
記住我
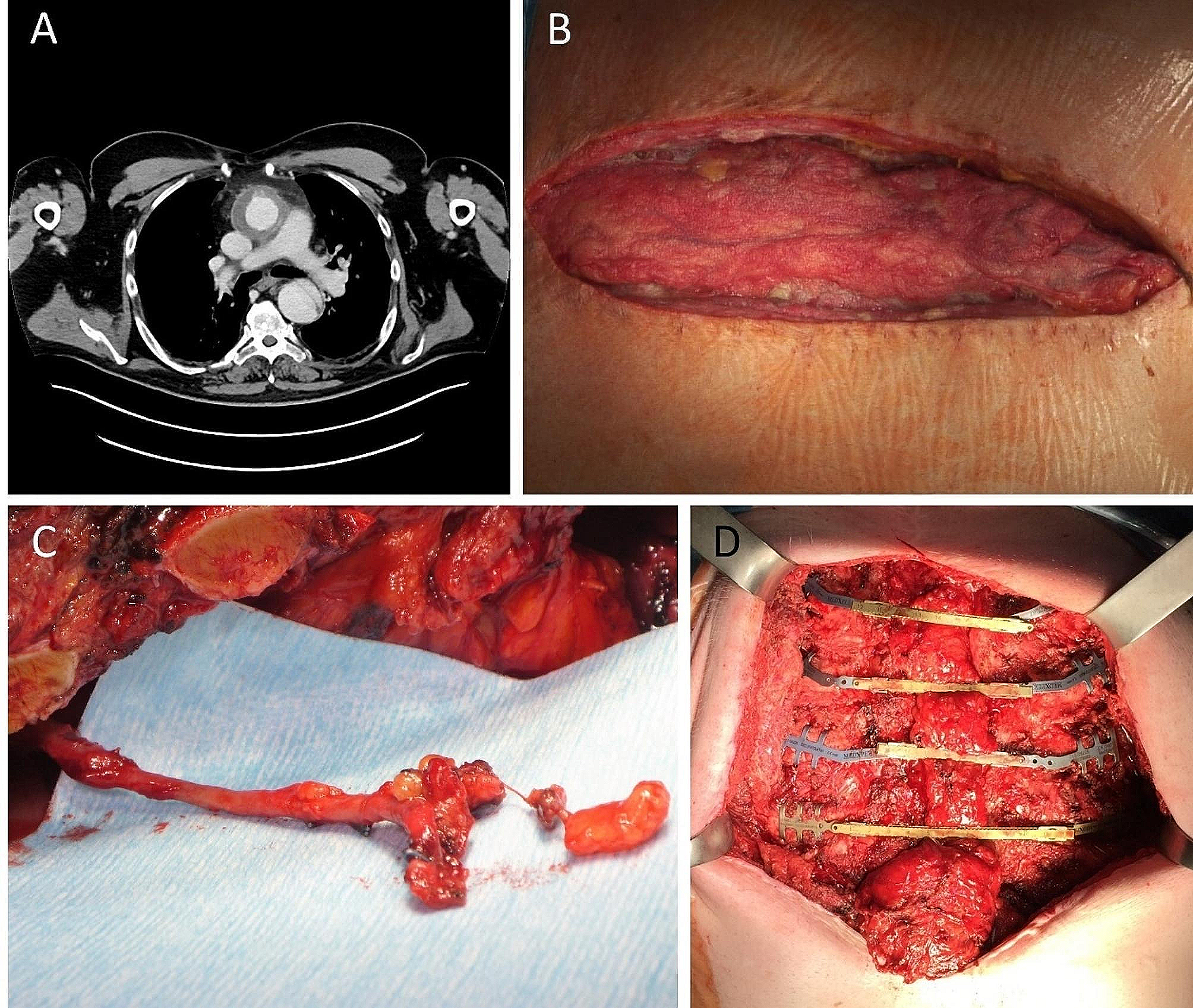








A 48-year-old hypertensive smoker, presented with a history of progressive shortness of breath (Medical Research Council dyspnoea grade 2) [4]. Initial clinical examination and laboratory tests were unremarkable for thoracic pathology. A chest radiograph (CXR) identified a widened mediastinum along with a left upper zone mass. This was confirmed on subsequent Computed Tomography (CT) and Positron-Emission Tomography (PET) scans (Fig. 1a, b and c) as being an fluorodeoxyglucose (FDG) avid left anterior mediastinal and upper lobe lung mass with an avid station 5 mediastinal lymph node, and a PET avid right thymic satellite nodule seen adjacent to the junction between the left innominate vein and superior vena cava (SVC). A CT biopsy of the mediastinal mass showed carcinoid of unknown origin. This was staged as T4N3M0 [5]. T4 due to mediastinal and lung involvement and N3 due to the right thymic nodule which was debated as lymph node or nodule. Staging nodal assessment was not felt possible as only station 5 was avid and pathological. The MDT considered surgical and oncological treatment options and given the carcinoid diagnosis, surgical excision was felt to be the apt option.
Fig. 1
A Axial CT scan demonstrating left anterior mediastinal mass B & C Axial PET showing FDG avid right thymic nodule and left anterior mediastinal tumour involving the left upper lobe
IntraoperativelyThe surgical targets were the right thymic nodule, the left thymic lobe and the left upper lung lobe. To reduce the incision related morbidity, the initial plan was keyhole access for the left hemithorax and then a sternotomy to inspect the right thymic area abnormality and its possible excision. On inspection of the left hemithorax via robotic access, the tumour was found to involve the left upper lobe of the lung with direct confluent spread to the left thymic lobe and left phrenic nerve. Given the adhesions and bulk, we converted to a left posterolateral thoracotomy and completed the left upper lobectomy with complete gross excision of neighbouring mediastinal fat, left phrenic nerve and lymphadenectomy of station 5 with sampling of left stations 10, 11, 9 and 7. The main specimen was left attached to the left thymic lobe to avoid any spillage. The thoracotomy was closed, patient rolled into a supine position and a median sternotomy was performed. The right thymic nodule from the CT was found as a discrete nodule in the body of the right thymic lobe adjacent to the junction between the left brachiocephalic vein and superior vena cava (SVC). Due to dense adhesions with the pericardium, both thymic lobes were radically resected with the underlying attached pericardium. The entire detached specimen was extracted without spillage in a large retrieval bag via the sternotomy. The residual pericardial defect was from the SVC to the left atrial appendage (LAA). Although the pericardial defect was large, it was felt that this defect was mostly anterior and cardiac herniation could be prevented by left lower lobe expansion and a raised left hemidiaphragm. 2 pleural and 1 mediastinal chest drains were placed on suction.
Clinical deteriorationOn day 1 post-operatively, the patient looked well, had stable observations and was mobilising adequately. Later in the day, he suddenly became clammy with oligoanuria but normotension (103/76mmHg) and bradycardia. A newly placed central venous catheter showed a central venous pressure (13mmHg) and raised troponins (1073 ng/L). The blood pressure responded to intravenous crystalloid boluses but his 12-lead ECG showed bradycardia with a junctional rhythm, with no capture in chest leads V1-2 (Fig. 2). A bedside transthoracic echocardiogram could not obtain sufficient acoustic windows. A CXR showed left sided shift of the mediastinal contents (Fig. 3a). When posterior ECG leads were applied along the inferior scapular line, as was the echocardiogram probe, positive deflections and acoustic windows were seen. All these features together were suggestive of cardiac herniation. He was transferred to the intensive care unit for haemodynamic optimisation with judicious filling and dobutamine.
Fig. 2
Initial 12-lead ECG of patient showing junctional rhythm and lack of capture in chest leads V1-V2
Fig. 3
A CXR pre repair of cardiac herniation showing mediastinal shift B CXR post reduction and repair of pericardial defect, showing a midline mediastinum
Redo operationThe patient underwent a redo-sternotomy on day 2. The heart had herniated into the left thoracic cavity with the left ventricular apex pointing towards the spine, causing marked inferior caval kinking. After reducing the heart back to its normal anatomical lie, the pericardial defect (approximately 15 cm x 10 cm) was repaired using a GoreTex patch. Fenestrations were made in the patch to prevent cardiac tamponade. Bronchoscopy showed endobronchial secretions which were suctioned out. The left lower lobe re-expanded well. The post-operative CXR demonstrated resolution of the mediastinal shift and adequate left lung re-expansion (Fig. 3b). The ECG trace returned to normal sinus rhythm. The patient recovered well clinically and biochemically. The final histopathology showed a completely resected TTF1 negative atypical carcinoid pT3N2 (from station 5) M0 R0 of thymic origin.
留言 (0)