Repair of a fistula between the aorta and right ventricular outflow tract secondary to infective endocarditis of a unicuspid aortic valve and previously repaired ventricular septal defect
In complex cases of IE where there is damage to the fibrous skeleton, a more individualised approach may be required to facilitate adequate debridement of the infection and reconstruction. IE can occasionally result in destruction of periannular tissue leading to abscess cavities, pseudoaneurysm and potential erosion into adjacent chambers and fistula formation. The clinical presentation of aorto-RVOT fistulae will ultimately depend on the size of the shunt created signs of which may include a continuous murmur and/or thrill [4, 5]. When the infection invades toward the right behind the central fibrous body, it reaches the conduction bundle and the atrioventricular node, and damage to these structures results in heart block [6, 7]. The rate of heart failure, VSD and complete heart block have been shown to be greater in patients with fistula formation. This however, has not been shown to be an independent factor for mortality [8].
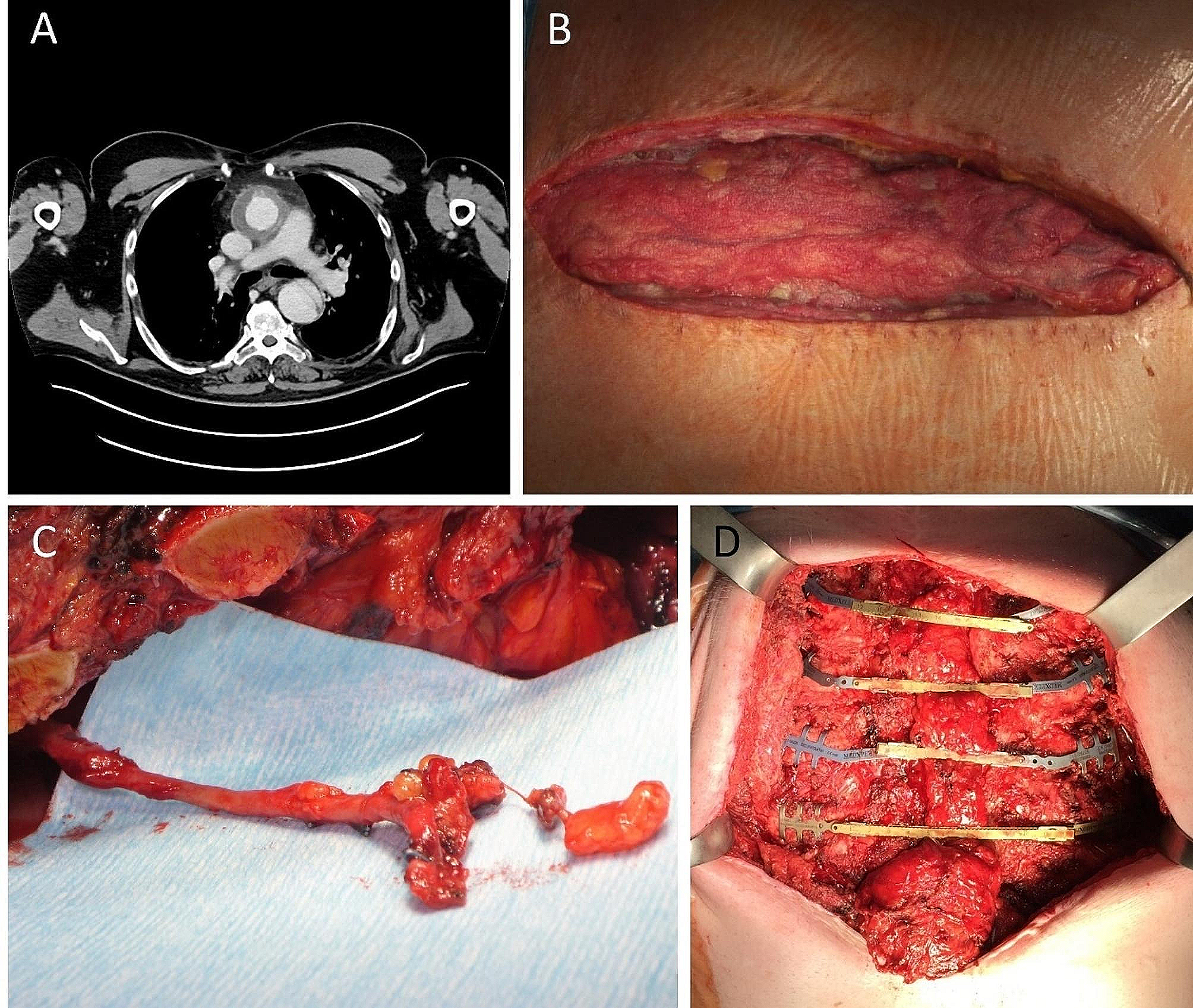
Identification of such structural damage secondary to IE through appropriate investigation is beneficial for surgical planning and helps to determine the intra-operative approach to repair with a combination of echocardiography and cardiac CT [9]. They should ultimately be treated in a timely manner surgically to avoid further destruction of cardiac tissue and conduction system. The aim of surgery is to remove infected tissue, clear and debride infection and cavities, remove embolic sources, and restore cardiac integrity and valve function. Various techniques can be employed for aortic valve endocarditis including valve replacement, root replacement, and aortic homograft implantation. A clear long-term advantage of one technique has yet to be proven [10]. Infective extension of aortic valve endocarditis into the fibrous skeleton may warrant replacement or repair of both the aortic and mitral valve, with reconstruction of the intervening the intervalvular fibrosa (“commando” or “hemi-commando” operation).
With native aortic valve IE, valve repair is rarely a surgical option. In cases where the annulus is destroyed, use of a homograft may be beneficial, but a valved conduit can be considered a viable alternative [11, 12]. This is a complex case demonstrates some of the ‘new problems’ that are to be expected and encountered as we continue the long-term follow up of infants and children undergoing complex congenital heart disease surgery. The key finding in this case has been the significant fistulae secondary to SBE on the background of a unicuspid valve with a previous repair of VSD; and the application of the knowledge that we have gleaned from ‘standard aortic work’ over the years and how this applies to cases of complex congenital heart disease. Furthermore, the importance of accurate documentation from previous surgeries cannot be over emphasised as such details can significantly impact the planning of any future red-surgery. As the complex adult congenital heart disease population ages, it is important to address new and more complex problems with creative thinking by using a multi-modality approach.









留言 (0)