Estradiol valerate (E2V) is a derivative of estradiol (E2), a hormone naturally occurring in the human body, crafted to replicate the effects of E2 within the body. It is commonly prescribed to address hormone-related conditions. E2 is typically synthesized with an ester side chain, such as E2V, estradiol undecylate, estradiol benzoate, and estradiol cypionate. This is because endogenous E2, when taken orally, has minimal bioavailability (typically ranging from 2% to 10%) due to rapid degradation by first-pass metabolism in the gut and liver. Consequently, these ester side chain prodrugs of E2 serve to safeguard it from first-pass degradation, thereby allowing it to exert its estrogenic effects [1]. They enhance absorption, lipophilicity, and bioavailability post-administration and also facilitate sustained release from depot intramuscular injections [2,3].
E2V was initially employed for medical purposes in 1954 [4] and gained approval for hormone therapy and hormonal contraception in 2010 [4,5]. It stands out as one of the most frequently used estradiol esters and is endorsed in hormonal treatment guidelines [[6], [7], [8]]. E2V finds application in various medical contexts, including fertility suppression for contraception, inhibition of sex hormone production, estrogen deficiency supplementation, and treatment of conditions such as female gonadal dysfunction, atrophic vaginitis, vulva dryness, and menopausal syndrome [[9], [10], [11]]. Moreover, E2V is effective in treating cancers like metastatic breast cancer [12] and advanced androgen-dependent prostate cancer [13]. Recently, E2V has been made available in tablet form for oral intake (marketed as Progynova® and Primiwal E4®) and via intramuscular injection (sold as Delestrogen® and Progynon Depot®) [5]. Typically, oral administration of E2V leads to substantial first-pass hepatic metabolism, resulting in low drug potency and reduced bioavailability. Conversely, intramuscular injection and transdermal administration circumvent this metabolic pathway. Intramuscular administration of E2V ensures an extended duration of action due to the formation of an intramuscular depot, from which the medication is gradually released and absorbed. The reported duration of action varies; for instance, a 5-mg dose lasts 7–8 days, while a 100-mg dose provides efficacy for 21–28 days [14]. However, intramuscular injections come with drawbacks such as injection site pain, infection risks, and the need for trained personnel, thereby limiting their convenience and accessibility. Consequently, transdermal administration, considered a safe and convenient alternative, has been explored for E2V delivery.
Transdermal drug delivery presents an appealing alternative to oral intake, particularly when compared with hypodermic injections. This mode of therapy offers various advantages, such as avoiding first-pass metabolism, being painless, and enabling self-administration [15]. Moreover, transdermal formulations can be tailored for controlled release of drugs over an extended duration to enhance patient compliance. Furthermore, they can be easily removed on upon necessity, such as in cases of adverse effects or treatment discontinuation is warranted [16]. However, the efficacy of transdermal drug delivery is impeded by the stratum corneum, the outermost layer of the skin, which serves as a physical barrier, leading to reduced drug bioavailability and delivery efficiency [17]. To surmount this obstacle, both passive enhancement techniques [18] (such as optimizing formulation, reducing drug particle size, and using chemical enhancers) and active enhancement methods [19] (including sonophoresis, iontophoresis, and microneedles) can be employed to augment transdermal drug delivery.
E2V exhibits poor solubility in water, classified as “practically insoluble” according to the solubility classification from the United States Pharmacopoeia and European Pharmacopoeia [20], with a log octanol/water partition coefficient (Log P) of 6.62 [21]. However, it demonstrates high solubility in various oils [20], posing challenges in formulating pharmaceutical preparations for transdermal drug delivery. Nanoemulsion (NEs), a lipid-based system, offer a novel formulation approach to enahnce the solubility of poorly water-soluble drugs. NEs are colloidal dispersion systems consisting of two immiscible phases: oil and water, stabilized by emulsifying agents (surfactants and cosurfactants), with droplets typically ranging from 10 nm to 1000 nm in diameter [22]. NEs exhibit optical isotropy and kinetic stability, often produced using high-energy methods. NEs have been extensively employed orally to improve the solubility and bioavailability of lipophilic drugs. Their advantages as drug carriers, particularly for lipophilic drugs, include high stability, enhanced drug solubility, improved bioavailability, and high loading capacity [23]. Moreover, they offer protection against hydrolysis and oxidation of drugs or bioactivities [24]. However, their application in topicals is limited by challenges such as low viscosity and high spreadability, leading to difficulties in controlling drug dosing [25]. The combination of micro-/nanodrugs in microneedles (MNs), a novel drug delivery technology, has garnered increasing interest in pharmaceutical fields, including nanosuspensions [26,27], nanomicelles [28], polymeric nanoparticles [29], and solid lipid nanoparticles [30]. Yet, research on loading of NEs or lipid-based systems into innovative microtechnology dosage forms like MNs, which offer controlled drug dosing and release, remains limited. Examples include amphotericin B nanoemulsions [31], progesterone microemulsions [32], fluconazole microemulsions [32,33], collagenase emulsions [34], and lidocaine liposomes [35]. Therefore, enhancing the solubility of E2V using NEs represents a valuable objective for effectively incorporating them into MN dosage forms for controlled transdermal drug delivery.
MNs represent a compelling advancement in microtechnology, characterized by micron-scale dimensions, typically falling within the range of 25–1000 μm [36]. They serve to create microchannels within the stratum corneum barrier, facilitating transdermal drug delivery. MNs holds significant appeal due to their minimally invasive nature, painlessness, lack of biohazard, generation of nonsharp waste, potential for self-administration by patients, enhanced bioavailability, and ability to enable sustained drug release [37,38]. Among various types of MNs (including solid MNs, coated MNs, hollow MNs, and hydrogel MNs) dissolving microneedles (dMNs) are widely utilized. This preference arises because dMNs completely dissolve into the skin within a desirable timeframe, leaving no hazardous sharp waste behind [39]. Typically, dMNs are crafted from biodegradable polymers known to be safe and nonirritating upon application to the skin, such as polyvinylpyrrolidone (PVP), polyvinyl alcohol (PVA), poly(methyl vinyl ether/maleic acid) (Gantrez™), and polymethacrylate (Eudragit®) [40,41]. However, loading lipophilic drugs into dMNs presents a considerable challenge due to the immiscibility between the aqueous polymeric phase of dMNs and the lipophilic phase of drugs. This mismatch can lead to issues concerning content uniformity, completeness of MN dissolution, and properties such as mechanical strength and insertion capability. Consequently, core-shell dissolving microneedles (CS-dMNs) have been developed to address these limitations [42]. Typically, the core of CS-dMNs, intended for sustained drug release, is fabricated using polymers such as polycaprolactone (PCL), polylactic acid (PLA), or poly(lactic-co-glycolic acid) (PLGA) [43]. By encapsulating the lipophilic phase of drugs within the core of CS-dMNs, these devices enable slow drug release, detachment of needles from the patch backing, and retention of the core within the skin. Recent advancements have led to techniques facilitating the rapid separation of needle tips from MN patches to sustain drug release. This techniques include core-shell structures [42], air bubble incorporation [44], effervescent formulations [17,45], and high porosity designs [46]. As a result, developed CS-dMNs can be self-administered by patients, with the core embedding into the skin promptly and sustaining drug release over an extended duration.
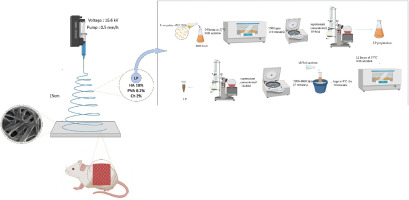
This study introduces a novel approach for self-administration of E2V-NE-loaded CS-dMNs, aiming at controlled release transdermal drug delivery. Initially, a computational design was utilized to optimize the size, PDI, and zeta potential of the E2V-NE formulations. Following this, E2V-NEs were incorporated into CS-dMNs using a micromolding technique. The design of the CS-dMN shell was further refined through computational strategies. Subsequently, the resultant optimal E2V-NE-loaded CS-dMNs underwent comprehensive evaluation, encompassing assessments of their physical appearance, mechanical strength, ex vivo insertion characteristics, drug loading efficiency, patch detachability, needle embedding in the skin, as well as ex vivo and in vivo skin permeation, and deposition of the drug in the skin.



留言 (0)