Phosphodiesterase (PDE)-4 is an enzyme responsible for the activity of various inflammatory cytokines. The increased levels of PDE-4 are found in patients with atopic dermatitis (AD), a skin inflammatory disorder involving skin barrier dysfunction responsible for erythema, pruritis, and dry patches on the skin, affecting the patient's quality of life [[1], [2], [3]]. PDE-4 increases the levels of inflammatory mediators involved in the pathogenesis of AD, including interleukin (IL)-4, IL-12, IL-5. The increased levels of PDE-4 lead to a decrease in levels of intracellular cAMP, which is responsible for the activation of various transcription factors, thereby leading to the elevation of various inflammatory mediators [4]. The drug molecules inhibiting PDE-4 activity cause an increase in the intracellular cAMP levels, thereby reducing the inflammatory cytokine levels involved in the pathogenesis of AD [5,6].
Apremilast (AP) is one such small drug molecule, an inhibitor of PDE-4 approved for treating psoriasis and psoriatic arthritis with an oral dose of 30 mg [7]. The clinical trial (phase 2, double-blind, NCT02087943) associated with oral administration of AP in doses of 30 and 40 mg daily in patients with moderate to severe AD showed a dose-dependent reduction in AD signs. The administration of 40 mg has significantly reduced the eczema area and severity index (EASI) but resulted in more adverse effects, including cellulitis in comparison with 30 mg dose. The frequent observation of cellulitis in patients receiving 40 mg AP resulted in discontinuation of this dose [8].
The oral delivery of AP is associated with several adverse effects with the dose of 30 mg daily in patients, such as nausea, diarrhoea, hypersensitivity and upper respiratory tract infection due to the off-target effects [9]. Another disadvantage of oral delivery of AP is its poor bioavailability due to the associated poor solubility and permeability, where it is classified as a biopharmaceutical classification system (BCS) class-IV drug [10,11]. To avoid the obstacles related to the oral delivery of AP, a topical route could be a better alternative to the oral route. The stratum corneum (SC) is the outermost layer of skin representing permeation barrier for the topically applied formulations. Various strategies of drug delivery systems have been developed to overcome this barrier such as lipid based nanocarriers including liposomes, ethosomes, transfersomes, solid lipid nanoparticles, nanostructured lipid carriers, nanoemulsions, liquid crystalline nanoparticles (LCN) and polymer based nanocarriers such as polymeric nanoparticles, polymeric micelles etc [12,13].
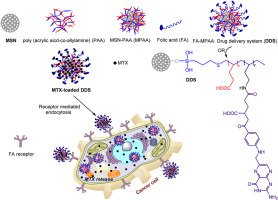
Out of these nanocarrier systems, LCNs possess various advantages for the delivery of drugs through the topical route. LCNs are lipid-based nanocarriers formed from the lamellar, cubic and hexagonal phases of commonly used amphiphilic lipids such as glyceryl monooleate/monoolein (MO) or phytantriol. In contrast, the surface of these nanocarriers is stabilized by incorporating polymers and surfactants [[14], [15], [16]]. The similar structural organization of LCN with SC and their high affinity towards skin would help to overcome the SC barrier and improve the permeability of drugs through the topical route. The amphiphilic nature of lipids forming LCN and the presence of surfactants further favour the skin permeability of drugs. The topical application of the drug-loaded in LCN interacts with the skin, forms a depot in stratum corneum layers and releases the drug in a controlled manner. This will further improve drug retention in skin layers and avoid systemic absorption, leading to minimal systemic adverse effects. Apart from this, the presence of water molecules in the structure of LCN provides hydration to the skin tissues [11,[17], [18], [19], [20]]. Various researchers have explored the topical delivery of not only drugs but also small interfering RNAs (siRNA) by encapsulating into the LCN system to improve the skin permeability as well as retention for the management of various skin disorders e.g. finasteride for androgenic alopecia [21]; tacrolimus for psoriasis [22]; apremilast for psoriasis [23]; luliconazole for fungal infection [24]; rapamycin for psoriasis [25]; apigenin for skin cancer [26]; co-delivery of triptolide and siRNA for psoriasis [27]; trans-resveratrol for skin inflammation [28]; protoporphyrin IX for photodynamic therapy [29]; oleanolic acid for inflammation [30].
In this regard, to improve the penetration and retention in skin layers, avoid the adverse effects associated with off-target activity, and increase drug loading, we have encapsulated the AP in LCN to improve its efficacy in AD management. In the current study, we have used MO as a lipid phase, poloxamer 407 and tween 20 as surfactants to prepare AP-LCN. Further, for the formulation of AP-LCN based gel (AP-LCNG), SEPINEO™ P 600 gel base was used. In vivo efficacy studies of AP-LCNG were evaluated in AD mice model.









留言 (0)