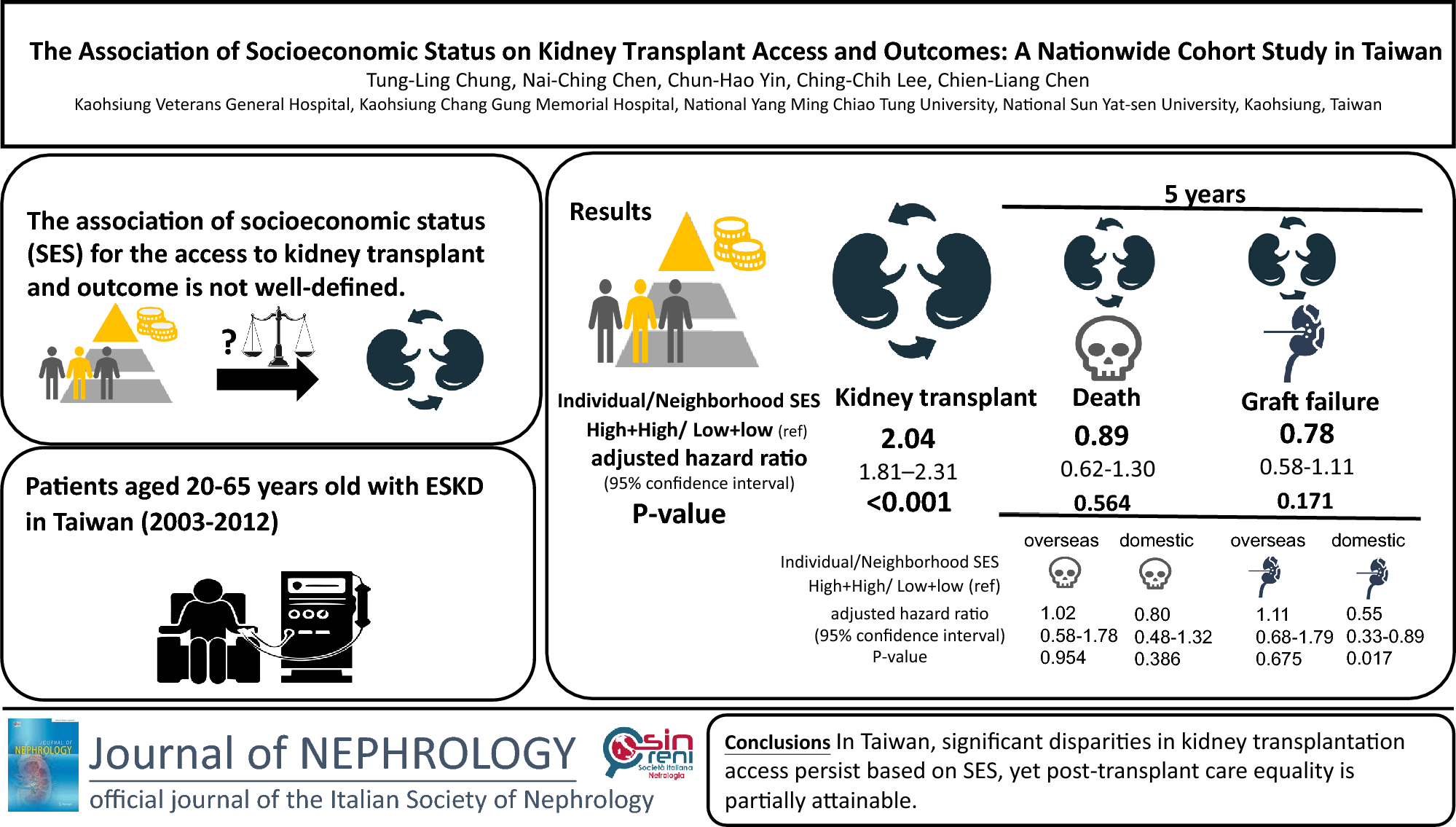
This population-based study in Taiwan assessed the combined effects of individual and neighborhood socioeconomic status on access to kidney transplantation in patients with ESKD. We investigated post-transplant patient readmission rates and graft survival using data provided by the NHI system. Data show that only 3004 patients (2.7% of ESKD patients) underwent kidney transplantation between 2003 and 2012 (10 years). Furthermore, patients with lower individual and neighborhood socioeconomic status had a lower chance of kidney transplantation despite Taiwan’s universal care and donor care system. We divided the transplant population into two groups, those who received a kidney transplant overseas and in Taiwan; the disparity in access to kidney transplants remained, and was associated with patients’ socioeconomic status and place of residence. However, these inequalities, including mortality and graft failure, were less relevant after transplantation. In the subgroup analysis, disparities existed only within domestic kidney transplant graft survival rates.
Concerning overseas kidney transplants, patients with low socioeconomic status cannot afford the fees for travel, surgery, and immunosuppressive drugs. Thus, it is reasonable to assume that disparities exist between overseas kidney transplant recipients and domestic ones. Previous studies have shown an association between individual or area socioeconomic status inequalities and access to kidney transplantation [12,13,14,15, 17, 18]. Socioeconomically disadvantaged patients may have more comorbidities and lower medication adherence rates. Potential barriers along the path to transplantation have been identified in the United States. Several studies show that transplantation rates are associated with socioeconomic and geographical factors, and vary significantly across different ages, races, and sex [11,12,13,14,15,16,17,18]. There are also some findings regarding culturally-related and local barriers to kidney transplantation among Asians and Pacific Islanders, particularly those residing in resource-deprived neighborhoods [23]. Moreover, a higher social adaptability index is associated with an increased likelihood of being wait-listed for kidney transplant [24]. In our study, we found that only 12.2% of ESKD patients were on the domestic kidney transplant waiting list. Despite Taiwan being a small island, patients with lower individual socioeconomic status and those living in deprived neighborhoods also have less access to transplants. This suggests the existence of several barriers. According to the Taiwan organ-sharing system, patients with ESKD need to return to the outpatient clinic regularly to maintain waitlisting. Patients who did not return beyond 6 months were excluded from the waiting list. Despite the fact that access to the organ share system is universal and free of charge in Taiwan, patients with lower income experience other difficulties, such as the need to work extra hours to support family and the financial burden of transportation to attend medical appointments. Therefore, if patients have low socioeconomic status or live in disadvantaged areas, they may be less likely to return for checkups. Furthermore, low socioeconomic status is associated with lower education in understanding their rights to use social welfare and medical systems. A Canadian study found that Canadians with lower-socioeconomic status used primary care more frequently, but when adjusted for their healthcare needs, they were less likely to receive specialty care [25].
Socioeconomic factors drive outcomes in many areas of healthcare, including access to primary and specialty healthcare, compliance with therapy, ability to afford medications, and outcomes after surgical procedures. This suggests that access to primary care may be a pathway through which income inequality affects mortality rates. Socioeconomic status-driven health inequalities are pronounced even in countries with universal healthcare. A recent study from Canada showed higher mortality among men with lower income, education, and occupational status for several causes of death [26]. In England, socioeconomic status disparities persisted and even widened after the establishment of the National Health Service [28]. The provision of universal coverage was insufficient to offset broader economic and social changes and inequalities. Socioeconomic status differences may be exacerbated by policies that require co-payment for drugs such as intravenous immunoglobulins, or that limit coverage to only several months post-transplantation [12]. However, in our study, individual and neighborhood socioeconomic status are not significantly associated with graft and patient survival after kidney transplantation. This can be attributed to the medical healthcare provided by Taiwan’s NHI and the social welfare system which provides free health coverage to low-income people.
The number of overseas transplants increased rapidly, perhaps because of improved transplantation outcomes, increased brokering activity, and organ supply in China. The number of overseas transplantations in Taiwan increased after 2000, peaked in 2005, and decreased after 2007 [27,28,29]. Taiwanese people can still register in China’s organ-sharing system and undergo kidney transplant in China because Taiwan is considered a part of China. Subgroup analysis revealed no significant differences in the overseas post-transplant mortality and graft failure rates. The Taiwanese healthcare system provides the same post-transplant care for overseas and domestic kidney transplant recipients. However, subgroup analysis for domestic kidney transplants revealed that individuals with high personal and neighborhood socioeconomic status experienced lower risks of graft failure (aHR = 0.55; [95% CI 0.33–0.89], p = 0.017) in domestic kidney transplants, suggesting that there is still need to reduce inequalities. The kidney transplant screening process could be one of the causes of the differences in graft failure. In Taiwan, all kidney transplant recipients receive an insurance that covers complement-dependent lymphocytotoxic cross-match tests to avoid rejection. However, further tests, such as donor-specific antibody screening (Luminex solid-phase assay or C1q assay) and antibody removal treatments, are not covered by this health insurance, and some patients cannot afford these tests. It is desirable that these treatments will be covered by the health insurance.
The strength of this study is that it used a nationwide cohort of ESKD patients to try to avoid selection biases and obtain a sufficient sample size to detect differences among patients with kidney transplantation with different individual and neighborhood socioeconomic status. Choosing the Taiwanese population as a study group may reduce the element of racial differences because over 95% of Taiwan's population is Han Chinese [19]. Furthermore, the diagnosis of ESKD related to dialysis and kidney transplantation is accurate because all medical charts must be reviewed by other hospital experts to confirm the diagnosis and avoid misclassification. However, this study has several limitations. In this study, we did not have detailed patient data, such as the cause of kidney disease and history of sensitization of patients to human leukocyte antigens in the NHIRD. Second, kidney transplantation candidates are selected and those with poor physical or mental health are less likely to be waitlisted. Confounding biases, such as low socioeconomic status, are also often associated with poorer overall health. Hence, the effects of low individual socioeconomic status may be underestimated because this analysis only included patients who successfully completed the process of evaluation and wait-listing. Even though multiple confounding variables such as medical comorbidity (Table 1) were controlled or adjusted for, residual confounding variables may still exist.
In conclusion, this study demonstrates the independent and combined effects of individual and neighborhood socioeconomic status on access to kidney transplantation, but not with the 5-year post-transplantation survival rate. Patients with individual and neighborhood deprivation were less likely to undergo kidney transplantation than those with individual deprivation and neighborhood advantage. However, differences in post-transplantation care are reduced through the follow-up offered by the Taiwanese healthcare system. Improved access to waitlisting through outreach clinics, education, or welfare support may further reduce disparities.



留言 (0)