This meta-analysis is the first to investigate the potential advantages of 3D over 2D laparoscopy for bariatric surgery. In our study, we included trials that compared two video systems for SG [10, 12, 14] and GB [2, 10, 11, 13, 14] procedures. 3D laparoscopy resulted in a significant reduction in the operative time and length of hospital stay among patients undergoing bariatric surgery.
The duration of the surgical procedure influences the risk of rhabdomyolysis, which increases with prolonged immobilization [16]. A shorter duration of surgical procedures decreases the exposure of patients with obesity to anesthetics and the rate of pulmonary complications, including pulmonary embolism secondary to deep vein thrombosis. In fact, prolonged surgery duration and immobilization are independent predictors of postoperative lung diseases, such as atelectasis, pneumonia, pulmonary embolism, and respiratory failure [17, 18]. Prolonged postoperative hospital stay increases hospital costs and the risk of infections and is a predictor of readmission in patients undergoing bariatric surgery [19,20,21].
These results are consistent with those of other previously published meta-analyses or trials investigating the efficacy of 3D and 2D laparoscopies. Cheng et al. [3] observed a shorter duration for surgical procedures in patients undergoing cholecystectomy, prostatectomy, or digestive surgery using a 3D video system. In addition, a randomized controlled trial comparing colon cancer resection performed using 3D and 2D laparoscopies found advantages only in terms of the duration of the surgical procedure in the 3D group, with no observed differences in the length of postoperative hospital stay between the two groups [22].
In the present study, the operative time was significantly shorter in patients undergoing one anastomosis gastric bypass [10] and RYGB [2, 11, 13, 14] with 3D laparoscopy, while there was no statistical difference between the two video systems in patients undergoing SG [10, 14]. This result can be attributed to the fact that the use of 3D may be of little importance in simple tasks, but can increase task efficiency, particularly during the execution of difficult surgical tasks [23], such as suturing and knotting [10, 24]. Indeed, during Roux-en-Y gastric bypass surgery, hand-sewing gastrojejunal anastomosis requires great skill and involves complex interactions between planes [13].
Prolonged recovery can increase the risk of serious postoperative complications, such as hospital-acquired infections [25]. A significant reduction in postoperative hospitalization time was observed in patients undergoing GB. Two studies were evaluated in this setting. Mongelli et al. [2] found that operative time, longer in 2D group, was the only factor independently associated with a prolonged hospital stay. In the study of Padin et al. [14] the high complication rate (4.3% vs 0%) was perhaps the basis for the longer hospital stay of these patients. However, the statistical heterogeneity was high (I2 = 81%, P = 0.02) and it cannot be excluded that our findings were influenced by inherent bias and this constitutes a relevant limitation of the study.
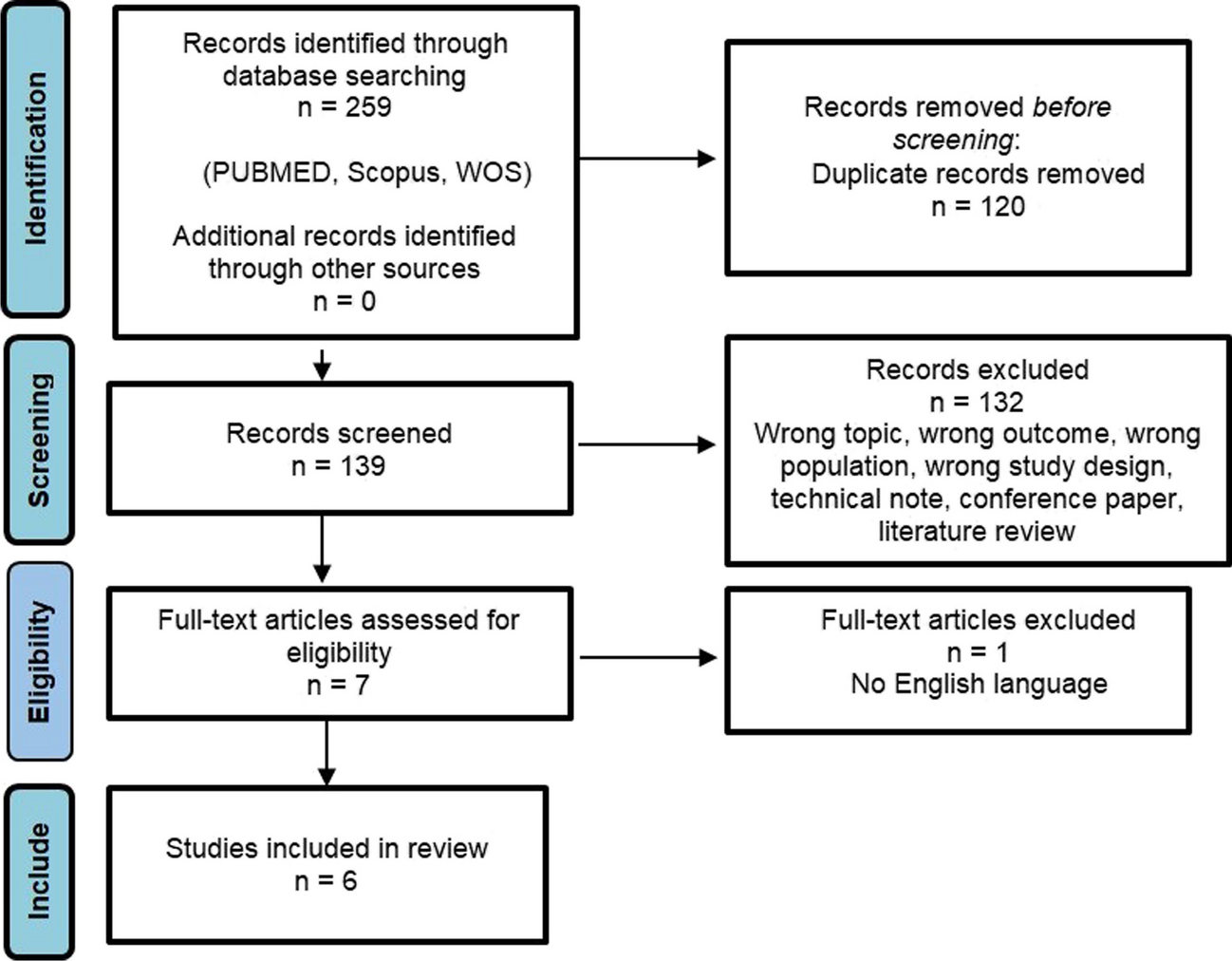
The follow up was reported in four of the six included studies. Complications were observed during recovery and within 30 days of surgery in three studies. Only Martínez-Ubieto et al [12] reported a follow-up of 24 months. As follow up differs among the studies with limited description of the identification of complications, this is considered a further limitation of the study.
Owing to the limited number of complications in the included studies, a narrative synthesis of the results was performed. A high overall complication rate was reported by Martínez-Ubieto et al. [12] in both 2D and 3D groups (22% and 15%, respectively). This is probably due to the included non-surgical and Clavien-Dindo grade I and II complications and a longer follow up. Padin et al. [14] reported a reduction in complications in the 3D cohort compared with the 2D cohort, especially in patients operated on by novice surgeons. The experience of the surgeons performing the procedures may have influenced the study results. Laparoscopic surgeons require extensive experience to overcome the lack of depth perception. However, with experience, the operator becomes accustomed to 2D vision. Experienced laparoscopic surgeons do not require a stereoscopic view to perform simple tasks such as dividing the greater curvature ligaments or constructing the gastric tube during SG using linear staplers [10]. Furthermore, 3D laparoscopy appears to help novice surgeons in reducing complications [14]. Although surgeons are largely skilled in laparoscopic bariatric procedures, there was a limited information on previous experience with 3D system. The surgical team performed more than 100 laparoscopic procedures using 3D laparoscopy in the study of Gabrielli et al. [11]. In contrast, very few or no procedures have been performed in other studies [10, 14]. Despite the surgical team/surgeon was the same for both groups (2D vs 3D) in each included study, surgical background may have a not negligible impact on our findings.
3D laparoscopy may have some disadvantages. The stereoscopic effect may cause headache, nausea and eye strain [26,27,28]. The operating team also must wear polarized glasses to view the screen in 3D with potential inconveniences. Moreover, the benefits of 3D vision such as better depth perception, image quality and spatial orientation may have a limited impact for experienced and skilled laparoscopic surgeons.


留言 (0)