
記住我



A 21-year-old man was admitted to our hospital due to the poor control of left eye’s IOP. Diagnosed with aniridic glaucoma, he had been given topical anti-glaucoma medications to control IOP since the age of one. Three years ago, he underwent goniotomy surgery of the left eye due to the failure of medical therapy, which was a combination of brinzolamide/timolol (AZARGA®, Alcon®, Vernier, Switzerland), latanoprost (XALATAN®, Pfizer, New York City, USA), brimonidine (ALPHAGAN®, Allergan, Dubin, Ireland) and pilocarpine (Bausch & Lomb, Shandong, China). The surgery was accomplished with the help of direct gonioscopy, and the range of goniotomy was 8 ~ 12 o’clock. The IOP was maintained between 16 ~ 20 mmHg after the surgery. He was regularly followed up, and the IOP raised again a month ago. The patient’s best corrected visual acuity was 0.8 OD and 1.0 OS (logMAR). The IOP measured by hand-held rebound tonometry (iCare TA01i tonometer, Vantaa, Finland) was 20 mmHg OD and 26 mmHg OS with brinzolamide/timolol, latanoprost and brimonidine for both eyes. Horizontal nystagmus was present (OU). Slit-lamp examination (OU) showed corneal conjunctivalization and vascularization. The central cornea was opaque and thickened, reflecting a Grade 4 aniridia-associated keratopathy [4]. The majority of iris tissue was absent with peripheral stump remaining, and posterior subcapsular cataract was present. The gonioscopy demonstrated that 360° anterior chamber angle was closed. Fundus examination showed pallor of optic disc (OS). The cup-to-disc ratio was 0.6 OD and 0.8 OS. Foveal reflex was absent, and retinal vessels were seen traversing the expected foveal area (OU) reflecting foveal hypoplasia (Figs. 1 and 2). The patient received cryptorchidism surgery in his childhood. The family history was unremarkable. The computerized tomography urogram demonstrated atrophy of partial renal parenchyma. The whole exome sequencing of peripheral blood confirmed a 13.39 Mb copy number loss at chromosome 11p15.1p13, in which contains PAX6 and WT1 gene (Fig. 3).
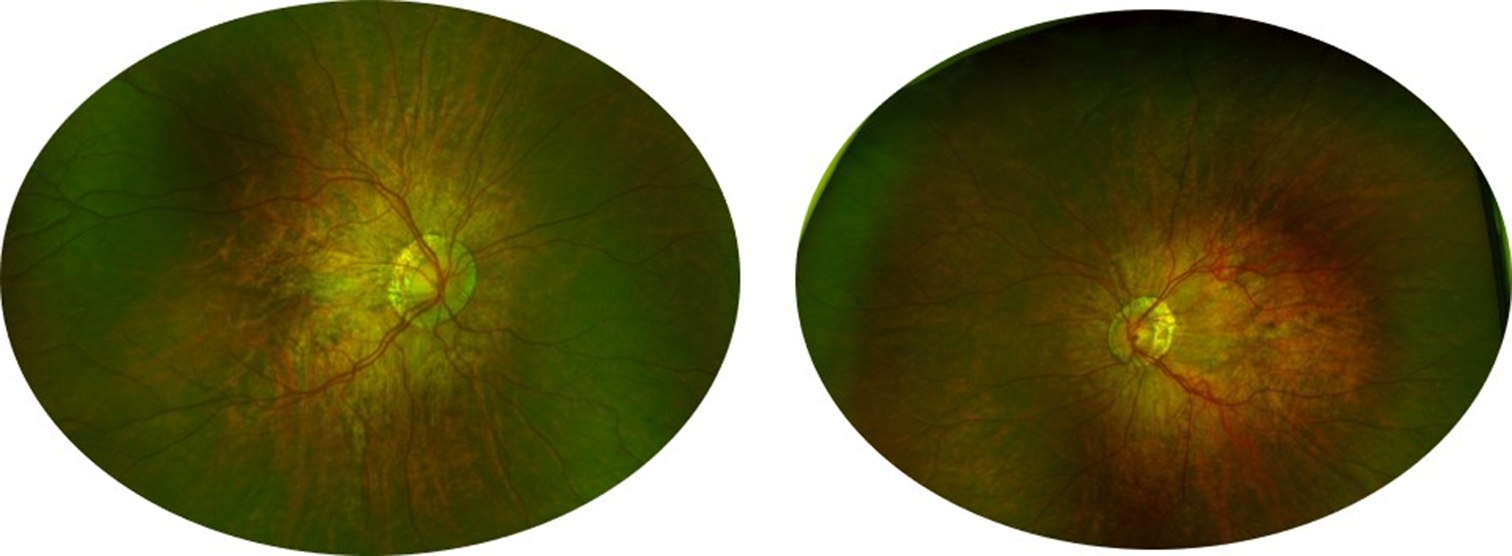
Fig. 1
Preoperative examinations of the right eye. A The anterior segment photo showed aniridia-associated keratopathy. B The fundus photo showed hypoplasia of optic disc and fovea. C The static perimetry showed diffuse defect of visual field. D The ultrasound biomicroscopy showed the absence of iris tissue and closure of anterior chamber angle
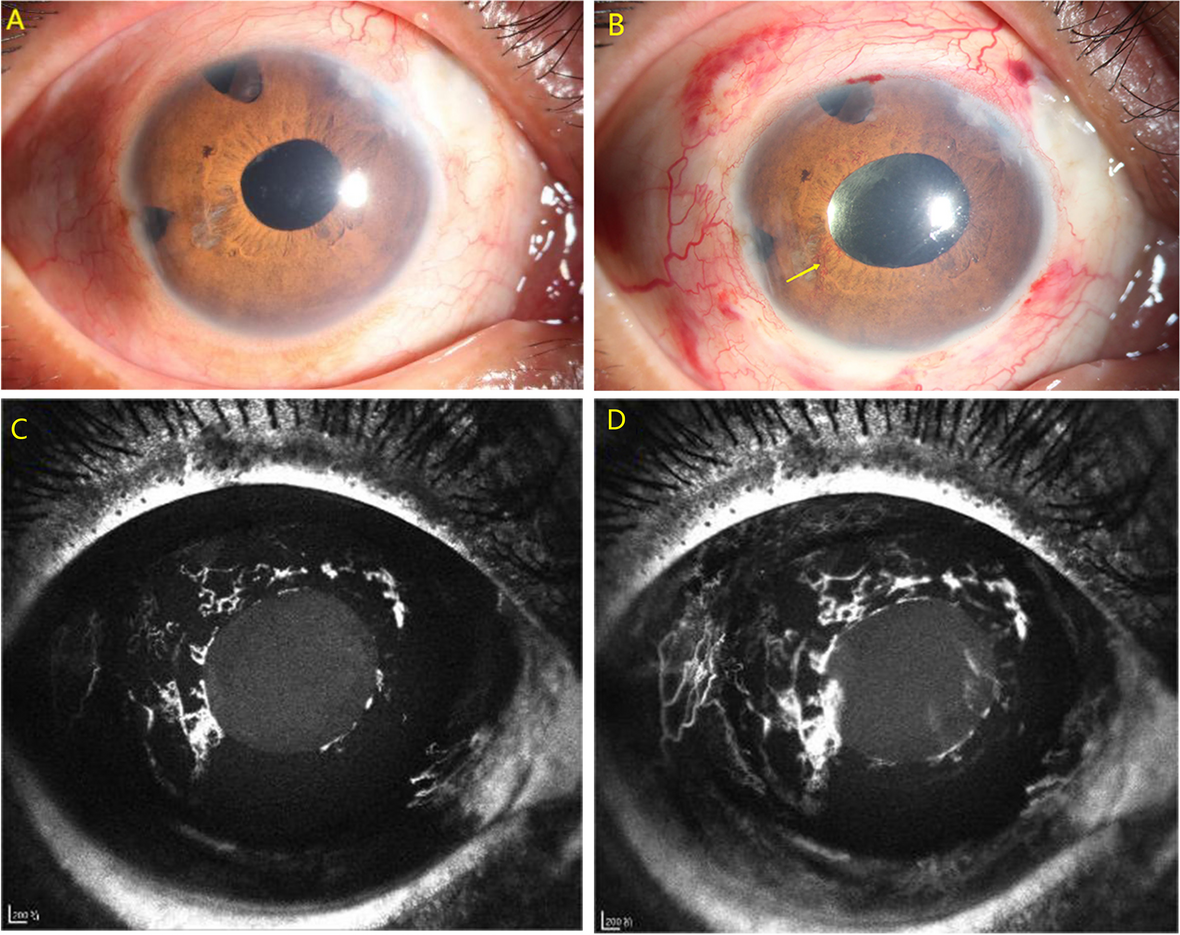
Fig. 2
Preoperative examinations of the left eye. A The anterior segment photo showed aniridia-associated keratopathy. B The fundus photo showed hypoplasia of optic disc and fovea. C The static perimetry showed diffuse defect of visual field. D The ultrasound biomicroscopy showed the absence of iris tissue and closure of anterior chamber angle
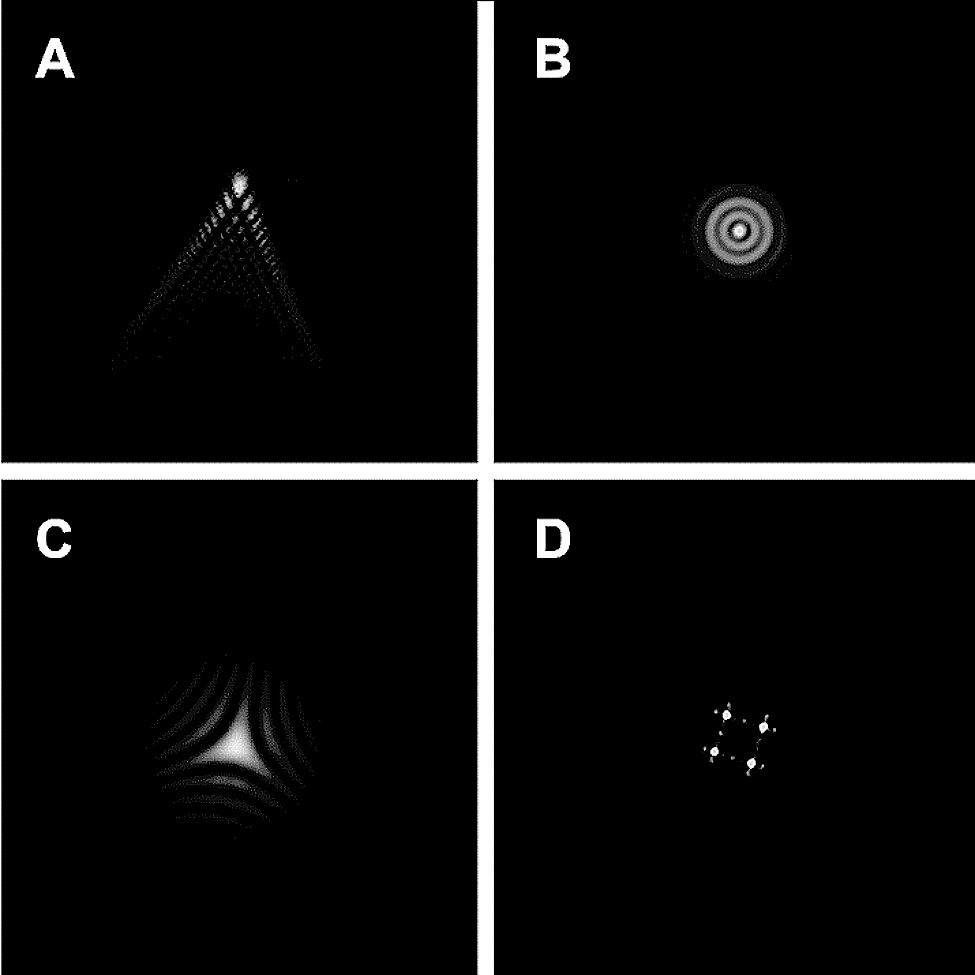
Fig. 3
Preoperative examinations of the kidneys and the whole exome sequencing of peripheral blood. A The B-scan showed hypoplasia of the right kidney. B The B-scan showed a normal left kidney. C and D The computerized tomography urogram showed hypoplasia of the right kidney and a normal left kidney. E The whole exome sequencing of peripheral blood confirmed a 13.39 Mb copy number loss at chromosome 11p15.1p13
The surgery was performed on the left eye under general anesthesia. Briefly, A fornix-based conjunctival flap was made at 12 o’clock. A 5 \(\times\) 4 \(\times\) 3-mm trapezoid superficial scleral flap was made at the same location followed by creation of a 2 \(\times\) 2-mm deep scleral flap to search for the external wall of the Schlemm canal. Paracentesis was made and viscoelastic was injected into the anterior chamber. A microcatheter (iTrack™, Nova Eye Medical Limited, Kent Town, Australia) was introduced via a breach of the Schlemm canal, and it passed through the Schlemm canal under the guidance of indicator at the tip of the microcatheter. 360° trabeculotomy was accomplished by pulling the two ends of the catheter. 10 − 0 nylon sutures were used to close the scleral flap and conjunctival flap. The anterior chamber was then irrigated from the paracentesis, followed by stromal hydration for corneal incision sealing. The intraoperative pictures and the image of iTrack™ are shown in Fig. 4. After the surgery, levofloxacin eyedrop QID (Cravit®, Santen, Osaka, Japan) and prednisolone acetate eyedrop QID (Pred Forte®, Allergan, AbbVie Inc., North Chicago, IL, USA) were given for 1 month, and pilocarpine eyedrop QN was given for 3 months.
Fig. 4
Intraoperative pictures and the image of iTrack™. A The scleral flap was made at 12 o’clock. B The microcatheter passed through the Schlemm canal circumferentially and came out from the initial breach (red dashed line). Green arrow: the iTrack™ microcatheter. Blue arrow: traction suture. Orange arrow: cotton. Red star: cornea. C The appearance of iTrack™
At the first postoperative day examination, the IOP decreased to 10 mmHg, and Grade II hyphema was presented. Anterior segment optical coherence tomography (AS-OCT) showed successful incision of the Schlemm canal (Fig. 5).
Fig. 5
Postoperative examinations of the left eye. A Anterior segment optical coherence tomography 1-day postoperatively. B Anterior segment optical coherence tomography 1-year postoperatively. C The ultrasound biomicroscopy 1-year postoperatively. The arrowheads demonstrated the successful incision of the Schlemm canal. D The anterior segment photo was similar to that of preoperatively
At 6-month follow-up, the VA of left eye was 0.9 (logMAR) and the IOP was 22mmHg with topical brinzolamide/timolol BID.
One year post MAT surgery, the VA of left eye was 0.9 (logMAR) and the IOP was 19mmHg with topical latanoprost/timolol QN (XALACOM®, Pfizer, New York City, USA). The AS-OCT showed that the trabecular meshwork was still incised on the temporal side. The nasal iris stump adhered anteriorly with the angle wall (Fig. 5).
Discussion and conclusionsAccording to the study of Gramer et al., congenital glaucoma is rare in aniridia patients, and the onset of glaucoma occurs in adolescence and early adulthood most [13]. Therefore, the monitoring of glaucoma should have been sustained since the diagnosis of aniridia. Surgery is often necessary to treat aniridic glaucoma. Different advocations about the methods of surgery reveal the refractoriness of aniridic glaucoma.
Various surgical procedures, including goniosurgeries, trabeculectomy, glaucoma drainage implants and cyclodestructive procedures, have been reported in previous researches. Goniosurgeries, including goniotomy and trabeculotomy, are the most reported approaches. The success rate of goniotomy varied in previous studies depending on the timing of intervention. Prophylactic goniotomy showed far better prognosis compared with therapeutic one [1]. Adachi et al. summarized 12 aniridic glaucoma eyes receiving trabeculotomy, and the results showed that 10 eyes received good IOP control with an average follow-up of 9.5 years. Thus, they suggested that trabeculotomy should be adopted as an initial method [12]. On the contrary, trabeculectomy demonstrates limited success rate. The study of Durai et al. revealed that the cumulative probability of failure was 58.3% in the trabeculectomy group at 2 years [14], and Wiggins et al. reported a success rate of only 7% receiving trabeculectomy [15]. Glaucoma drainage implant is another option. Almousa et al. implanted the Ahmed glaucoma valve for 8 aniridic glaucoma eyes, and 7 eyes received good IOP control [16]. Wiggins et al. also reported successful outcomes of glaucoma drainage implant in advanced patients who had already received prior glaucoma surgeries [15]. Although the efficacy of IOP control is good, complications related to implants, e.g., tube exposure, tube obstruction and corneal endothelial damage, may still occur in a high incidence [15,16,17]. Therefore, it may be better to preserve glaucoma drainage implants as a remedial procedure. Though cyclodestructive procedures are effective in controlling IOP, they often cause serious complications including hypopsia, cataract, retinal detachment and phthisis bulbi [15, 18, 19]. It may be unsuitable to select cyclodestructive surgery as an initial surgical choice to treat aniridic glaucoma patients who remain poor vision. The clinical information of prior studies is demonstrated in Table 1. In summary, prophylactic goniotomy provides good outcome in patients whose angle is open in early stage. However, surgical interventions demonstrate either limited efficacy or high incidence of postoperative complications in advanced patients. A new surgical approach is needed urgently for aniridic glaucoma patients following failed previous surgery.
Table 1 Summary of previous studies and current study on aniridic glaucoma patients treated with various surgical proceduresTo the best of our knowledge, this case is unique in its first use of MAT for treating aniridic glaucoma. Our patient received goniotomy previously, but failed to control the IOP after 3 years. The result is in accordance with previous reports [1, 7]. We attempt to figure out a better approach with higher success rate and fewer complications. Adachi et al. advocated that abnormality of Schlemm canal, which was similar to congenital glaucoma, was a mechanism of aniridic glaucoma [12]. In several recent literatures, MAT showed satisfied results in patients with congenital glaucoma, and many of these cases possessed cloudy corneas. In these researches, the criteria of success were defined as IOP ≤ 21 mm Hg with or without antiglaucoma medications. The success rate reached 88% and no severe complications were observed [9, 21, 22]. Therefore, these researches provide theoretical basis for us to use MAT to treat aniridic glaucoma. The advantage of circumferential trabeculotomy is the ability to maximize the IOP-reducing effect by treating the whole anterior chamber angle in a single surgery. The illuminated catheter tip also enables us to see the location directly across the sclera without the need of direct gonioscopy which may need a certain extent of corneal clarity. The postoperative IOP remains stable generally with topical medications within 1 year in our patient. The application of MAT in the treatment of aniridic glaucoma may be regarded as qualified successful. Compared with goniotomy which shows higher success rate in younger patients who have not developed glaucoma yet, MAT may be a potential option for treating aniridic glaucoma patient who is older and has experienced a previously failed surgery.
In conclusion, we exhibited a possible surgical approach to manage PAX6 aniridic glaucoma. However, further studies are needed to evaluate the efficacy and safety of MAT on aniridic glaucoma with more cases and longer follow-up period.
留言 (0)