of cost and access to equipment, future research must include high-quality, adequately powered randomized controlled trials to provide clear justification of cost and value added to patient outcomes using WBV.
Limitations of this study include the recruitment methods, small sample size, and a survey with only face validity that limits larger generalization of results. The high proportion of PTs responding to the survey may limit generalizations to other clinicians; however, it is likely that PTs will be most likely to use this modality. It is possible that clinicians with an interest or underlying knowledge of this survey topic were more motivated to provide responses, thus overinflating the current level of knowledge of WBV. A further limitation of this study was our convenience sampling of clinicians in pediatric institutions. Future knowledge and research are needed to understand clinical use of WBV with children and adolescents compared with the adult population.
CONCLUSIONSAwareness of WBV as a treatment intervention for cancer diagnoses is low among health care professionals. Most clinicians would be willing to use WBV and feel it is safe to use as part of a cancer rehabilitation program throughout the oncology continuum of care. More research is needed to determine the appropriate timing and dosage of this intervention. The greatest perceived benefits reported by respondents target frequently affected systems following antineoplastic treatment, offering hope for symptom relief for patients. Mitigation of barriers to enable clinical application of WBV, continued collaboration on the management of side effects related to antineoplastic treatment, and future studies in the use of WBV for cancer diagnoses are warranted.
STUDY DETAILS Author Contributions Role Author Conceptualization BR, JBer, KM, MS, KG Data curation BR Formal analysis JBen Funding acquisition Investigation BR Methodology BR, JBer, KM, KG Project administration BR Resources Software JBen Supervision MS KG Validation Visualization JBen Writing – original draft BR, JBer, JBen, KG Writing – review & editing BR, JBer, KM, MS, JBen, KGIntradepartmental funds from the Division of Clinical Therapies at Nationwide Children’s Hospital funded biostatistician support.
Ethics ApprovalConsent was gained prior to completion of the survey. This study was granted exemption following review by the Institutional Review Board at Cincinnati Children’s Hospital Medical Center.
Data Sharing StatementThe data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
ACKNOWLEDGMENTSThe authors are grateful to Ms Sula Bernstein for her valuable input and suggestions. The authors are also grateful to Mss McKenzie Stevens, Alisha Pratt, Jessica Lloyd, and Kelli Hobart for their role in the development of the survey.
REFERENCES 1. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin. 2022;72(1):7-33. 2. Miller KD, Nogueira L, Mariotto AB, et al. Cancer treatment and survivorship statistics, 2019. CA Cancer J Clin. 2019;69(5):363-385. 3. Mulrooney DA, Hyun G, Ness KK, et al. The changing burden of long-term health outcomes in survivors of childhood acute lymphoblastic leukaemia: a retrospective analysis of the St Jude Lifetime Cohort Study. Lancet Haematol. 2019;6(6):e306-e316. 4. Mokhatri-Hesari P, Montazeri A. Health-related quality of life in breast cancer patients: review of reviews from 2008 to 2018. Health Qual Life Outcomes. 2020;18(1):338. 5. Vetsch J, Wakefield C, Robertson E, et al. Health-related quality of life of survivors of childhood acute lymphoblastic leukemia: a systematic review. Qual Life Res. 2018;27(6):1431-1443. 6. Muller C, Krauth KA, Gerss J, Rosenbaum D. Physical activity and health-related quality of life in pediatric cancer patients following a 4-week inpatient rehabilitation program. Support Care Cancer. 2016;24(9):3793-3802. 7. Frikkel J, Gotte M, Beckmann M, et al. Fatigue, barriers to physical activity and predictors for motivation to exercise in advanced cancer patients. BMC Palliat Care. 2020;19(1):43. 8. Kakinuma K, Tsuruoka H, Morikawa K, et al. Differences in skeletal muscle loss caused by cytotoxic chemotherapy and molecular targeted therapy in patients with advanced non-small cell lung cancer. Thorac Cancer. 2018;9(1):99-104. 9. Pahl A, Wehrle A, Kneis S, Gollhofer A, Bertz H. Feasibility of whole body vibration during intensive chemotherapy in patients with hematological malignancies—a randomized controlled pilot study. BMC Cancer. 2018;18(1):920. 10. Mogil RJ, Kaste SC, Ferry RJ Jr, et al. Effect of low-magnitude, high-frequency mechanical stimulation on BMD among young childhood cancer survivors: a randomized clinical trial. JAMA Oncol. 2016;2(7):908-914. 11. Rustler V, Prokop A, Baumann FT, Streckmann F, Bloch W, Daeggelmann J. Whole-body vibration training designed to improve functional impairments after pediatric inpatient anticancer therapy: a pilot study. Pediatr Phys Ther. 2018;30(4):341-349. 12. Crevenna R, Cenik F, Margreiter M, Marhold M, Sedghi Komanadj T, Keilani M. Whole body vibration therapy on a treatment bed as additional means to treat postprostatectomy urinary incontinence. Wien Med Wochenschr. 2017;167(5/6):139-141. 13. Lopes-Souza P, Dionello CF, Sa-Caputo DDC, et al. Whole body vibration exercise in the management of cancer therapy-related morbidities: a systematic review. Drug Discov Ther. 2018;12(4):239-247. 14. Salhi B, Haenebalcke C, Perez-Bogerd S, et al. Rehabilitation in patients with radically treated respiratory cancer: a randomised controlled trial comparing two training modalities. Lung Cancer. 2015;89(2):167-174. 15. Schonsteiner SS, Bauder Missbach H, Benner A, et al. A randomized exploratory phase 2 study in patients with chemotherapy-related peripheral neuropathy evaluating whole-body vibration training as adjunct to an integrated program including massage, passive mobilization and physical exercises. Exp Hematol Oncol. 2017;6:5. 16. Streckmann F, Lehmann HC, Balke M, et al. Sensorimotor training and whole-body vibration training have the potential to reduce motor and sensory symptoms of chemotherapy-induced peripheral neuropathy-a randomized controlled pilot trial. Support Care Cancer. 2019;27(7):2471-2478. 17. Tantawy SA, Elgohary HMI, Abdelbasset WK, Kamel DM. Effect of 4 weeks of whole-body vibration training in treating stress urinary incontinence after prostate cancer surgery: a randomised controlled trial. Physiotherapy. 2019;105(3):338-345. 18. de Sire A, Lippi L, Ammendolia A, et al. Physical exercise with or without whole-body vibration in breast cancer patients suffering from aromatase inhibitor-induced musculoskeletal symptoms: a pilot randomized clinical study. J Pers Med. 2021;11(12):1369. 19. Rittweger J. Vibration as an exercise modality: how it may work, and what its potential might be. Eur J Appl Physiol. 2010;108(5):877-904. 20. Rubin CT, Sommerfeldt DW, Judex S, Qin Y. Inhibition of osteopenia by low magnitude, high-frequency mechanical stimuli. Drug Discov Today. 2001;6(16):848-858. 21. Pagnotti GM, Adler BJ, Green DE, et al. Low magnitude mechanical signals mitigate osteopenia without compromising longevity in an aged murine model of spontaneous granulosa cell ovarian cancer. Bone. 2012;51(3):570-577. 22. Van Ruymbeke B, Boone J, Coorevits P, Vanderstraeten G, Bourgois J. Whole-body vibration in breast cancer survivors: a pilot study exploring its effects on muscle activity and subjectively perceived exertion. Int J Rehabil Res. 2014;37(4):371-374. 23. Baker MK, Peddle-McIntyre CJ, Galvao DA, Hunt C, Spry N, Newton RU. Whole body vibration exposure on markers of bone turnover, body composition, and physical functioning in breast cancer patients receiving aromatase inhibitor therapy: a randomized controlled trial. Integr Cancer Ther. 2018;17(3):968-978. 24. Verhulst AL, Savelberg HH, Vreugdenhil G, Mischi M, Schep G. Whole-body vibration as a modality for the rehabilitation of peripheral neuropathies: implications for cancer survivors suffering from chemotherapy-induced peripheral neuropathy. Oncol Rev. 2015;9(1):263. 25. Fornetti J, Welm AL, Stewart SA. Understanding the bone in cancer metastasis. J Bone Miner Res. 2018;33(12):2099-2113. 26. Rustler V, Daggelmann J, Streckmann F, Bloch W, Baumann FT. Whole-body vibration in children with disabilities demonstrates therapeutic potentials for pediatric cancer populations: a systematic review. Support Care Cancer. 2019;27(2):395-406. 27. Duquette SA, Guiliano AM, Starmer DJ. Whole body vibration and cerebral palsy: a systematic review. J Can Chiropr Assoc. 2015;59(3):245-252. 28. Cai X, Qian G, Cai S, Wang F, Da Y, Ossowski Z. The effect of whole-body vibration on lower extremity function in children with cerebral palsy: a meta-analysis. PLoS One. 2023;18(3):e0282604. 29. Krause A, Schonau E, Gollhofer A, et al. Alleviation of motor impairments in patients with cerebral palsy: acute effects of whole-body vibration on stretch reflex response, voluntary muscle activation and mobility. Front Neurol. 2017;8:416. 30. Liquori BM, Gannotti ME, Thorpe DE, Fuchs RK. Characteristics of interventions to improve bone health in children with cerebral palsy: a systematic review. Pediatr Phys Ther. 2022;34(2):163-170. 31. Tekin F, Kavlak E. Short- and long-term effects of whole-body vibration on spasticity and motor performance in children with hemiparetic cerebral palsy. Percept Mot Skills. 2021;128(3):1107-1129. 32. Herrero AJ, Menendez H, Gil L, et al. Effects of whole-body vibration on blood flow and neuromuscular activity in spinal cord injury. Spinal Cord. 2011;49(4):554-559. 33. Sanudo B, Alfonso-Rosa R, Del Pozo-Cruz B, Del Pozo-Cruz J, Galiano D, Figueroa A. Whole body vibration training improves leg blood flow and adiposity in patients with type 2 diabetes mellitus. Eur J Appl Physiol. 2013;113(9):2245-2252. 34. Rustler V, Hagerty M, Daeggelmann J, Marjerrison S, Bloch W, Baumann FT. Exercise interventions for patients with pediatric cancer during inpatient acute care: a systematic review of literature. Pediatr Blood Cancer. 2017;64(11). doi:10.1002/pbc.26567.
留言 (0)