
記住我


During the study period, 104 patients satisfied our inclusion criteria. Among them, 50 (48.1%) patients were treated with CFDC and 54 (51.9%) with COL. The median age was 66.5 (IQR 58–78) years, 71 (68.3%) patients were male and the median CCI was 5 (IQR 2–7), with a slightly higher CCI in CFDC than COL. At the time of infection onset, 44 (42.3%) patients had a SARS-CoV2 infection, more commonly observed in the COL group (53.7% vs. 30%, p = 0.015) and 66 (63.6%) were hospitalized in the ICU (64.8% vs. 62% in the CFDC and COL group respectively, p = 0.766). Mechanical ventilation was present in 51 (49.5%) patients and 5 (4.8%) patients needed ECMO at the time of infection. Septic shock was present in 33.6% of subjects, higher in the COL group (42.6% vs. 24%). The most frequent source of BSI was primary BSI (45, 43.3%), followed by VAP (27, 26%), CR-BSI (21, 20.2%) and HAP (10, 9.6%), with no significant differences observed between the groups.
Overall, polymicrobial BSIs were identified in 23 out of 104 patients (22.1%), distributed as follows: 6 cases of CRAB/E. faecalis, 5 cases of CRAB/KPC-producing K. pneumoniae, 5 cases of CRAB/vancomycin-resistant E. faecium (VRE), 2 cases of CRAB/S. aureus, 2 cases of CRAB/Candida spp, 2 cases of CRAB/E. cloacae, 1 case of CRAB/KPC-producing K. pneumoniae/Candida spp.
Specifically, among the patients with lung infections, 7 cases exhibited polymicrobial BSI, distributed as follows: 2 cases of CRAB/E. faecalis, 2 cases of CRAB/VRE, 1 case of CRAB/Candida spp, 1 case of CRAB/KPC, 1 case of CRAB/E. cloacae. Notably, in only the latter two cases, KPC and E. cloacae were also detected in bronchoalveolar lavage (BAL) samples, suggesting a genuine polymicrobial lung infection.
The full baseline demographic and clinical features of study population are shown in Table 1.
Table 1 General features and outcomes of study populationCombination therapy was administrated in the majority of patients (78, 75%), of which 36 (72%) treated with CFDC regimens and 42 (77.7%) with COL regimens. The most common associated antibiotic was A/S [median dosage 24 gr/die (range 6–27)], used overall in 42 (40.4%) patients [24 (48%) vs. 18 (33.3%) in CFDC and COL groups, respectively], followed by FOF in 32 (30.8%) patients [median dosage 16 gr/die (range 6–18)] [12 (24%) vs. 20 (37%) in CFDC group and COL group, respectively]. Meropenem was mainly combined with COL than CFDC (12.9% vs. 2%, p = 0.036). All the regimens are described in Supplementary Fig. 1.
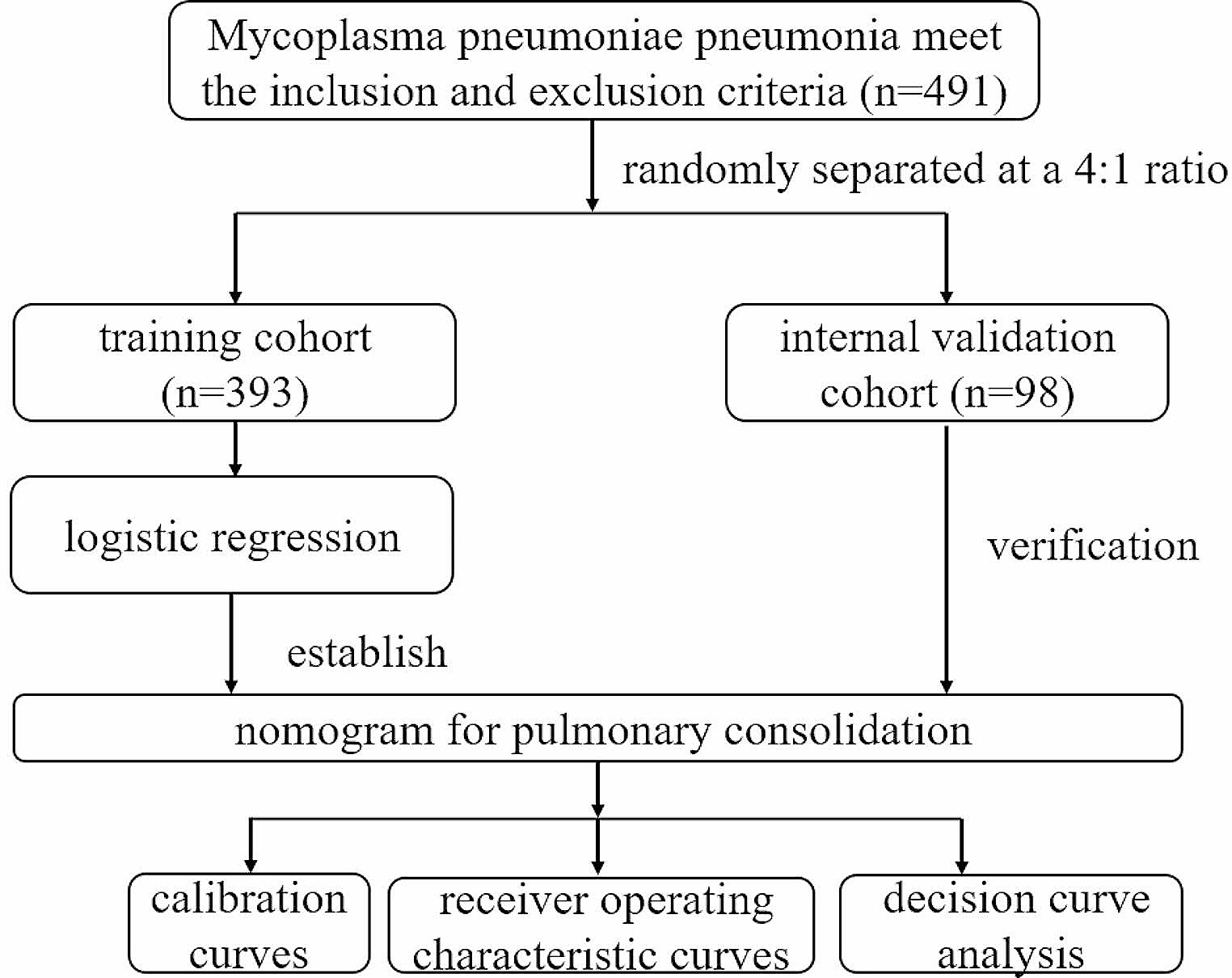
OutcomesWhile the 7-day, 14-day, and 30-day mortality rates did not show significant differences between the two groups, they were lower for the CFDC group compared to the COL group (16% vs. 20.4%, 22% vs. 31.5% and 36% vs. 42.6% for CFDC and COL, respectively). Notably, clinical cure was significantly higher in CFDC than in COL group (66% vs. 44.4%, p = 0.027) (Fig. 1). Details of the comparison between patients with and without clinical cure are shown in Supplementary Table 1.
Fig. 1
Study outcomes and adverse events according to CFDC or COL regimens. CFDC: cefiderocol; COL: colistin. AKI: Acute Kidney Injury
After stratification according to the source of infection, we found that patients with HAP/VAP treated with CFDC had a statistically significant lower 30-d mortality and higher clinical cure than those treated with COL (22.2% vs. 68.4%, p = 0.008, and 72.2% vs. 15.8%, p = 0.0008, respectively), especially in patients with bacteremic VAP (28.6% vs. 76.9%, p = 0.02 and 71.4% vs. 7.7% p = 0.001, respectively) (Fig. 2, panel A-B).
Fig. 2
30-d mortality (Panel A) and clinical cure (Panel B) rates in patients receiving CFDC or COL regimens for HAP or VAP. CFDC: cefiderocol; COL: colistin. HAP: hospital-acquired pneumonia; VAP: ventilator-associated pneumonia
Patients treated with COL exhibited a higher incidence of adverse events compared to those treated with CFDC regimens (38.8% vs. 10%, p < 0.0001), primarily attributed to acute kidney injury (AKI) in the COL group (Fig. 1). In detail, patients receiving CFDC experienced mild gastrointestinal toxicity (n = 4) and increase in sodium values (n = 1), the latter probably due to concomitant A/S administration, while AKI was observed in all the patients treated with COL.
No differences between the two groups were observed as for microbiological cure and rates of infection recurrence or secondary infections (Table 1).
Predictors of 30-d mortalityComparison between 30-d survivors and non-survivors is shown in Table 2. A significative higher mortality was found in older patients (p = 0.040), those with SARS-CoV2 infection (p = 0.002), higher CCI (p = 0.0019), septic shock (p < 0.001), CRRT (p = 0.017) and ECMO (p = 0.004), while source control (when indicated) was protective (p = 0.028), as well as early clinical improvement and clinical cure (p < 0.0001 each).
Table 2 Comparison of 30-d survivors and non-survivorsAt multivariable Cox regression analysis, ICU stay (HR 2.74, 95% CI 1.13–6.65, p = 0.025), SARS-CoV2 infection (HR 2.61, 95% CI 1.31–5.19, p = 0.006), ECMO (HR 8.63, 95% CI 2.68–27.77, p < 0.0001) and CCI (each point increment, HR 1.17, 95% CI 1.05–1.32, p = 0.005) were independently associated with 30-d mortality.
Receiving CFDC was not associated with the primary outcome (HR 0.91, 95% CI 0.45–1.82, p = 0.798), and this finding was further supported by the IPTW analysis (HR 0.74, CI 0.35–1.55, p = 0.431) (Table 3). The standardized mean differences before and after the IPTW procedure for each variable potentially influencing the treatment are shown in Supplementary Table 1.
Table 3 Cox-regression multivariable analysis for 30-d mortality predictorsMicrobiology analysesCFDC susceptibility was available in 59 patients (56.3%), equally distributed between the groups (26/50, 52% and 33/54, 61.1% in CFDC and COL, respectively). CFDC was in-vitro susceptible in all but one subjects, with MIC values ranging from 0.094 to 1.5 µg/mL. The patient with CFDC resistance even before CFDC therapy had MIC 4 µg/mL, exhibited also COL resistance and was eventually treated with COL, MEM and A/S.
Emergence of CFDC in vivo resistance was observed in one patient (MIC 4 µg/mL). Unfortunately, we could not estimate the actual MIC before CFDC treatment since only disk diffusion was available.
COL resistance was observed in 13/104 patients (12.5%). All the strains were resistant to A/S, with MIC > 16/8 µg/mL.
Use of CFDCCFDC was mostly used in combination (36/50, 72%), particularly with A/S (48%) and FOF (24%). CFDC adjustment for renal function was noted in 12 patients, with a slightly higher 30-day mortality observed in those receiving CFDC adjusted for renal function (7/18, 38.8% vs. 5/32, 15.6%, p = 0.08), although the difference did not reach statistical significance. In particular, the patient who experienced in vivo resistance to CFDC was obese and on hemodialysis while treated.
留言 (0)