RA patients are known to have a 2- to 4-fold higher incidence of malignant lymphoma as a complication than the general population [4]. Although MTX is used as a first-line treatment for patients with RA, it carries a risk of LPD [2]. When LPD occurs, biologics are often used in the RA patients as an alternative to MTX [5]. LPD, including malignant lymphoma, has been found to occur in RA patients receiving MTX, and this is termed MTX-LPD. The WHO classifies it as immunodeficiency-associated LPD. EBV infection is said to be a complication in about half of MTX-LPD cases, and EBV reactivation has been implicated [6,7,8]. It is thought that the EBV gene releases factors similar to growth factors, transcription factors, and apoptosis inhibitors, causing B lymphocytes to transform into lymphoblasts, exhibiting tumor-like growth [9]. The most common sites of MTX-LPD are lymph nodes [10] and tonsils [11], but thyroid [12], lung [13], liver [14], and colon lesions [15] have also been reported.
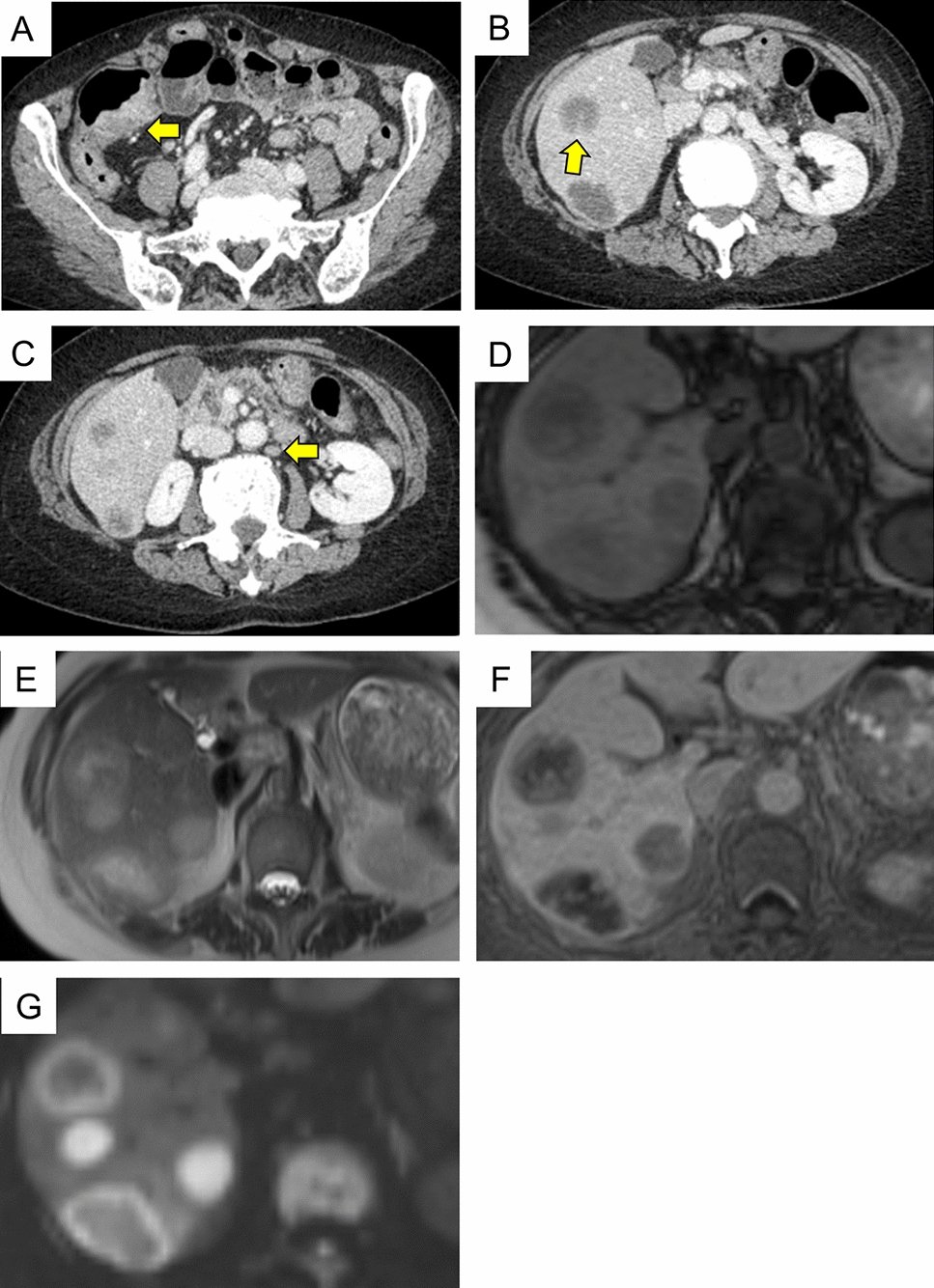
Imaging modalities, such as US and CT, can aid the diagnosis of hepatic lymphoma/MTX-LPD. A previous report has indicated that penetrating vessels running through the tumor visualized by US was helpful for diagnosis of hepatic lymphoma [16]. In the present case, penetrating vessels running through the tumor were detected by CT scan. The evidence suggests that MTX-LPD should be considered in RA patients who are receiving MTX medications when CT or US shows a hepatic mass with signs of penetrating vessels.
A search of PubMed using the terms “MTX-LPD” and “hepatic”, or “MTX-LPD” and “liver”, yielded 12 available studies published in English between 2000 and 2022 [10, 14, 17,18,19,20,21,22,23,24,25,26]. In all cases the patients had been treated with immunosuppressants such as MTX, steroids, infliximab, and tacrolimus. All had taken MTX for more than 24 months, and the median total dose of MTX was 1932 mg (960–6000 mg). Ten patients showed reactivation of EBV. The present patient had taken MTX for 24 months (total dose, 960 mg) and also showed reactivation of EBV. MTX-LPD involving the liver along with other parenchymal organs must be differentiated from cancer metastasis. As shown in Table 2, five patients with hepatic MTX-LPD accompanied by other parenchymal organ lesions involvement of the adrenal gland (n = 2), multiple lymph nodes (n = 1), spleen (n = 1), and colon (n = 1, this case).
Table 2 Reported cases of rheumatoid arthritis patients with methotrexate-related lymphoproliferative disease in the liverIn the listed MTX-LPD, DLBCL type cases (n = 8), MTX was discontinued and three of the patients achieved complete remission. Three additional patients achieved complete remission with chemotherapy. Two patients were treated by partial hepatectomy and had no recurrence. Two patients with MTX-LPD, Hodgkin lymphoma type, also stopped using MTX. One of them suffered relapse even after withdrawal of MTX, and the other underwent partial hepatectomy and had no recurrence. Our present patient achieved complete remission after MTX had been withdrawn. These findings suggest that immediate withdrawal of MTX is recommended for patients with hepatic MTX-LPD, DLBCL type. Our patient had two lesions; these may have been concurrent, or one may have been due to metastasis from the colon to the liver. Because of the multiple lymph node metastases and the histological similarities of the lesions, the possibility that the colon lesion had metastasized to the liver could not be ruled out. To our knowledge, this is the first case of MTX-LPD involving both the liver and colon to have been reported in English.



留言 (0)