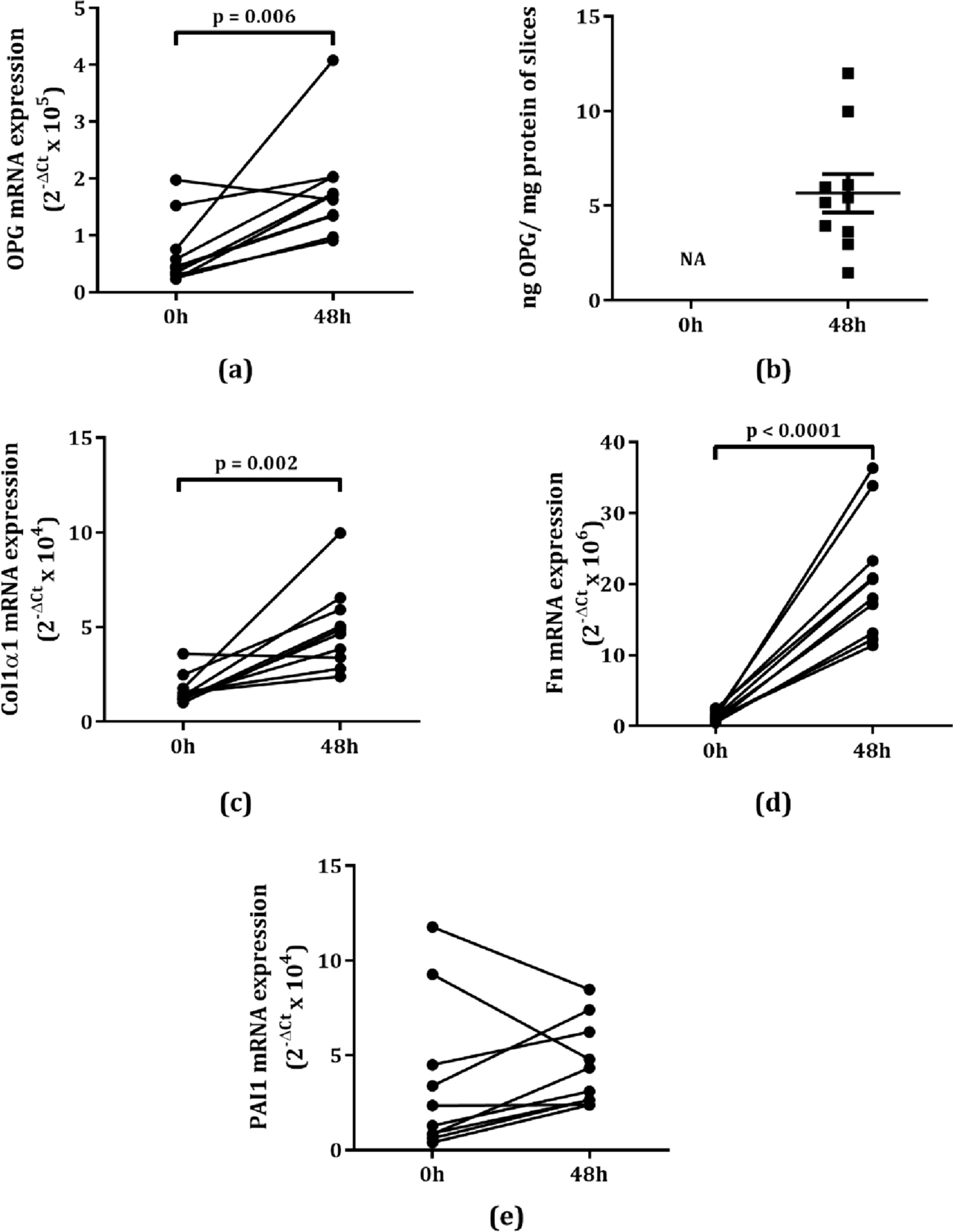
Our study investigated if OPG expression would associate with fibrotic responses induced by profibrotic cytokines TGFβ1 or IL13 in lung tissue and whether it would respond to antifibrotic treatment. OPG was initially recognized for its role in bone turnover in which it prevents bone resorption and stimulates production of extracellular matrix in cartilage [18]. However, in recent years, an increasing number of studies have shown correlations between OPG and several fibrotic conditions including liver, vascular, cardiac, kidney and intestinal fibrosis [19,20,21,22,23,24,25,26,27,28,29]. This study, and our own previous studies [9, 10] have now shown that this also appears to be the case for fibrosis in lung tissue and even wound healing. Our data shows that after the slicing procedure a repair or regenerative response was induced, with higher Col1α1 and Fn mRNA expression, which was accompanied by higher production of OPG. Inducing a more fibrotic response by treating with TGFβ1 magnified this inherent repair response induced by slicing.
How OPG actually influences wound repair and fibrosis is still an open question, but a study by Hao et al. suggests an interaction between TRAIL, OPG, and collagen-producing cells [30]. Using OPG-deficient mice, they showed lower collagen deposition in heart tissue, accompanied by increased expression of TRAIL and a higher level of apoptosis in heart tissue, which suggesting an association between TRAIL, OPG, and collagen production. We have previously shown fibroblasts and myofibroblasts to be important producers of OPG [9, 14] and these cells are also key cells in collagen production [31, 32]. These combined findings indicate that OPG, as a decoy receptor for TRAIL, may protect (myo)fibroblasts from TRAIL-induced apoptosis and can thereby contribute to both physiological wound healing and fibrosis. Alternatively, OPG, serving as a decoy receptor for RANKL, might also play a role in hindering RANKL-induced epithelial repair, as previously demonstrated by us [10]. Coupled with the suppression of TRAIL-induced apoptosis of myofibroblasts, this mechanism could potentially contribute to the development of fibrosis. Future studies should be designed to investigate these interactions in more detail in the context of lung fibrosis.
Interestingly, there appears to be no close connection between OPG and collagen production as OPG mRNA expression did not correlate with Col1α1 mRNA expression, while OPG did correlate with Fn and PAI1 in our model of early-stage fibrosis. Little is known about interactions between Fn, PAI1 and OPG, however, a study by Vial et al. showed that PAI1 stimulates Fn matrix assembly by disrupting the interaction between αvβ5 and vitronectin that then stimulates activation of α5β1 integrin, which increases the rate of Fn polymerization [33]. OPG has been shown to bind to αv integrins as well and may therefore enhance production of other fibrotic markers [34].
As we have shown before, OPG expression in lung tissue can clearly be promoted by TGFβ1, [24, 29, 35, 36]. To get more insight into the regulation of OPG expression, we also studied the effect of IL13, a fibrosis-associated cytokine known to be able to increase TGFβ1 expression [14, 37]. Indeed, previous studies have shown that IL13 plays an important role in the development of lung fibrosis [38, 39]. However, unlike TGFβ1, IL13 stimulation of murine lung slices did not induce mRNA expression of Col1α1, Fn and PAI1, while it did induce production of OPG mRNA and protein. This induction appeared to be directly dependent on TGFβ1 as co-treatment with galunisertib, a TGFβ receptor-I kinase inhibitor, could completely block the OPG-inducing effect of IL13. We previously showed a similar phenomenon in liver slices, in which IL13 induced OPG expression through IL13 receptor α2 (IL13Rα2)-induced TGFβ production [14]. In the present study we did find higher expression of IL13Rα2 after treatment with IL13, but not a concomitant increase in TGFβ1 expression. This may have been caused by a difference in the kinetics of different mRNA transcripts studied. However, these results do suggest that OPG is responsive towards small changes in fibrogenesis and may thus serve as sensitive marker to observe fibrosis initiation and/or progression. Indeed, a recent multicenter cohort study by Bowman et al. showed that OPG particularly associated with progressive fibrosing interstitial lung disease, reinforcing this view [11].
Importantly, we found that OPG was also released by both slices from lung tissue of a patient with normal lung function as well as slices from lung tissue of patients with lung fibrosis, with the latter releasing far more than slices of control lung tissue. The OPG production by control lung tissue could also be increased by stimulating with TGFβ1, suggesting similar pathways in mice and men. Due to limited availability of lung tissue from patients with normal lung function, we only obtained one sample for this study and these studies should therefore be extended for definite conclusions. Our results, however, do confirm the possibility of studying OPG as a marker of lung fibrosis in a clinical setting. The advantage of using OPG as marker of remodeling and fibrosis over other tissue proteins is that OPG is a soluble protein that can easily be measured in blood or culture media. Serum OPG should therefore be further investigated as a marker for progression of fibrotic disease in clinical practice.
In the interest of clinical applicability of OPG as a marker for treatment effects, we further investigated whether OPG production is affected by treatment with antifibrotic drugs. We found that OPG production was indeed inhibited by both drugs, even though expression of fibrosis-associated markers were not (yet) affected. The reason for this discrepancy is unclear but as many in vitro, in vivo, and clinical studies have shown pirfenidone and nintendanib can inhibit extracellular matrix production [40,41,42,43,44,45,46,47,48], our results reinforce the notion that OPG may be an early marker of treatment effect before any other markers are affected.
Concluding, our study has shown that OPG is upregulated in early stages of lung fibrosis and wound repair and responds to antifibrotic treatment. As OPG can easily be measured in serum, it is an interesting candidate to further investigate as a potential biomarker for fibrotic disorders of the lung and a potential marker for treatment effect of novel antifibrotics.




留言 (0)