This retrospective investigation included 110 patients who were diagnosed with oesophageal cancer coupled with hyperlipidaemia and who underwent oesophagectomy for the management of their oesophageal malignancy. The analysis conducted in the study highlighted a significant improvement in lipid profiles following oesophagectomy that could help reduce the risk of cardiovascular diseases. Variations in the extent of improvement were observed among different subtypes of hyperlipidaemia, with mixed hyperlipidaemia exhibiting the most pronounced remission rate. Further scrutiny revealed a discernible correlation between alterations in lipid parameters and weight reduction.
The beneficial influence of bariatric surgery on lipid homeostasis has been substantiated by a wealth of literature. Recent investigations have demonstrated that bariatric procedures substantially ameliorate lipid profiles, manifesting as a cardio-protective synergy involving reductions in TC, LDL, TG, and elevated HDL [15]. In concordance, a comprehensive review revealed that one year postbariatric surgery, patients exhibit reduced LDL and TG levels, elevated HDL levels, diminished left ventricular dimensions and mass, and heightened ejection fractions [16]. Kjellmo CA et al. reported that bariatric surgery elicited a favourable modulation of lipoprotein profiles among morbidly obese individuals, characterized by lowered LDL and apoB levels, an attenuated SAA/PON1 ratio, and augmented HDL concentrations. Nevertheless, this intervention did not affect cholesterol efflux capacity [17]. Moreover, retrospective inquiries have alluded to a diminished cardiovascular disease risk among individuals undergoing laparoscopic sleeve gastrectomy, manifesting as a substantial 12.7% increase in HDL levels and a 22.9% decrease in TG levels [18]. Correspondingly, the findings in the study are consistent with these observations. In an investigation involving 110 patients with oesophageal cancer and hyperlipidaemia who underwent oesophagectomy, a notable 16.7% increase in HDL levels was observed one year postprocedure. Conversely, TG, LDL, and non-HDL levels decreased by 14.3%, 26.7%, and 23.2%, respectively. In summary, both oesophagectomy and bariatric surgery have demonstrated lipid ameliorative effects.
To discern a rationale for the improvements in lipid profiles, it is pertinent to note that plasma gastrin levels exhibit a noteworthy reduction subsequent to laparoscopic sleeve gastrectomy. This reduction correlates with a diminished appetite and decelerated gastric emptying, subsequently fostering effective weight loss during the postoperative period [19]. These mechanisms may underpin the observed alterations in HDL and TG levels during the postoperative phase. Notably, parallels exist between the surgical manoeuvres employed in oesophageal cancer resection and sleeve gastrectomy. Several studies have elucidated the utility of the tube stomach technique in oesophagectomy for oesophageal cancer. Some scholars posit that the diameter of the tube stomach closely approximates that of the oesophagus. This physiological feature reduces the food retention time within the thoracic stomach, bolstering peristaltic activity and preventing thoracic-gastric syndrome attributed to gastric retention. Moreover, partial gastric tissue resection during these surgeries curtails gastric acid secretion, consequently preventing postoperative reflux oesophagitis. Furthermore, the tube stomach technique has been shown to effectively diminish the incidence of postoperative respiratory and circulatory complications [20]. This finding emphasizes that both oesophagectomy and sleeve gastrectomy entail partial gastric tissue removal, which results in a reduction in gastric volume. This, in turn, diminishes gastric lipase secretion as well as the release of cholecystokinin, a hormone known to stimulate the secretion of digestive enzymes such as lipases and proteases. These cumulative effects culminate in a marked reduction in triglyceride hydrolysis and attenuated absorption of free fatty acids, thereby enhancing overall blood lipid profiles [21]. However, despite the commonality of i lipid level reductions following these procedures, the magnitude of reduction may vary contingent on the location and extent of gastric tissue resection. Notably, during sleeve gastrectomy, a substantial section of the fundus—the main location of gastrin secretion—and the stomach's larger curvature are removed [22]. Gastrin has been implicated in stimulating appetite, augmenting gastric motility, promoting growth hormone secretion, and inhibiting fat utilization. The removal of the fundus of the stomach also perturbs the release of intestinal hormones, including gastrin [23]. Conversely, oesophageal carcinoma resection targets a segment of the lesser curvature of the stomach, exerting a comparatively milder influence on intestinal hormones, consequently resulting in a lesser reduction in blood lipid levels.
In the dynamic analysis of lipid fluctuations among patients with oesophageal cancer and concurrent hyperlipidaemia at the one-year postoperative mark, a significant reduction in all lipid parameters was observed within the initial week following oesophageal cancer resection. This intriguing phenomenon can be attributed, in part, to the dietary shifts enforced during the postoperative period. Notably, at the institution, patients diagnosed with oesophageal cancer typically adhere to a regimen of fasting with water intake for approximately 5–7 days following surgery. Only after confirmation of the absence of critical complications, such as anastomotic fistula, are pacients permitted to initiate oral intake. In the initial phases of dietary reintroduction, most patients primarily adhere to a liquid diet. Furthermore, Jahansouz et al. reported that acute changes in the expression and activity of peroxisome proliferator-activated receptor delta (PPARδ) and gamma (PPARγ) in subcutaneous adipose tissue are caused by bariatric surgery. These changes correlate with a reduction in lipid storage, an increase in lipolysis, and an increase in lipid oxidation [24]. Correspondingly, the study revealed a transient decrease in serum TC and LDL levels in patients following oesophageal cancer resection. This could be linked to a similar mechanism.
In addition to dietary influences and the metabolic consequences of surgery, it is pertinent to consider the role of the surgical stress response. Surgical stimuli have been associated with increased cortisol and growth hormone release through the hypothalamic-pituitary axis, which, in turn, fosters lipolysis [25]. As time progresses, the effects of these factors on lipid profiles gradually wane or diminish, resulting in a gradual increase in lipid levels beginning one month postoperatively. Notably, TC and LDL levels peak at the six-month postoperative follow-up, albeit remaining significantly lower than the preoperative levels. Conversely, HDL levels reach their zenith at the one-year postoperative milestone, significantly surpassing preoperative levels. Intriguingly, there were no significant differences in TG levels between the first week and subsequent postoperative periods.
This finding is in contrast to that of a study by Magdalena Vila et al., who examined the lipid profiles of patients after pancreaticobiliary bypass. Their findings indicated a significant decrease in TC levels postsurgery, with a nadir being reached at one year postsurgery, followed by a gradual increase. Conversely, TG levels exhibited an increase from one month postoperatively to six months postoperatively, followed by a decrease, with a substantial decrease observed at one year postoperatively. HDL decreased at three months postsurgery, followed by a significant increase at the six months and one year postsurgery. LDL levels continued to decrease postoperatively, with the most pronounced reduction occurring at three months postoperatively. Discrepancies with the study's findings could be attributed to variances in the timing of follow-up assessments, with Magdalena Vila et al. commencing their postoperative evaluation at three months as opposed to the assessment at one week postoperatively in this study.
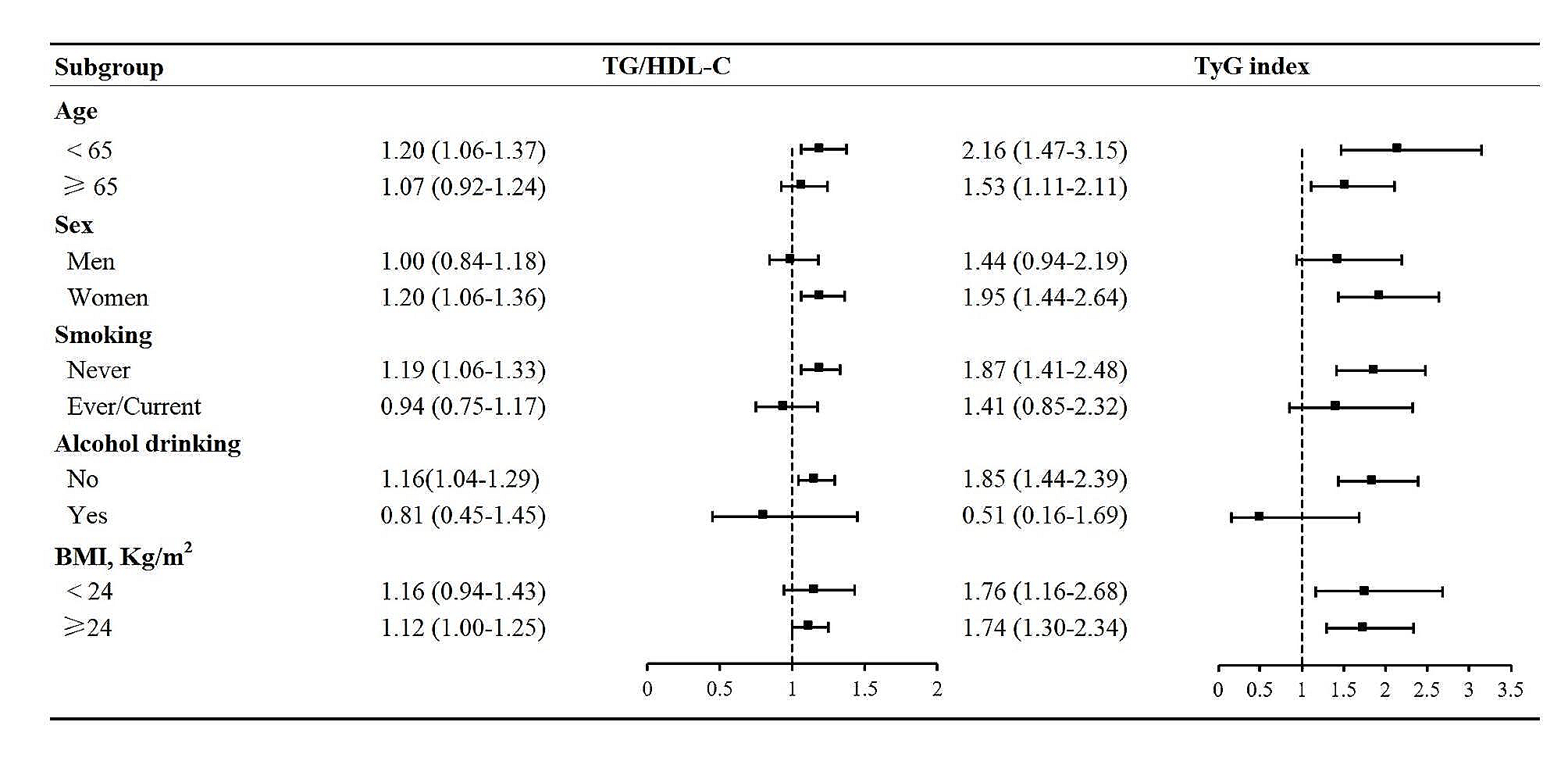
Numerous scholars have investigated the correlation between postoperative lipid alterations and weight loss after bariatric surgery. Dattilo AM et al. have posited that weight loss is closely linked with noteworthy reductions in TC (r = 0.32), LDL (r = 0.29), very-low-density lipoprotein (r = 0.38), and TG (r = 0.32) [26]. Researchers Aucott L et al. established a linear association, showing that cholesterol decreases by 1.3% and triglycerides decreased by 1.6% for each kilogram of weight reduction [27]. Regrettably, pertinent studies exploring the interface between lipid alterations and weight loss following oesophageal cancer resection are lacking. In this investigation, an attempt was made to bridge this knowledge gap by analysing the correlation of lipid fluctuations with changes in weight among patients who underwent oesophagectomy for oesophageal cancer. This findings revealed that alterations in TC, LDL, and non-HDL levels at one-year postoperative juncture were positively correlated with preoperative body weight and a negatively correlated with one-year postoperative weight loss. Conversely, TG fluctuations exhibited an inverse relationship with preoperative body weight and TWL% and a positive correlation with one-year postoperative weight loss. Similarly, regression analysis by L. N. Zhang et al. revealed a positive correlation between body weight changes and alterations in TC, LDL, and TG, along with a negative correlation with HDL fluctuations. Their findings implied that irrespective of baseline weight, weight loss confers benefits in terms of improving blood pressure, glucose profiles, and lipid parameters among middle-aged and older adults [28]. Furthermore,according to Busetto L et al., in morbidly obese people, slight weight loss—roughly 10–20% of starting body weight—has the greatest effect on lipid profiles [29]. This finding substantiates the close association between weight loss and lipid improvements. The underlying rationale for this association may be attributed to heightened utilization of lipid reserves within adipose tissue that involves fat consumption for energy and consequently reduction of blood lipid levels. Notably, this study further revealed that changes in the TG/HDL ratio were negatively correlated with preoperative body weight and TWL% but positively correlated with one-year postoperative weight loss. A possible early indicator of insulin resistance is the TG/HDL ratio. Recent investigations have suggested that caloric restriction prompts hepatic fat depletion within one week, subsequently enhancing hepatic insulin sensitivity and clearance, irrespective of whether metabolic surgery is performed [30, 31].
Following oesophagectomy, patients may encounter unintended reductions in weight and gastrointestinal complaints linked to inadequate nourishment and impaired functional recovery, even in the absence of long-term recurrence [32]. Furthermore, malnourished patients may develop sarcopenia and osteoporosis alongside weight loss [33]. The multifactorial causes of weight loss include tumour-related symptoms (e.g., dysphagia), metabolic abnormalities, treatment-related toxicity, and muscle atrophy due to patient inactivity [34]. Studies by Scarpa et al. and Wu et al. have demonstrated the enhancement of postoperative nutritional profiles, including loss of appetite and body mass index, through minimally invasive oesophagectomy [35, 36]. Postesophagectomy enteral nutrition commonly involves the use of a jejunostomy tube. Adequate nutritional support is essential for in preventing malnutrition in oesophagectomy patients, and enteral nutrition rich in eicosapentaenoic acid (EPA) has been shown to preserve lean body mass postesophagectomy [37]. Additionally, a study reported that an enteral diet rich in ω-3 fatty acids improved oxygenation post-thoracic oesophagectomy [38]. A walking-feeding intervention for patients with newly diagnosed locally advanced oesophageal cancer during neoadjuvant chemoradiation therapy initiation and completion effectively maintained patients' functional walking ability and nutritional status [39]. Nutritional interventions primarily focus on providing adequate calories and nutrients through additional supplements or educating patients to opt for a protein- and calorie-rich diet [40, 41]. Long-acting octreotide has been utilized for decades to reduce postprandial symptoms and induce weight gain in various clinical scenarios related to reducing body weight [42]. Surgical growth inhibitor analogues have also been employed to alleviate postprandial symptoms and may have a favourable impact on nutrition, improving the recovery of weight loss following surgery [43].
There are a few noteworthy strengths in this study. First, the study focused on patients with oesophageal cancer combined with hyperlipidaemia, a subject which has reveived less attention in existing scientific research. By studying the relationship between preoperative combined hyperlipidaemia and postoperative metabolic function, preoperative management and postoperative rehabilitation can be improved. Second, the comparison of lipid changes at different postoperative time points enhances the comprehensiveness of the findings and provides valuable insights into the dynamics of lipid parameters, contributing to a deeper understanding of the long-term effects of oesophageal cancer resection on lipids. In addition, the results of this study are not only applicable to patients with oesophageal cancer, but also might additionally serve as a resource for the management of allied illnesses. This study has certain limitations. First, 110 patients from a single medical facility constituted a numerically unremarkable but eligible sample used in the study's retrospective review. It is possible that some patients did not strictly follow the requirement of fasting for 10–12 h prior to the examination, possibly leading to bias and limited the generalizability of the results to the larger group of patients with combined hyperlipidaemia undergoing oesophagectomy for oesophageal cancer. Therefore, a large sample, multicentre study is necessary to validate the results. Second, this study had a limited follow-up period, and a longer-term assessment of metabolic markers and general health would help to provide a more thorough grasp of the effects of oesophageal cancer surgery on patients with hyperlipidaemia. Third, this study focused on metabolic changes after surgery and did not delve into specific dietary and lifestyle measures that affect patients' metabolic markers after surgery. Future studies could take specific nutritional and exercise interventions into account to explore their potential impact on patients' postoperative metabolic health.






留言 (0)