
記住我



Retinal vascular density is a quantitative measurement that describes the concentration or number of blood vessels within a specific area of the retina. It provides information about the health of the retinal vascular system. A higher VD indicates a greater number of blood vessels within the measured area, while a lower density suggests fewer vessels.
The study found that total vascular density decreased significantly in group 2 with severe ICA stenosis and longer duration of diabetes. Previous studies [7, 8] have suggested that severe ICA stenosis with DM can lead to reduced blood flow to the optic nerve head and retina, which may cause ischemia and subsequent vascular changes. Our findings support the existing evidence that suggests a correlation between ICA stenosis and vascular density in patients with proliferative diabetic retinopathy [7].
Increased FAZ areaThe foveal avascular zone is a small, circular area in the center of the retina known as the fovea. The FAZ is called avascular because it lacks the typical network of blood vessels that are present in other parts of the retina. In healthy eyes, the FAZ is relatively small and well-defined. However, certain eye conditions or disease can cause changes in the FAZ such may involve an enlargement or disruption of the FAZ area, which can affect central vision and lead to visual impairments.
The study observed a statistically significant increase in FAZ area among participants in group 2. The findings of this study are consistent with previous research suggesting that in patients with DM, the FAZ area increases with severe ICA stenosis [8, 9]. This could be attributed to reduced blood flow to the retina leading to ischemia, as suggested by Conrath J [10]. Additionally, Kikushima W. proposed that the size of the FAZ area could serve as a marker for the degree of ICA stenosis [11].
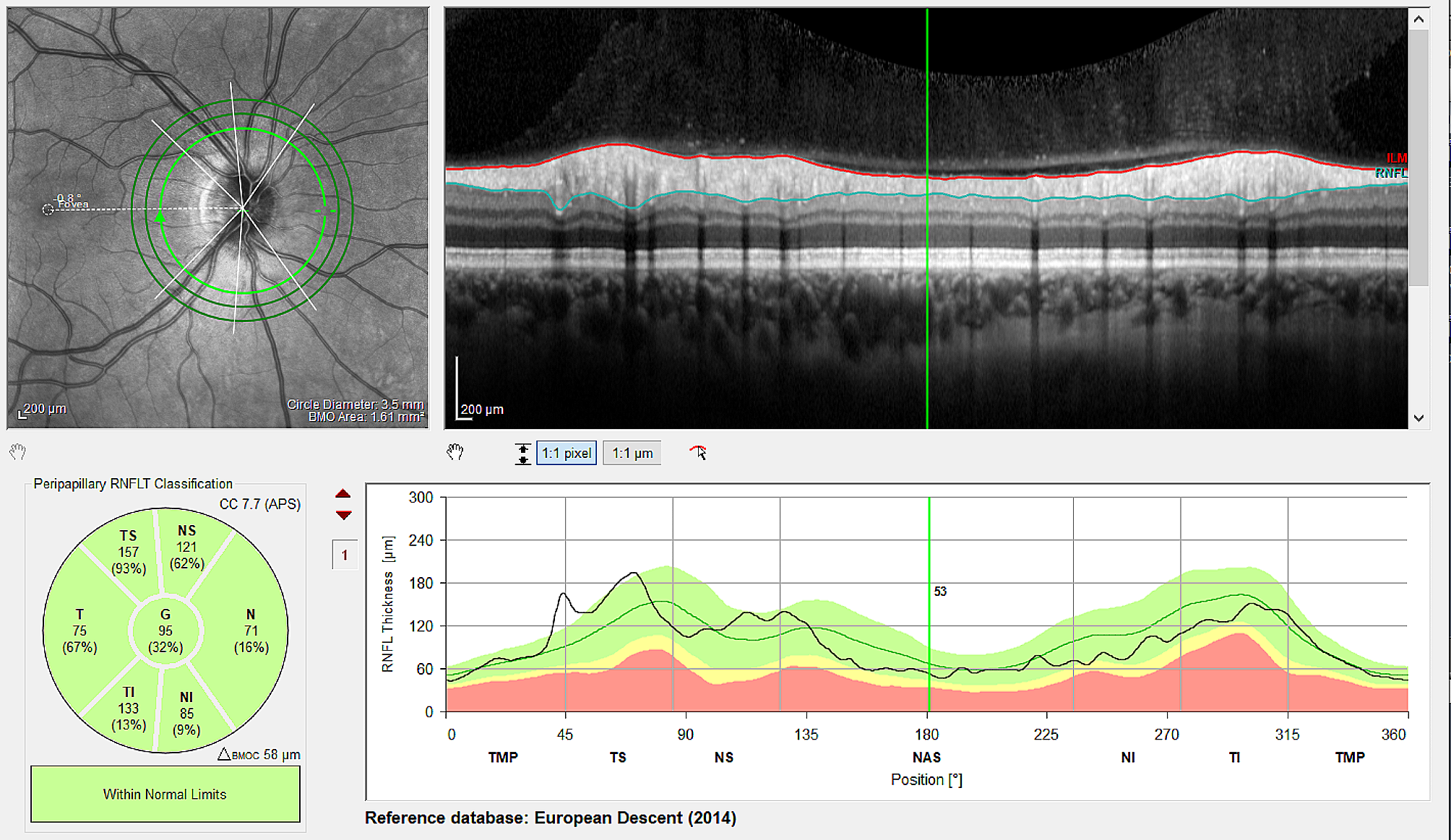
Decreased total RNFL thickness / temporal RNFL thicknessThe retinal nerve fiber layer is a thin layer of nerve fibers that lines the inner surface of the retina, which is the light-sensitive tissue at the back of the eye. The RNFL is made up of the axons of ganglion cells, which are the specialized cells responsible for transmitting visual signals from the retina to the brain. RNFL can divided into different regions based on their anatomical location in the eye. The four main regions are superior, inferior, nasal, temporal as shown in Fig. 5.
Fig. 5
Report sample of the measurement of the retinal nerve fiber layer (RNFL) with OCT. (A) The four main regions of the RNFL. (B) RNFL thickness of four regions
The RNFL thickness showed statistically significant thinning in group 2 with severe ICA stenosis, especially in the temporal region, with group 1 showing a significant decrease to 82.46 ± 27.75 μm and group 2 to 71.75 ± 20.19 μm (p = 0.019). Studies have proposed that the mechanism underlying the relationship between ICA stenosis and RNFL thickness reduction may be attributed to a reduction in blood supply to the retina and choroid caused by carotid artery changes, which subsequently results in a decreased thickness of the retinal nerve fiber layer supplied by the central retinal artery and posterior ciliary artery [12, 13].
According to Oage G., the RNFL is highly susceptible to ischemia because it is supplied by end arteries with limited collateral blood flow capacity. This renders the RNFL particularly vulnerable to any reduction in blood supply, underscoring the significance of maintaining adequate perfusion to this region of the retina [14]. Specially, the papillomacular bundle(PMB) and the temporal RNFL have a tightly interconnected structure and function [13, 14]. Impairment of the temporal RNFL can impact the PMB’s function, resulting in reduced central visual acuity.
ICA stenosis is associated with elevated oxidative stress, which is characterized by an imbalance between reactive oxygen species production and neutralization [15]. Also, oxidative stress has been suggested to contribute to the loss of retinal ganglion cells(RGCs), which could lead to thinning of the RNFL, including the temporal region. Studies have shown that increased oxidative stress in the retina can lead to damage of RGCs and axons, which can result in thinning of the RNFL, including the temporal region [16]. A study showed that treatment with N-acetylcysteine (an antioxidant) improved the thickness of the temporal RNFL in patients with mild impairment. This suggests that oxidative stress may be involved in the loss of temporal RNFL thickness in these patients [17].
The observed association with ICA stenosis and the link to blood flow alterations imply that monitoring RNFL thickness could offer valuable insights into the vascular health of individuals with CAS. Clinically integrating RNFL thickness assessments may provide an additional dimension for risk assessment, prompting consideration for early interventions to mitigate the risk of adverse cerebrovascular events. Despite acknowledged study limitations, the findings underscore the potential of RNFL thickness as a clinically relevant biomarker, calling for further well-planned, large-scale prospective studies to validate its significance in guiding interventions for individuals with carotid artery stenosis and ultimately improving patient outcomes.
Decrease in IOPOur study observed a statistically decrease in IOP among participants in group 2. This result can be explained by CAS, which can affect blood flow to the ciliary body. This may result in high oxidative stress, leading to reduced aqueous humor production and subsequently resulting in normal or low IOP.
In a recent study by Jones et al., it was found that patients with ICA stenosis had significantly lower IOP compared to controls, supporting the idea that reduced aqueous humor production can lead to lower IOP [18]. Moreover, oxidative stress has been identified as a potential contributor to decreased aqueous humor production in patients with CAS. In an experimental study by Nakamura et al., it was found that oxidative stress induced by H2O2 led to a reduction in aqueous humor production in cultured rabbit ciliary processes [19].
However, some studies have suggested that elevated IOP may be associated with an increased risk of ICA stenosis [20]. Conversely, other studies have found no significant association between IOP and the prevalence or severity of ICA stenosis [21].
Relationships with total-C, hyperlipidemia and ageContrary to our initial expectations, our study revealed a statistically lower total -C level in patients with ICA stenosis. Although the traditional risk factors for ICA stenosis, such as hypertension and smoking, have been extensively studied, the association between cholesterol and ICA stenosis remains unclear. Our study results show similar results with previous studies. In a study by Singh et al. [22], the presence of hyperlipidemia was found to be a significant predictor of ICA stenosis in patients with carotid artery disease. Similarly, a meta-analysis by Mathiesen et al. [23] demonstrated a strong positive association between total -C levels and the risk of CAS.
ICA stenosis is a common manifestation of atherosclerosis, a disease that affects the arterial walls and is characterized by the formation of plaque [24]. Atherosclerosis develops slowly over time and is influenced by various risk factors, including age, total cholesterol levels, and hyperlipidemia [25]. Advancing age is a well-established risk factor for the development of atherosclerosis and ICA stenosis [26]. With aging, lipid-rich plaque buildup in arterial walls with age increases stenosis risk, and high cholesterol levels and hyperlipidemia can promote lipid-rich plaque formation and atherosclerosis [27, 28].
Overall, our findings suggest that the relationship between cholesterol and ICA stenosis is complex and warrants further investigation. It is possible that the lower total-C levels observed in our study were a result of medication use or other factors, rather than a causal relationship with ICA stenosis. However, there is some evidence to suggest that cholesterol-lowering medications, such as statins, may have a protective effect against the development of ICA stenosis. In a meta-analysis of randomized controlled trials, Zhang et al. found that statin therapy was associated with a significant reduction in the incidence of CAS, particularly in patients with hypercholesterolemia [29].
Understanding and addressing the concomitant effects of PDR and ICA stenosis is paramount for ensuring optimal patient outcomes. The synergistic interplay between ICA stenosis and PDR exacerbates the potential for retinal and choroidal blood supply deficiencies, accelerating retinal changes. As the retina acts as a window to systemic vascular health, its alterations can reflect broader systemic vascular issues, of which ICA stenosis is a key contributor. Enhanced management strategies targeting both conditions concurrently can mitigate complications, offer patients a more comprehensive treatment approach, and potentially improve both ocular and systemic health outcomes. Recognizing the intertwined nature of these conditions paves the way for more holistic, patient-centered interventions that can revolutionize the care paradigm for those suffering from both PDR and ICA stenosis.
Prudent interpretation of these findings is advised due to the limitations outlined below. Firstly, the study had a relatively small number of patients, which could limit the generalizability of the findings to a larger population. Secondly, the study design is cross-sectional and retrospective, which may limit the ability to establish causality and infer changes over time. Given that this study was retrospective in nature, further prospective or longitudinal research is necessary to support the recommendation for carotid evaluation in patients with bilateral PDR. Thirdly, we did not compare changes in the carotid artery in the absence of RNFL defects, which could provide more insight into the relationship between CAS and retinal changes.
The findings of this study suggest that changes in retinal and choroidal blood supply due to carotid artery changes may be the mechanism by which RNFL thickness reduction is related to ICA stenosis. However, it should be noted that this study had a small sample size and was limited to a cross-sectional retrospective design, making it difficult to confirm changes in the RNFL. Moreover, the cohort study failed to compare changes in the carotid artery in the absence of RNFL defects.
Lastly, while fundus fluorescein angiography (FFA) is a valuable tool for confirming the proliferative phase of PDR, the retrospective design of our study limited our access to complete FFA data for all included patients. In our study, proactive treatments such as panretinal photocoagulation (PRP) or vitrectomy were administered to patients with severe PDR before conducting FFA examinations. Subsequently, post-treatment FFA imaging was performed. The substantial improvement in clinical features, resulting from these initial treatments, led to minimal disparity observed in FFA findings between the eyes. Consequently, we decided to exclude these cases from the study at the outset, introducing certain limitations to our research. Moving forward, future prospective studies should incorporate FFA results for a more robust and definitive confirmation of PDR stages.
留言 (0)