Movement is life. From birth to death and every moment in between, even when we are asleep, people move, and change position. This makes the condition of a long-term medically induced coma as is standard practice for certain critically ill patients, a stress to normal human physiology. Even in healthy individuals, bed rest is damaging to multiple-organ systems-depleting bone density, maladapting the vestibular system, the baroreceptors in the vascular system, muscle structural integrity, cardiopulmonary power, and efficiency within 3 days (1). Metabolic derangements and insulin resistance damage the capability of skeletal muscle to function and support homeostasis as immobility and illness accelerate muscle catabolism without necessary anabolic rebuilding (2,3).
It is within this holistic physiology framework that the first modern randomized control trial (RCT) of “Early Physical and Occupational Therapy” led by Schweickert et al (4), was conducted over a decade and a half ago. This landmark study challenged our long-held beliefs that sedation and bed rest were necessary components of ICU care and showed us that this type of intervention was not only feasible but could reduce the burdens of postcritical illness disability.
Based on these findings, and those from subsequent studies, clinical practice guidelines from multiple professional societies, including the Society for Critical Care Medicine, have recommended that patients with critical illness be physically active early and often seems a straightforward directive (5–7). Nevertheless, implementation of these interventions in clinical practice remains low (8). Although this may simply reflect the well-described delay between research findings and clinical practice, it may also reflect the fact that findings from the largest of these trials are mixed (4,9–13). As a result, some would argue that early mobility has not been shown to improve outcomes therefore mobilizing patients without clear evidence of a benefit is not worth the personnel effort and costs and may expose patients to harm. Others may argue that negative studies were poorly conducted, lacked important elements of effective interventions, did not deliver enough of the intervention, or delivered it too late. Ultimately more studies will be needed to resolve these conflicts and dictate clinical care. Nevertheless, repeating the same studies with the same methodologies is unlikely to achieve this end. Therefore, future studies of physical rehabilitation will need to be conducted with greater rigor and reproducibility.
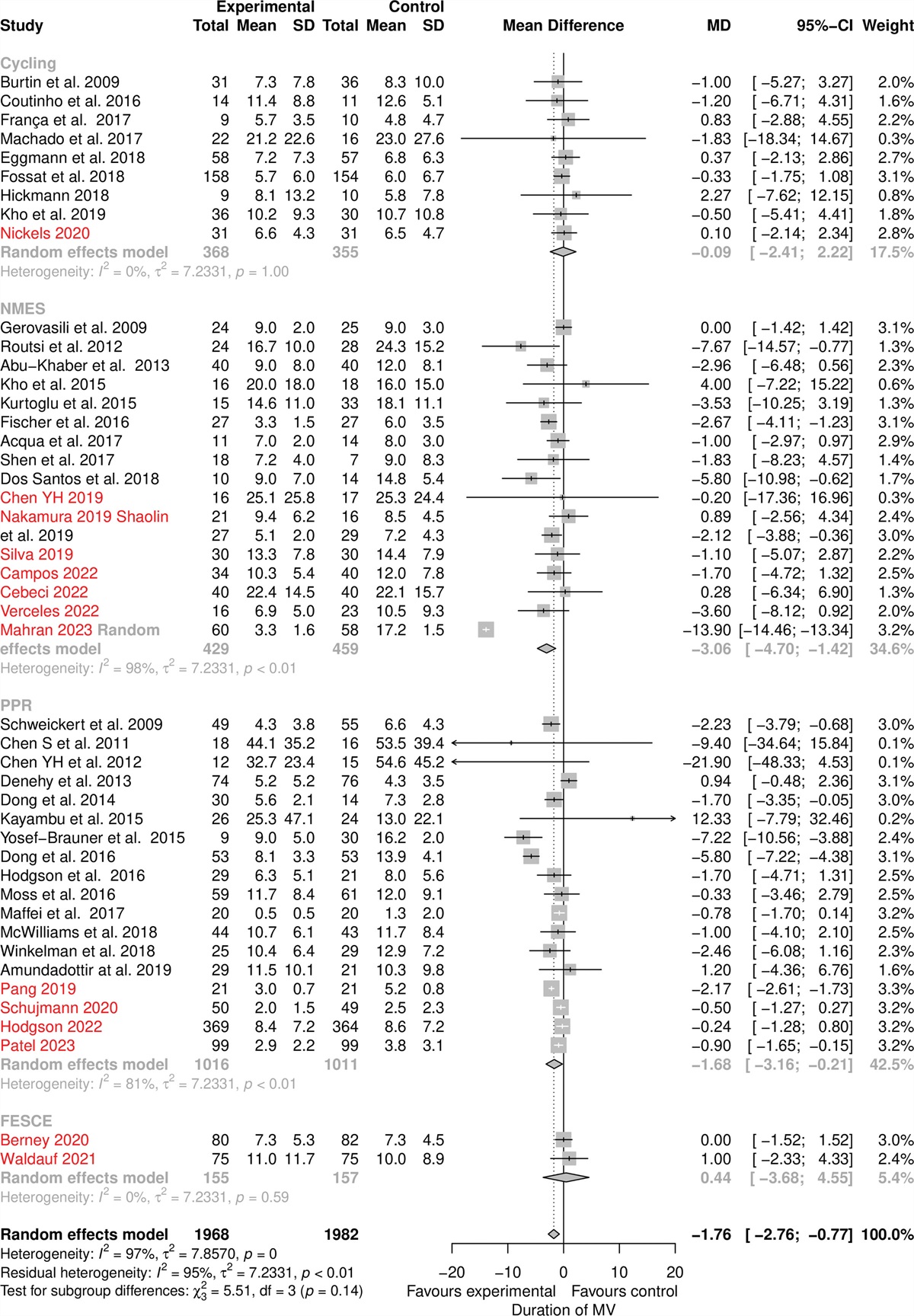
To date, interventions falling under the umbrella of physical rehabilitation in those with critical illness include physical and occupational therapy, early mobility, in-bed interventions, neuromuscular electrical stimulation, and cycle ergometers. Furthermore, within each type of intervention, the elements and personnel who deliver the intervention differ between studies. Together, these differences contribute to the heterogeneity of this body of research and likely contribute to inconsistent findings (14). For example, a recent meta-analysis of physical rehabilitation showed that interventions where patients move out of bed, improved physical function at hospital discharge, reduced the amount of time patients required mechanical ventilation, and decreased ICU and hospital length of stay; compared with in-bed modalities such as neuromuscular electrical stimulation or in-bed cycling suggesting these types of interventions may be the most effective (15,16). Yet not all studies of out-of-bed interventions have been shown to improve outcomes (10,12,13).
Rigorous and reproducible research allows other researchers to replicate a study and improve the chances that similar results will be obtained in similar populations. A key component of rigor and reproducibility is treatment fidelity. Treatment fidelity describes the extent to which an intervention is delivered as planned (i.e., the extent to which the intervention protocol was followed, the dose of intervention delivered, how often it was delivered, who delivered it, and how well it was delivered). Without reporting treatment fidelity, we cannot understand if positive studies are positive because of the intervention or because of other factors that were unintentionally added (or left out) to the intervention. In negative studies, it is unclear if the intervention does not work or if the protocol was not followed.
In this issue of Critical Care Medicine, Farley et al (17) conducted a scoping review of the reporting of treatment fidelity in studies of physical rehabilitation in patients with critical illness. The authors identified 94 studies that assessed a range of physical rehabilitation modalities. To understand treatment fidelity, the authors assessed the number of treatment fidelity components defined by an expert panel of behavioral scientists (i.e., study design and treatment, interventionalist training, how well study participants understood the intervention, could perform the skills taught in the intervention, and how well participants used the intervention skills outside of study interventions), The key finding of the study was that, on average, studies reported only one of five of these elements, with a median of 19% treatment fidelity components reported across studies. Studies also reported significantly more elements related to study design and interventionalist training than those elements related to how well participants understood and applied the intervention. Perhaps reflecting these findings, the number of components reported in intervention groups (24%) was greater than those reported in the control groups (14%) and far from the target the authors hoped for 70%. The authors conclude that research into methods by which to improve treatment fidelity is needed to improve studies of ICU physical rehabilitation.
The authors are commended for bringing to light the importance of treatment fidelity in these complex studies so that we can better understand their strengths and weaknesses. Further, by drawing parallels between behavioral science interventions and physical rehabilitation interventions for those with critical illness, the authors provide a novel framework from which to build future interventions.
How might better reporting of treatment fidelity help advance the field of physical rehabilitation in survivors of critical illness? Over 20 years ago, recognizing the need to improve the rigor of studies related to behavioral change that affects health behaviors (e.g., smoking, unhealthy diet, sedentary behavior) the National Institutes of Health (NIH), with support from private foundations, founded the NIH-Behavioral Change Consortium (NIH-BCC) (18). The mission of the NIH-BCC was to establish best practices for studies evaluating the efficacy and effectiveness of health behavior interventions. Among the products developed by the NIH-BCC was the development of recommendations to improve treatment fidelity by identifying important concepts and best practices for health behavior research. These recommendations covered five areas: study design, training providers, delivery of treatment, receipt of treatment, and enactment of treatment skills. In the following section and in Table 1, we apply this treatment fidelity framework to ICU physical rehabilitation, proposing ideas for how to improve future studies.
TABLE 1. -
National Institutes of Health-Behavioral Change Consortium Treatment Fidelity in ICU Early Mobility
Treatment Fidelity Element
Study Design
Training Provided
Delivery of Treatment
Receipt of Treatment
Enactment of Treatment Skills
National Institutes of Health Behavioral Change Consortium description
• Ensure same treatment dose within conditions
• Ensure equivalent dose across conditions
• Plan for implementation setback
• Standardize training
• Ensure provider skill acquisition
• Minimize “drift” in provider skills
• Accommodate provider differences
• Control for provider differences
• Reduce differences within treatment
• Ensure adherence to treatment protocol
• Minimize contamination between conditions
• Ensure participant comprehension
• Ensure participant ability to use cognitive skills
• Ensure participant ability to perform behavioral skills
• Ensure participant use of cognitive skills
• Ensure participant use of behavioral skills
Physical rehabilitation interventions
Equivalent number of sessions; same length of sessions for participants
Ensure same intervention is delivered regardless of critical illness (e.g., delirious, mechanically ventilated)
Report the intensity and dosage of the intervention relative to patient capability and premorbid functioning
Train multiple interventionalists to accommodate those who may leave the study during its conduct
Standardize training of all interventionalists
Establish and train interventionalists to performance criteria; measure these before and during the study
Regular refresher training, and use of observations collected during intervention to ensure intervention components are delivered appropriately
Provide training for interventionalists according to their needs/experience
Prioritizing intervention as essential, not ancillary
Simulating and practicing needed communication skills for providers
Simulation training for manual skills needed and use of equipment
Report quantity of chosen rehabilitation modality, including specific activities performed, and inclusion of activities performed by control groups
Monitor for nonspecific treatment effects (e.g., rapport with patients)
Use treatment manuals. Review intervention delivery regularly with “spot checks” to ensure adherence and that the content and “dose” of treatments follow protocol
Reduce cross-contamination by having different interventionalists; train interventionalists in the importance of avoiding cross-contamination
Ensure appropriate sedation management and reporting of sedation practices
Explain intervention to participants in a manner that is able to be understood by those with delirium, cognitive impairment, or who have low health literacy
Assess participants’ understanding of skills being taught; interventionalists provide feedback to participants
Determine participant goals for mobility intervention
Empower participants to ask to get out of bed and move
Report how often patients perform these activities outside of intervention periods
Evaluate strategies to provide psychologic counseling and emotional care.
Empower patients to advocate for greater physical activity throughout their hospital stay
Measure the ability and/or confidence of patients to perform mobility tasks.
Assess participants’ complete mobility tasks outside of intervention sessions.
Measure whether participants’ goals were met by the intervention
STRATEGIES FOR IMPROVING STUDY DESIGN: BETTER METHODS FOR REPORTING THE “DOSE” OF INTERVENTION
In the largest RCT to date for the mobility of mechanically ventilated patients—by Hodgson et al for the TEAM trial Investigators titled Early Active Mobilisation in the ICU (10), the ICU mobility scale was used to report the highest level of activity achieved per patient session. Although this scale has both face and construct validity and is one of the more detailed measures of mobility in the ICU, sections of this scale allow for patients to perform a wide range of activities that may represent variations of strength to receive the same score (19). For example, a score of “4, Standing” includes doing so with or without assistance along with the use of devices to facilitate standing (e.g., a standing lifter device or tilt table). Thus, a range of patients including those who are profoundly weak and patients capable of independent standing, received the same score despite the variation in the amount of exercise relative to patient’s body composition and physiologic stress. Future tools used to report the dose of intervention should express the intensity and dosage of the intervention relative to patient capability and premorbid functioning (9).
STRATEGIES FOR IMPROVING PROVIDER TRAINING: REPORT DETAILS OF PROVIDER TRAINING AND CULTURAL PRACTICES RELATED TO PHYSICAL REHABILITATION
Any physical rehabilitation provided to an ICU patient depends heavily on the training of the provider, their clinical background, which assessments are used to determine a patient’s abilities to perform the intervention, motivational and communication skills, and the culture of the ICUs where the interventions are studied. For example, a cohort of 48 medical ICU nurses was trained to initiate mobilization out of bed of mechanically ventilated patients after they met specific clinical parameters (e.g., Richmond Agitation Sedation Scale 2 to –2, Fio2< 0.6, positive end-expiratory pressure < 10 cm H2O, Spo2 > 90%, mean arterial pressure > 60, systolic blood pressure < 200, and no titration of ionotropic medications for >12 hr). Despite the training intervention, when 105 of 191 enrolled patients met predefined eligibility criteria within 2 days of intubation, not one of the qualifying patients mobilized out of bed (20). First, these data highlight the importance of providing detailed reports of training provided to personnel delivering physical rehabilitation interventions. Second, they highlight that despite training providers to deliver a planned out-of-bed mobilization protocol, providers can encounter multiple barriers that prevent the patient from receiving out-of-bed mobility. Thus, anticipating, addressing, and reporting barriers to intervention delivery is needed.
STRATEGIES FOR IMPROVING MONITORING AND IMPROVING DELIVERY OF TREATMENT: REPORTING INTERVENTION MODALITIES AND SPECIFIC ACTIVITIES
The goal of all physical rehabilitation interventions is to improve mobility, yet some interventions may “impede” patient functional mobility rather than enhance it (21). One trial randomized previously independent, mechanically ventilated, critically ill adults to a control group receiving standard physiotherapy including early mobilization, or to an experimental group with early endurance and resistance training combined with mobilization. Patients randomized to the intensive rehabilitation group received significantly more physiotherapy (sessions: 407 vs. 377, p < 0.001; time/session: 25 min vs. 18 min, p < 0.001) with all additional time spent in bed cycling while the control group spent more time achieving higher levels of out-of-bed activity with no time on bed bicycling (21). The study found no differences between the groups in participants’ functional capacity or independence at hospital discharge in the group who performed more functional out-of-bed activity training, even though this occurred at a lower frequency and duration than the intervention group, supporting the idea that out-of-bed activity may be more beneficial (15). Thus, methods for reporting the quantity of the chosen rehabilitation modality, including specific activities performed, and inclusion of activities performed by control groups, will help to reduce differences between studies, provide clear information about how well the protocol was adhered to, and whether there was contamination between groups.
STRATEGIES FOR IMPROVING RECEIPT OF TREATMENT: REPORTING SEDATION PRACTICES
In addition to confounding mobility interventions, sedation practices during patient rest times, have a tremendous impact on the capability of a patient to participate in and comprehend the intervention. Furthermore, as patients awaken from sedation, they need to recalibrate their sense of self, autonomy, and power to rebuild their unfamiliar new weakened selves, which may lessen the effects of the intervention (22). For example, two randomized trials of physical rehabilitation where the intervention was paired with sedation interruption found a benefit to physical rehabilitation (4,11), whereas those where sedation was not specifically managed failed to show benefit (12,13). Explicitly managing sedation helps to reduce differences in intervention delivery and facilitates adherence to the intervention protocol, thus future studies should ensure appropriate sedation management and reporting of sedation practices.
Improving monitoring and enactment of treatment: Measure activities occurring outside of interventions. Similarly, ICU mobility studies often fail to account for patient activity levels during nonintervention hours of the day. Performing mobility activities outside of intervention periods can reflect how well participants are using the behavioral and cognitive skills learned during the intervention. By reporting how often patients perform these activities outside of intervention periods, we will begin to understand how well they are progressing physically, but also their abilities to understand the intervention and how they may apply it both in the hospital and afterward. In addition, studies should evaluate strategies to provide psychologic counseling and emotional care to empower patients to advocate for greater physical activity throughout their hospital stay.
Beyond avoiding physically harmful bed rest and in the face of an inconclusive evidence base, early mobility interventions remain vital to the physical and psychologic recovery of patients with critical illness. The low rates of reporting treatment fidelity reported by Farley et al (17) must not discourage us from allowing our patients to actively participate in the most basic human need for autonomous movement while we wait for definitive data produced by future, -reported, trials. Rather, their study should serve as an inspiration to improve future research studies and to examine ICU provider behaviors needed to help our patients move.
REFERENCES
1. Spiering BA, Weakley J, Mujika I: Effects of bed rest on physical performance in athletes: A systematic and narrative review. Sports Med. 2023; 53:2135–2146
2. Eggelbusch M, Charlton BT, Bosutti A, et al.: The impact of bed rest on human skeletal muscle metabolism. Cell Rep Med. 2024; 5:101372
3. Fazzini B, Märkl T, Costas C, et al.: The rate and assessment of muscle wasting during critical illness: A systematic review and meta-analysis. Crit Care. 2023; 27:2
4. Schweickert WD, Pohlman MC, Pohlman AS, et al.: Early physical and occupational therapy in mechanically ventilated, critically ill patients: A randomised controlled trial. Lancet. 2009; 373:1874–1882
5. Devlin JW, Skrobik Y, Gelinas C, et al.: Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2018; 46:e825–e873
6. Lang JK, Paykel MS, Haines KJ, et al.: Clinical Practice Guidelines for Early Mobilization in the ICU: A Systematic Review. Crit Care Med. 2020; 48:e1121–e1128
7. Daum N, Drewniok N, Bald A, et al.: Early mobilisation within 72 hours after admission of critically ill patients in the intensive care unit: A systematic review with network meta-analysis. Intensive Crit Care Nurs. 2024; 80:103573
8. Ashkenazy S, Ganz FD, Kuniavsky M, et al.: Patient mobilization in the intensive care unit: Assessing practice behavior—a multi-center point prevalence study. Intensive Crit Care Nurs. 2024; 80:103510
9. Scheffenbichler FT, Teja B, Wongtangman K, et al.: Effects of the level and duration of mobilization therapy in the surgical ICU on the loss of the ability to live independently: An international prospective cohort study. Crit Care Med. 2021; 49:e247–e257
10. TEAM Study Investigators and the ANZICS Clinical Trials Group; Hodgson CL, Bailey M, Bellomo R, : Early active mobilization during mechanical ventilation in the ICU. N Engl J Med. 2022; 387:1747–1758
11. Schaller SJ, Anstey M, Blobner M, et al.; International Early SOMS-guided Mobilization Research Initiative: Early, goal-directed mobilisation in the surgical intensive care unit: a randomised controlled trial. Lancet. 2016; 388:1377–1388
12. Morris PE, Berry MJ, Files DC, et al.: Standardized rehabilitation and hospital length of stay among patients with acute respiratory failure: A randomized clinical trial. JAMA. 2016; 315:2694–2702
13. Moss M, Nordon-Craft A, Malone D, et al.: A randomized trial of an intensive physical therapy program for patients with acute respiratory failure. Am J Respir Crit Care Med. 2016; 193:1101–1110
14. Zhang L, Hu W, Cai Z, et al.: Early mobilization of critically ill patients in the intensive care unit: A systematic review and meta-analysis. PLoS One. 2019; 14:e0223185
15. Waldauf P, Jiroutková K, Krajčová A, et al.: Effects of rehabilitation interventions on clinical outcomes in critically ill patients: Systematic review and meta-analysis of randomized controlled trials. Crit Care Med. 2020; 48:1055–1065
16. Wang YT, Lang JK, Haines KJ, et al.: Physical rehabilitation in the ICU: A systematic review and meta-analysis. Crit Care Med. 2022; 50:375–388
17. Farley C, Newman ANL, Hoogenes J, et al.: Treatment Fidelity in 94 Randomized Control Trials of Physical Rehabilitation in the ICU: A Scoping Review. Crit Care Med. 2024; 52:717–728
18. Bellg AJ, Borrelli B, Resnick B, et al.; Treatment Fidelity Workgroup of the NIH Behavior Change Consortium: Enhancing treatment fidelity in health behavior change studies: Best practices and recommendations from the NIH Behavior Change Consortium. Health Psychol. 2004; 23:443–451
19. Hodgson C, Needham D, Haines K, et al.: Feasibility and inter-rater reliability of the ICU mobility scale. Heart Lung. 2014; 43:19–24
20. Cooper D, Gasperini M, Parkosewich JA: Nurses’ perceptions of barriers to out-of-bed activities among patients receiving mechanical ventilation. Am J Crit Care. 2021; 30:266–274
21. Eggmann S, Verra ML, Luder G, et al.: Effects of early, combined endurance and resistance training in mechanically ventilated, critically ill patients: A randomised controlled trial. PLoS One. 2018; 13:e0207428
22. Zhang H, Sheng Y, Yu C, et al.: Understanding the needs and perceptions of early mobilization for critically ill patients: A systematic review of qualitative studies. Intensive Crit Care Nurs. 2023; 81:103584









留言 (0)