Design and Participants
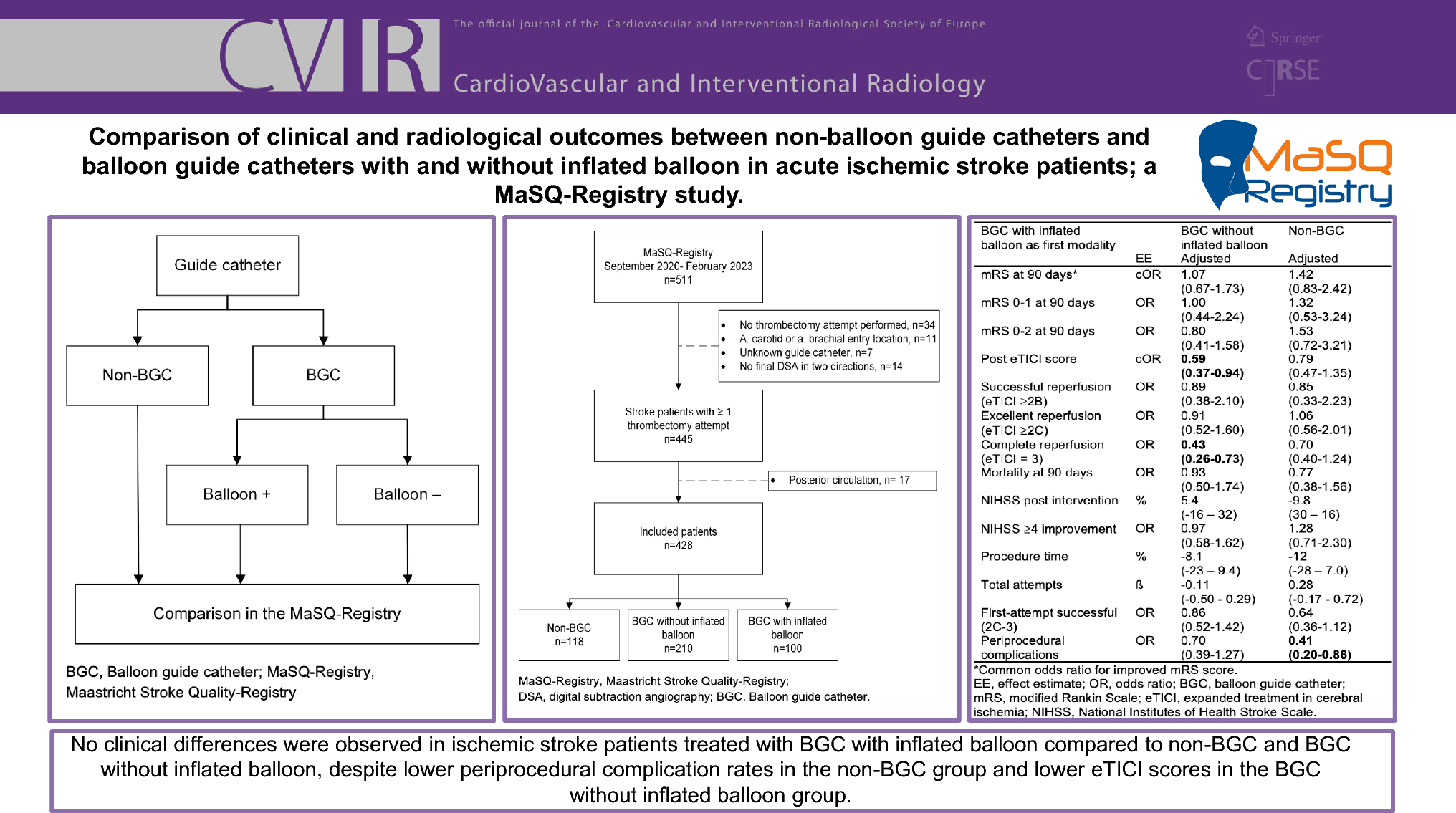
For this study, we used data from the Maastricht Stroke Quality-Registry (MaSQ-Registry) from September 2020 to February 2023. In the MaSQ-Registry, data were prospectively collected for quality purposes by the treating physicians and researchers. Patients were included if they met the following inclusion criteria: age ≥ 18 years, an intracranial anterior circulation occlusion (thrombus or dissection) confirmed by CT-angiography, and groin puncture within 24 h after symptom onset. Patients were excluded when no data were available regarding the guide catheter and the balloon, or when no final digital subtracted angiography was performed in two different projections. Patients were divided into three groups based on the first-line thrombectomy technique: non-BGC, BGC with inflated balloon, and BGC without inflated balloon.
Ethical approval for retrospective analysis was obtained from the medical ethics committee. The need to obtain individual informed consent was waived, according to the Dutch Medical Research Involving Human Subjects Act. Data were collected in a secured online Castor (v2023.1.2.0) database. This study was conducted using the STROBE guidelines.
Outcome Measures
The primary outcome was the modified Rankin Scale 90 days after EVT. The mRS runs from 0 (no symptoms) to 6 (death) [14]. Secondary clinical outcomes included excellent and favorable functional outcome (defined as mRS 0–1 and mRS 0–2, respectively), the National Institutes of Health Stroke Scale (NIHSS) 24–48 h after the EVT, and early neurological recovery, defined as improvement of 4 or more points on the NIHSS at 24–48 h after EVT. Deceased patients were assigned a score of “42” [15]. The NIHSS was scored as standard care by the attending physician at the ward or retrospectively using a standardized score chart based on the reports of the neurological exam.
Technical outcomes were reperfusion rate, procedure duration, first-attempt successful reperfusion, and the occurrence of periprocedural complications. The expanded Thrombolysis In Cerebral Infarction (eTICI) scale was used to assess the reperfusion after EVT. eTICI is a scale from 0 (no perfusion) to 3 (100% reperfusion) [16]. Successful, excellent, and complete reperfusion was defined as eTICI ≥ 2B, ≥ 2C, and 3, respectively. The eTICI was scored by the treating physician at the end of the procedure.
Imaging Assessment
The Alberta Stroke Program Early CT Score (ASPECTS) and the collateral status according to Tan et al. on baseline CT scans were assessed in a core laboratory by one neuroradiologist and one neuro-interventional radiologist [17]. Both core laboratory members were blinded for clinical outcome. After every thrombectomy attempt and at the end of the thrombectomy, the eTICI score was scored by the treating physician, who performed the thrombectomy. The final eTICI score was used as outcome measure and, when necessary, reevaluated by a second neuro-interventional radiologist.
Treatment
Local and national guidelines for the treatment of AIS were followed. The choice of technique and devices during EVT was left to the treating physician. The EVT characteristics regarding the first-line technique, including the use of a (non-)BGC and whether the balloon was inflated or not, were registered by the treating physician directly after the procedure. There was no default guide catheter and no predefined criteria whether the balloon of a BGC should be inflated or not. These decisions were made by the treating physician based on personal preferences and periprocedural findings (e.g., when achieving flow arrest without inflating the balloon, when the BGC was not placeable in the internal carotid artery, in case of a carotid dissection). The reasons not to inflate the balloon were not registered. The first-line technique was registered as direct aspiration only, stent retriever thrombectomy only, or combined technique thrombectomy (stent retriever combined with an aspiration catheter). Regardless the used first-line technique, aspiration at the back end of the guide catheter was achieved using manual aspiration with a 50 cc syringe. Periprocedural complications included distal thrombi, vasospasm, perforations, and dissections and were scored by the treating physician directly after the EVT.
Statistical Analysis
Baseline characteristics were analyzed with descriptive statistics. To analyze continuous variables, we used an ANOVA or Kruskal–Wallis test. For binary and ordinal data, the Chi-square test or Fisher’s exact test was used. Multivariable ordinal regression analysis was used to compare the differences in the mRS at 90 days with BGC with inflated balloon as comparator. Multivariable linear, ordinal, or binary logistic regression analyses were performed for our secondary outcomes as appropriate. Continuous outcome measures were transformed using the natural logarithm because the residuals were not normally distributed. Effect estimates from the resulting regression models were exponentiated to calculate the percentual change using the following formula: (exponentiate (β-coefficient) − 1) × 100%.
The adjustments used in the regression analyses were based on literature and univariable analyses. Variables used in the regression analyses for adjustments were age, atrial fibrillation, pre-NIHSS, pre-mRS (dichotomized 0 versus 1–5), systolic blood pressure, presence of a tandem lesion, time between symptom onset and groin puncture, baseline ASPECTS, and baseline collateral score. All analyses were performed using R (version 4.1.2). P values below 0.05 were considered statistically significant.
Missing Values
Baseline characteristics were described using raw data. For the regression analyses, missing data were imputed with multiple imputation by chained equations (MICE) using the mice package version 3.14.0 with predefined variables as predictors. The number of imputations was set to 50. Table 1 shows the missing rate in baseline variables. The mRS-score was missing in 6.8%. When one of the subitems of the NIHSS or the total NIHSS score was missing (in 8.9% of the cases), the NIHSS sum score was imputed.
Table 1 The baseline characteristics of the included patientsSubgroup Analyses
To investigate the effect of the first-line technique on the mRS score, subgroup analyses were performed. We distinguished direct aspiration only thrombectomy, stent retriever only thrombectomy, and the combined technique thrombectomy as first-line thrombectomy techniques. In the subgroup analyses, the same adjustments were made as in the main analyses. Additionally, a sensitivity analysis was performed to investigate the effect of the different guide catheters after removing the patients with a carotid artery stenosis or a carotid stent placement during EVT. The analysis was repeated on the mRS at 90 days, mRS 0–1, and mRS 0–2.





留言 (0)