
記住我








An 80-year-old female with transient right upper limb weakness was referred to our institution. Her medical history included hypertension, dyslipidemia, and type 2 diabetes mellitus, all of which were treated with oral medications. Physical examination upon admission revealed a regular pulse of 78 beats/min and a blood pressure of 155/101 mmHg. Blood tests revealed no significant findings and well-controlled dyslipidemia (low-density lipoprotein cholesterol, 67 mg/dL) and diabetes mellitus (hemoglobin A1c 6.2%). Brain magnetic resonance imaging revealed an acute cerebral infarction in the left precentral gyrus. Transthoracic echocardiography (TTE) revealed a tumor that was 20 × 33 mm in the LA. The tumor floated into the left ventricle through the mitral valve orifice during diastole. TTE also showed no significant mitral regurgitation (MR) or mitral stenosis (MS) and a left ventricular ejection fraction of 72%. Transesophageal echocardiography (TEE) revealed a left atrial tumor attached to the anterior mitral leaflet, with no significant MR or MS (Fig. 1). Cardiac computed tomography revealed a left atrial tumor attached to the posterior wall of the LA, close to the coronary sinus (Fig. 2), and no substantial coronary artery stenosis. However, tumor nutrient vessels were not detected. We considered this patient to be at risk of embolization and sudden death. Therefore, we planned a cardiac tumor resection four days after diagnosing the patient with acute cerebral infarction.
Fig. 1
Preoperative transesophageal echocardiography. The left atrial tumor (yellow arrow) was attached to the anterior mitral leaflet. No significant mitral regurgitation was observed (A, B)
Fig. 2
Cardiac CT. The left atrial tumor (yellow arrow) had no significant nutrient vessels. Its stalk was attached to the posterior wall of LA (yellow arrowhead). This tumor is close to the coronary sinus and its ostium (white arrowhead) and atrioventricular node (red circle). CT: computed tomography, LV: left ventricle, AS: atrial septum, LA: left atrium, RA: right atrium
General anesthesia was induced. Subsequently, a median sternotomy was performed, and cardiopulmonary bypass (CPB) was established via aortic and bicaval cannulations. The aorta was cross-clamped, and the heart was arrested with antegrade cardioplegia. The LA was examined using a right-sided left-atrial approach. The tumor was observed to be dark red, jelly-like, and approximately 30 mm in size. Its stalk was attached to the posterior wall of the LA, close to the AV node and orifice of the coronary sinus (Fig. 3). Therefore, an atrial septal incision was performed. The tumor was delicate and had to be resected into pieces. Special care was taken to avoid damage to the coronary sinus and AV node, as the stalk was resected with a 5 mm margin around its base. The atrial septum and LA were closed directly. After declamping the ascending aorta, the patient had a CAVB. Intraoperative TEE demonstrated severe mitral regurgitation due to A2 prolapse (Fig. 4). Myxomas have the potential to mask mitral valve prolapse. Consequently, cardiac arrest was performed again, and mitral valve repair was conducted with artificial chordae reconstruction, 28-mm Sorin-MEMO 3D annuloplasty ring (Sorin Group Italia S.r.L., Saluggia, Italy), and P1/P2 indent closure. A saline test revealed no significant MR. The patient was easily weaned from CPB, and protamine was systemically administered. As her heart rhythm was CAVB, temporary pacing was necessary.
Fig. 3
Intraoperative findings. The tumor was dark red, jelly-like, and approximately 30 mm in size. It was attached to the posterior wall of the LA (black arrow). LA: left atrium
Fig. 4
Intraoperative transesophageal echocardiography. Before tumor resection, no significant MR was detected (A). After tumor resection, severe MR due to A2 prolapse was demonstrated for the first time (B). MR: mitral regurgitation
Postoperative histopathological analysis revealed that the tumor was a myxoma with no tumor cells in the resected margin (Fig. 5), and TTE showed no evidence of residual tumor, trivial MR, or significant atrial shunt flow. Pacemaker implantation was performed for the CAVB on the 11th postoperative day, and the patient was discharged on the 21st postoperative day.
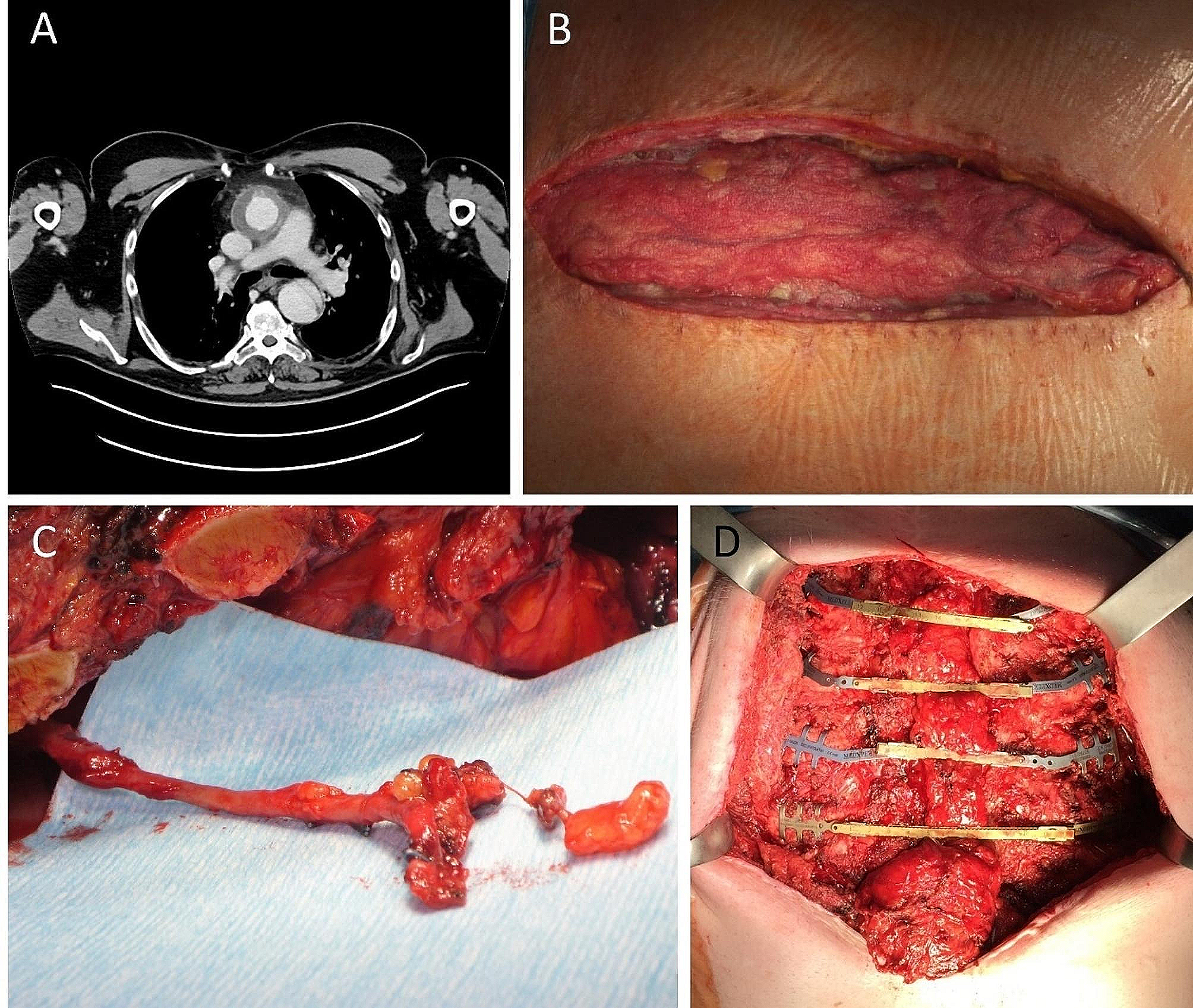
Fig. 5
Histological examination. The resected specimen was observed to be dark red and jelly-like (A). The tumor was composed of stellate and spindled cells (B, hematoxylin & eosin, ×40). Tumor cells were CD34 positive (C, immunohistological staining of CD34, ×100)
留言 (0)