
記住我

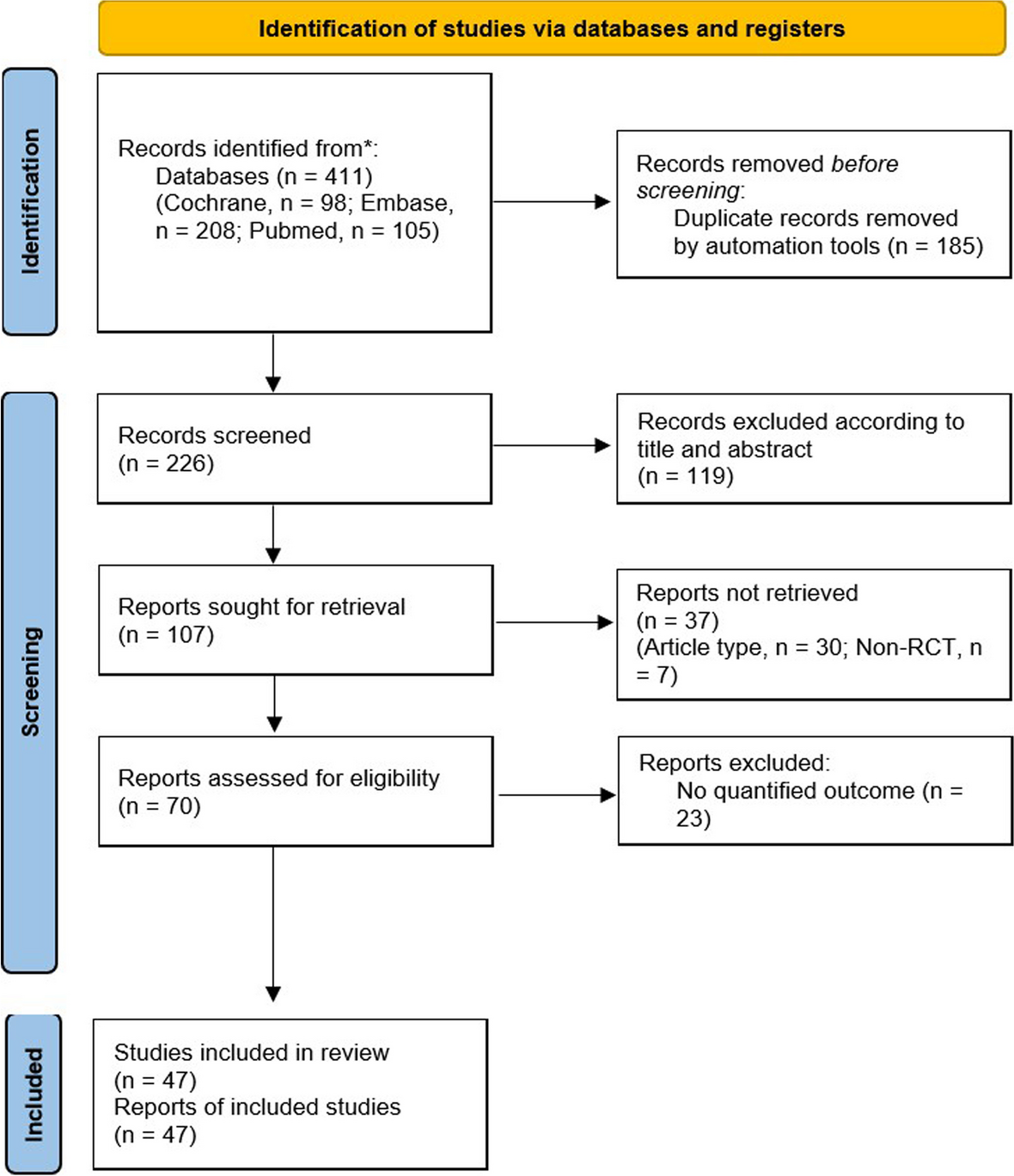






We retrospectively screened the records of 328 patients who underwent end-to-end urethral anastomosis at our hospital between January 2020 and December 2022 and selected 91 recurrent patients for inclusion in this study (Fig. 1). We selected patients with a 2–4-cm-long membranous urethral defect on urethrography that developed after a pelvic fracture who underwent suprapubic cystostomy at least 1 month before the operation. We excluded patients with a bladder neck injury (n = 17), urethral fistula (n = 27), accompanying anterior urethral stricture (n = 56), penile transposition urethral anastomosis (n = 8), graft replacement urethral anastomosis (n = 48), or incomplete follow-up (n = 81). The preoperative evaluation included age, time of injury, number and method of previous operations, physical examination, routine urine examination, urine culture, urinary flow rate, urethrogram, and urethroscopy. The patients underwent surgery 3 months after the pelvic fracture and had a lack of bacterial growth in urine cultures. Preoperatively, the suprapubic tube was replaced, and a urine culture was performed daily. Prophylactic antibiotics were administered according to drug sensitivity test results. The bladder was irrigated twice a day with 1,000 mL of 0.9% saline mixed with 5 mL of povidone-iodine. Surgery was performed after a negative urine culture result was returned. The patient was admitted to the hospital on the day of surgery.
Fig. 1
Retrospective chart review for inclusion and exclusion of cases
Surgical techniquesThe patients were administered general anesthesia and placed in the lithotomy position. An inverted Y-shaped incision was made in the perineum, and the bulbous urethra was separated to free the distal and proximal ends. Then, the distal end was freed to the level below the scrotum and transected at the disrupted site of the membranous urethra. The scar tissue was removed to expose the mucosa on both ends of the anastomoses. Then, the vertical and horizontal urethral defect lengths were measured. The extension line of the distal urethra is the Y line, the extension line of the proximal urethra is the X line. The reference point is the end of distal urethra and the proximal urethra. The vertical distance is from the distal reference point to the X line. The horizontal distance is from the proximal reference point to the Y line. For patients with long defect and high tension, 6 ancillary maneuvers were performed successively (Video 1).
Cavernous septum splitting (Fig. 2A): An electric scalpel was used to incise the septum of the penile cavernous body along the middle of the junction. The depth of the septal cut reached the lower edge of the pubis. The distal urethra was embedded into the penile cavernous septum after anastomosis.
Fig. 2
Ancillary maneuvers. A: penile cavernous septum incision; B: resection of the lower margin of the symphysis pubis; C: distal urethra mobilization; D: transposition of the anterior urethra at the foot of the cavernosum; E: folding of the penile cavernous body; F: urethral spongiform suspension
Inferior pubectomy (Fig. 2B): An electric scalpel was used to incise the periosteum to the lower edge of the pubic symphysis. Then, a wedge-shaped section of the bone was removed with a bottom width and height of 1.5–2.0 cm to create a direct urethral anastomosis with an osteotome.
Urethral mobilization to the penile-scrotal junction (Fig. 2C): Urethral tension was assessed by pulling the distal urethra to meet the proximal urethra. In the case of significant tension in the distal urethra, the urethra was freed to the penile-scrotal junction.
Rerouting of the anterior urethra (Fig. 2D): A channel was created to allow the anterior urethra to cross the tissue surrounding the bifurcation of the corpus cavernosum. Then, the anterior urethra was translocated to the lower edge of the corpus cavernosum to create a tension-free anastomosis with the posterior urethra.
Corpus cavernosa folding (Fig. 2E): This technique affects erectile function and should be avoided in patients who prefer to retain sexual function.
Urethral cavernous tissue suspension (Fig. 2F): Urethral tension after anastomosis was reduced by applying sutures to connect the two sides of the urethral cavernous tissue and the albuginea of the corpus cavernosum. The suture was placed on the corpus cavernosum 0.5 cm below that on the urethral cavernous tissue.
An F16 urinary catheter remained in place for 4 weeks after the operation, and the cystostomy tube was removed 3 weeks after normal urination resumed. Urine flow rate and urethroscopy were performed postoperatively.
Follow-upThe postoperative data included recurrence of the stricture and time of recurrence. In the case of urinary incontinence, the method used to treat the incontinence was recorded. Letters, emails, medical software, and the social media application WeChat were used to record postoperative urine flow rates and complete self-report questionnaires, PROM (USS-PROM). Surgical failure was evaluated using the annual Qmax, which required a uroflow voided volume of at least 200 mL. For patients with a Qmax less than 15 mL/s, follow-up cystoscopy was performed. Failure of passage of an F16 flexible cystoscope was used to indicate stricture recurrence. The International Index of Erectile Function (IIEF) was used to evaluate sexual function before and after surgery, with scores less than 21 indicating erectile dysfunction (ED).
Statistical analysisSPSS software (version 22.0; IBM Corp., Armonk, NY, USA) was used for statistical analysis. The baseline characteristics were analyzed using descriptive statistics and are presented as numbers and percentages. The chi-square and Fisher’s exact tests were used to compare data. P values < 0.05 were considered to indicate statistical significance.
留言 (0)