
記住我





Crohn's disease (CD) is a chronic inflammatory disease with unknown etiology that destroys the gastrointestinal tract (1). Patients often have multiple complications, which seriously affect the quality of life. Compared with adults, pediatric patients with CD have fewer drug choices, more difficult treatment, higher cost, poor prognosis, and need more therapeutic drugs to choose. Despite the increasing number of available treatments, anti-tumor necrosis factor (TNF) agents remain the only biological therapy for pediatric patients with moderate to severe CD (2, 3). Despite their recognized effectiveness, the primary non-response rate is 10%–30% and the secondary loss of response rate is 13%–40% (4–7).
In recent years, new biologics have been approved for the treatment of CD in adults. Foreign studies have shown that ustekinumab (UST) has high clinical remission rate and safety on CD in the treatment of tumor necrosis factor (TNF-α) antibody loss in adults, but there is little experience in treating CD in children (8, 9). At present, the mechanism of action of UST in the treatment of CD is not very clear. The main mechanism may be that UST is a fully humanized IgG1 monoclonal antibody that binds with specificity to the p40 protein subunit of interleukins IL-12 and IL-23 blocks the inflammatory pathway mediated by downstream Th1 cells and Th17 cells (10, 11). As we have seen previously with biologics first marketed in the adult Inflammatory bowel disease (IBD) population, there is increasing off-label use of UST in children even in the absence of pediatric pharmacokinetic data. Data on the effectiveness of UST in the pediatric population is limited. However, with increasing off-label use in children, more data on safety and effectiveness in children with IBD are needed. Herein we report our experience on the clinical effectiveness and safety of UST in the treatment of CD in children and adolescents from three tertiary care IBD referral center in China.
Methods PatientsThis study was a retrospective multicenter study carried out at three tertiary care centers in Shanghai, China. We reviewed a database of pediatric IBD patients diagnosed before age 18. As of November 2023, patients with CD who received their first dose of UST at 18 years old or younger and followed up for a minimum of 24 weeks were included in this study. All patients were cared for by a board-certified gastroenterologist, and UST was prescribed at the discretion of the prescribing physician. Ethics approval for the study was obtained from the ethics committee of each center. Informed consent for participation and sample collection was obtained from their parents.
Data collectionElectronic medical records were reviewed for demographic, medical and surgical treatment history, including steroid use, past biologics and immunomodulator exposure, disease location and behavior (Paris classification) (12), and disease activity (Weighted pediatric CD activity index [wPCDAI] (13). Clinical activity scores and associated laboratory data were recorded at baseline (ustekinumab initiation time) and at 24–32 and 48–56 weeks of follow-up. Laboratory data included complete blood count, albumin, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and fecal calprotectin. Considering the different assays used to assess CRP, we believe that this serum marker is elevated when the value ≥8 mg/L. We also collected data on adverse events, including reactions at infusion and injection sites, and serious adverse events (SAEs).
Disease activity assessments and outcome measuresClinical evaluation was performed before induction treatment and at weeks 24–32, and 48–56 of UST therapy via wPCDAI with values indicating clinical remission (<12.5 points). The clinical response, defined as a decrease in wPCDAI >17.5 (13, 14). Colonoscopy was performed at week 0 and weeks 24–32 or weeks 48–56 of UST therapy to assess mucosal healing by using a simple endoscopic CD score (SES-CD). Endoscopic remission was defined as SES-CD <3 points and a decline in the SES-CD of >50% was defined as endoscopic response (15). In addition, we assessed changes in height, weight, and body mass index (BMI) between baseline to 12 months using a Z-score based on WHO standards.
The primary outcomes were clinical remission at weeks 24–32 and weeks 48–56 of UST therapy. Secondary outcomes were clinical response at the same time points, endoscopic remission, changes in CRP, ESR, albumin and fecal calprotectin, improvement in growth parameters.
Date analysesStatistical analysis was performed using SPSS 20.0 for Windows (IBM, Somers, NY). Continuous clinical and demographic variables are expressed as the median and interquartile range (IQR). The categorical variables are expressed as percentages. The Mann–Whitney test was applied for the comparison of two groups. P value <0.05 was considered statistically significant.
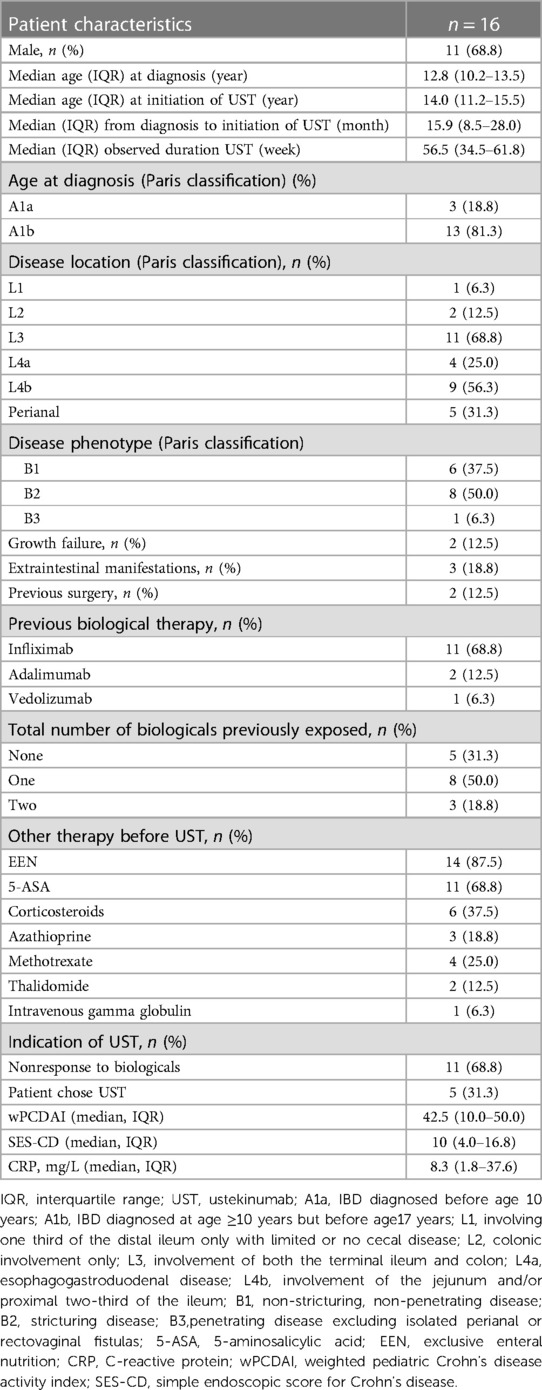
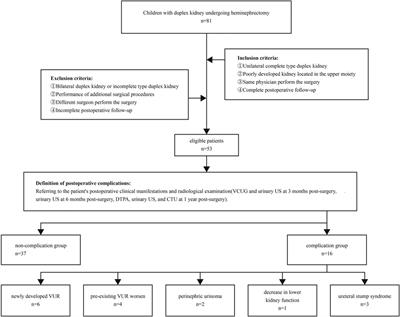
Results Patient characteristics and UST regimensFrom the three hospitals, we identified 16 patients with CD who received UST treatment. The demographic information and disease characteristics of those patients are summarized in Table 1. Among three Ala, two were very early-onset IBD (VEO-IBD), and one of the cases with IL-10 gene defect confirmed by whole exome sequence. Among the 13 cases of Alb, one with the defect of BTK gene confirmed by whole exome sequence. Except for 5 bio-naïve patients whose parents actively chose UST, all others (68.8%) received alternative biologics before UST treatment. Only one patient was treated with corticosteroids accompany, and the corticosteroids were discontinued within 16 weeks of UST treatment. At baseline, while 12 patients were in the active phase of the disease and the remaining four were in clinical remission following receiving exclusive enteral nutrition (EEN) therapy. However, one patient still had intestinal stenosis and capsule endoscopy incarceration after EEN treatment, other three patients had active disease on colonoscopy, which warranted the initiation of UST. Two patients discontinued UST at week 32 due to the poor response. Among the 13 cases who had been followed more than 1 year, 11/13 (84.6%) remained on UST treatment.
Table 1. Demographics and clinical characteristics of pediatric crohn’s disease patients at initiation of UST.
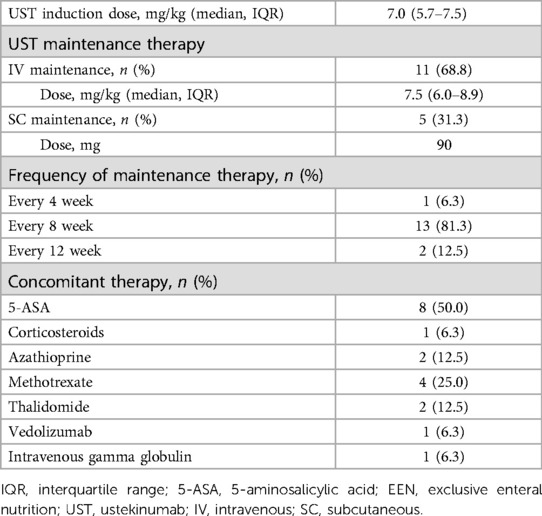
Because UST has not been approved for children with CD, the dose and interval between doses refers to the regimen approved in Chinese adult CD patients (induction with 260 mg for patients <55 kg, 390 mg for patients ≤85 kg, and 520 mg for patients >85 kg, intravenously, maintenance with 90 mg every 8–12 weeks, subcutaneously) and Phase 1 clinical trial of UST in children with moderate to severe active CD (16). Patients older than 15 years of age or weighing more than 40 kg received an adult dose of UST. While the others received a first induction dose of 6–9 mg/kg intravenously at week 0 and followed by an intravenous infusion of 6–9 mg/kg for maintenance every 4–8 weeks, or a subcutaneous infusion of 90 mg/dose for maintenance every 8–12 weeks. In summary, Table 2 summarizes UST treatment information including dose and administration method at induction, the mode, frequency, and duration of maintenance therapy administration. Referring to the relevant literature in adults and children, all patients received a first induction dose of 6–9 mg/kg intravenously. And then according to the disease activity and the wishes of their families, five patients followed by a subcutaneous infusion for maintenance every 8–12 weeks. Other eleven patients received an intravenous infusion for maintenance, including 10 of them at an interval of 8 weeks, and one patient received continuous intravenous infusion maintenance every 4 weeks due to severe disease activity and multi-segmental stenosis of the small intestine. During the follow-up period, one patient needed to shorten the interval to every 6 weeks. One child was still in clinical activity after shortening to 4 weeks, so treatment with UST was discontinued at 32 weeks.
Table 2. UST therapy of the study cohort (n = 16).
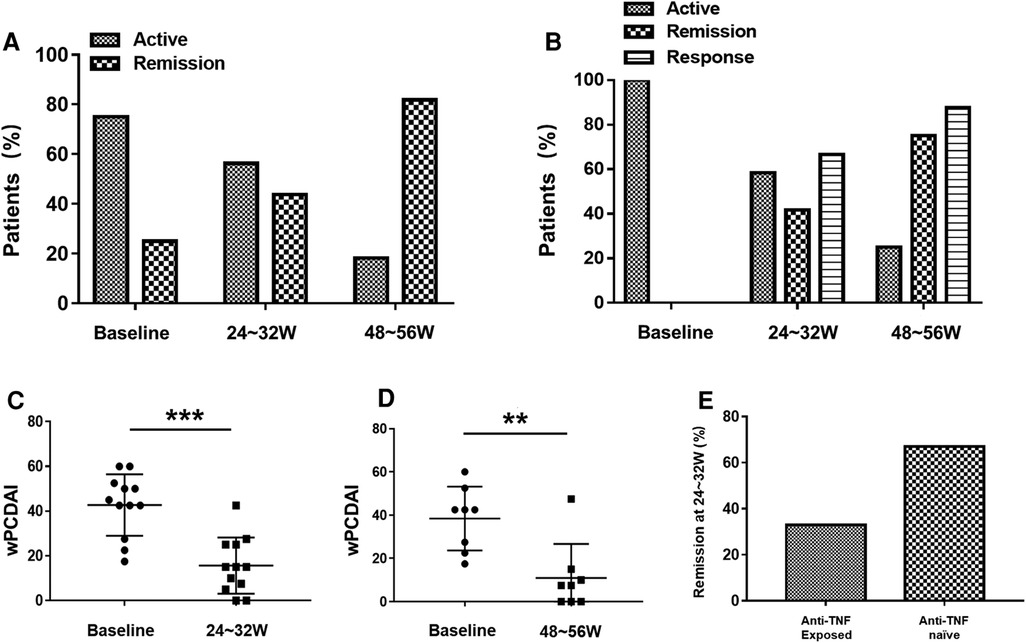
Clinical outcomesFour patients (25%) had a wPCDAI (<12.5) indicating clinical remission at baseline. However, one patient still had intestinal stenosis and capsule endoscopy incarceration after EEN treatment, other three patients had active disease on colonoscopy, which warranted the initiation of UST. As shown in Figure 1A, the clinical remission improved to 56.3% at 24–32 weeks and to 81.8% at 48–56 weeks of UST treatment. In addition, among patients who were clinical active at baseline, there was a significant decrease in wPCDAI at 24–32 weeks of UST treatment (43.8, IQR: 31.3–51.9 vs.15, IQR: 5.6–25, p < 0.001) (Figure 1C). At 24–32 weeks of UST therapy, 8/12 patients (66.7%) achieved clinical response, and 5/12 patients (41.7%) achieved clinical remission. Among patients followed over 48–52 weeks, 7/8 patients (87.5%) achieved clinical response, and 6/8 patients (75%) achieved clinical remission at 48–56 weeks (Figure 1B) and wPCDAI was significantly lower than baseline (42.5, IQR: 23.8–50 vs. 7.5, IQR: 0–13.8, p = 0.004) (Figure 1D).
Figure 1. (A) Proportion of patients in clinical remission and active phase under ustekinumab treatment (at baseline, weeks 24–32 and weeks 48–56). (B) Proportion of patients (wPCDAI > 12.5 at baseline) in clinical remission, clinical response and active phase under ustekinumab treatment (at baseline, weeks 24–32 and weeks 48–56). Changes in wPCDAI at baseline and weeks 24–32 (C) or baseline and weeks 48–56 (D) of patients who were clinical active at baseline. (E) Ustekinumab remission rates at weeks 24–32 in anti-TNF exposed vs. biologic-naïve Crohn disease patients. wPCDAI = weighted pediatric Crohn's disease activity index, TNF = tumor necrosis factor. **P < 0.01, ***P < 0.001.
Eleven patients had been exposed to anti-TNF therapy before starting UST, of which two patients had been on ≥2 anti-TNF. The cause for discontinuation of anti-TNF included secondary loss of response (n = 10) and primary nonresponse to anti-TNF (n = 1). Bio-naïve patients were more likely to achieve clinical remission than bio-exposed patients 66.7% vs. 33.3% at 24–32 weeks, respectively (Figure 1E).
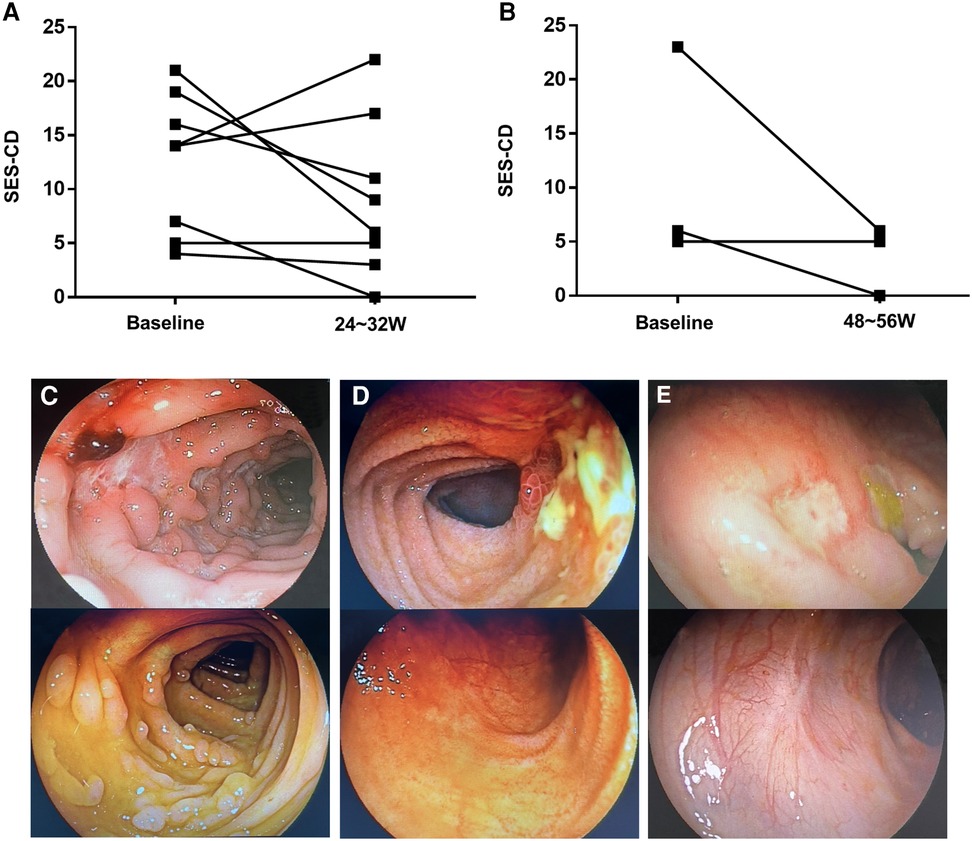
Endoscopic outcomesAll patients underwent colonoscopy at baseline. During follow-up, colonoscopy were performed with scoring of SES-CD in 11 patients. Of those, eight were performed at 24–32 weeks and three at 48–56 weeks. Figures 2A,B shows the change in SES-CD. Among the eight patients evaluated at week 24–32, 1/8 patients (12.5%) achieved endoscopic remission and 3/8 patients (37.5%) achieved endoscopic response. Three patients were evaluated at weeks 48–56, of whom one (33.3%) achieved endoscopic remission and two (66.7%) achieved endoscopic response. Figures 2C–E shows the change in endoscopy findings of three patients who achieved clinical response during follow-up.
Figure 2. (A) Changes in the simple endoscopic score (SES-CD) of eight patients at weeks 24–32. (B) Changes in the SES-CD of three patients at weeks 48–56. (C) Transverse colon findings in a 11-year-old girl (at week 0, at week 24). (D) Findings of terminal ileum in a 12-year-old girl (at week 0 and at week 26). (E) Findings of descending colon in a 3-year-old boy (at week 0 and at week 27).
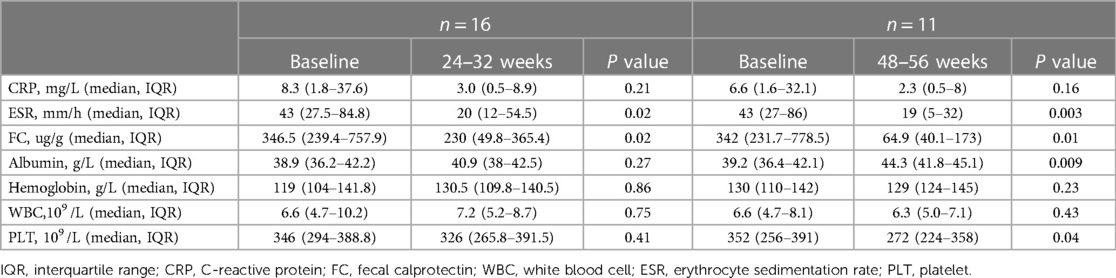
Biologic outcomesAt baseline, eight (50%) patients had a normal CRP. Among the eight with an elevated baseline CRP, the test normalised in four at 24–32 weeks. 9/11 (81.8%) patients who were followed over 48–56 weeks achieved normal CRP at 48–56 weeks. The longitudinal changes of biological indicators at baseline and during maintenance therapy are shown in Table 3. It can be seen that ESR and fecal calprotectin decreased significantly at 24–32 weeks and 48–56 weeks after UST treatment. Serum albumin levels and platelet counts were significantly improved at 48–56 weeks compared to baseline. White blood cell count, hemoglobin and CRP levels did not change significantly over time.
Table 3. Summary of clinical indicators at baseline, at 24∼32 weeks and at 48∼56 weeks.
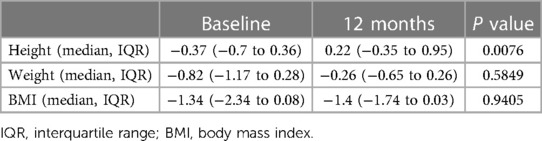
GrowthThe growth parameters are summarised in Table 4. Height Z-scores increased significantly from baseline to 12 months (−0.37, IQR: −0.7 to 0.36 vs. 0.22 IQR: −0.3 to 0.95, p = 0.0076). Weight Z-scores improved from baseline to 12 months (−0.82, IQR: −1.17 to 0.28 vs. −0.26 IQR: −0.65 to 0.26, p = 0.5849), the change was not significant. There was no significant change in BMI Z-score.
Table 4. Summary of growth parameters, expressed as Z-scores, at baseline and at 12 months.
Perianal diseaseFive patients had perianal disease at diagnosis and four had perianal disease activity before treatment with UST. One patient experienced an exacerbation of perianal disease and no improvement in diarrhea after treatment with UST and one VEO-IBD patient with severe perianal disease also did not improve satisfactorily with the use of UST. However, perianal disease in the other two patients improved significantly, and perianal disease did not occur in the other patients.
Stricturing diseaseEight patients had significant intestinal stenosis at the time of initial UST treatment, and four of them had colorectal stenosis. After UST treatment, one case of colon stenosis improved from multiple stenosis to one stenosis, while the other three cases had no significant improvement. Among the four children with small intestine stenosis, three of them underwent capsule endoscopy stuck in the small intestine. All of the four children with intestinal stenosis improved to varying degrees after UST treatment, and two of the children had their capsules excreted in the stool after about three months of UST treatment.
Drug safetyAdverse events that were potentially related to therapy were reported in eight (50%) children, including one clostridium difficile infection in one patient (treated with oral antibiotics), one otitis media in one patient, and nine events of upper respiratory tract infection in eight patients. All adverse events were mild and no serious adverse events were noted with UST. During maintenance, adverse events were not the cause of medication cessation. In contrast, two patients discontinued UST due to the poor clinical response.
Drug concentrations and antidrug antibodiesOf the 16 patients included in this study, 11 (69%) had UST drug concentrations and antidrug antibody levels tested (HeRui IBD, Suzhou, China) at a median time of 26 (24–43) weeks after UST initiation. Of the 11 patients, none had antibodies detected and concentrations ranged from 0.9 to 20 ug/ml. Nine patients had trough concentrations at weeks 24–32—median trough concentration for the patients was 10.3 (5.35–14.3) ug/ml. The median trough concentration for those in clinical remission was 13.65 (8.15–18.55) ug/ml compared with 5.5 (3.55–12.35) ug/ml for the patients not in clinical remission at weeks 24∼32 (p = 0.128). Of the remaining two patients, one had a trough concentration of 11.5 ug/ml at week 82 and one had a trough concentration of 0.9 ug/ml at week 52.
DiscussionCompared with adults, pediatric patients with CD have fewer drug choices, rapid disease progression, more difficult treatment, higher cost, poor prognosis, and need more therapeutic drugs to choose. Despite the increasing number of treatments available, anti- TNF-α drugs remain the only proven and approved biologic therapy for pediatric patients with moderate to severe CD (2, 3). However, the treatment of CD with anti-TNF-α may lead to drug allergy, no response or secondary loss of response (4). Therefore, anti-TNF-α agents cannot meet the therapeutic needs of all pediatric patients with CD. The efficacy of UST for adult CD patients has been reported in the IM-UNITI study. 46.9% of patients achieved steroid-free remission and 10.9% achieved an endoscopic remission at week 44 (10, 17).
The regimen of UST for pediatric CD patients is not explicit. The most common regimen is an induction doses with 6 mg/kg intravenously and maintenance with 90 mg every 8–12 weeks, subcutaneously. Sandborn et al. reported that the high dose of UST therapy can improve the clinical response rate and clinical remission rate of CD patients (18). A multicenter retrospective study reported that 66% of patients recaptured response following treatment intensification with UST 90 mg every 4 weeks (19). Dayan et al. reported the rates of steroid-free remission at week 52 (60%) (20). Their regimen consisted of an intravenous induction dose followed by subcutaneous maintenance doses every 8 weeks; meanwhile, interval shortening to every 4 weeks or re-induction of UST was required in 39% of patients. In addition, the study also showed that bio-naïve patients were significantly more likely to achieve steroid-free remission than bio-exposed patients (20), suggesting that more aggressive UST therapy is needed in bio-exposed patients. Based on the above results, this study adopted a more aggressive regimen of UST. All patients were decision to prescribe UST was at the discretion of the prescribing physician.
Currently, data on the efficacy and safety of UST in the pediatric population are limited, and results vary widely among studies. This study reports on real-life experience using UST for the treatment of CD in a pediatric and young-adult patients from multiple IBD referral centers. Our data demonstrate that the steroid-free clinical remission rates were 41.7% at weeks 24–32, 75% at weeks 48–56 and clinical response rate were 66.7% at weeks 24–32, 87.5% at weeks 48–56. During the follow-up period, the endoscopic response rate and endoscopic remission rate were 45.5% and 18.2%, respectively. This suggests that pediatric and young adult patients could benefit from UST as either a primary or secondary biologic therapy for the induction, or maintenance of remission of CD. However, there were only few reports regarding the use of UST for pediatric patients with CD. A retrospective multicenter cohort study for pediatric patients reported that twelve of 44 (27.3%) patients achieved steroid-free remission at 12 months. In their study, induction therapy was given subcutaneously (21). Another single-center retrospective study of children from Japan reported the steroid-free clinical remission rates were 59% at week 26, 50% at week 52 (22). Patients in their study received an induction dose of 6–9 mg/kg intravenously, followed by subcutaneous injections every 8–12 weeks. The higher clinical response and remission rates in our study may be related to our more aggressive regimen of UST. In our study, all patients received a first induction dose intravenously, and then according to the disease activity and the wishes of their families, five patients followed by a subcutaneous infusion for maintenance every 8–12 weeks. Other eleven patients received an intravenous infusion for maintenance. So, we divided the results by different regiments between maintenance subcutaneously group and maintenance intravenously group to determine the effect of different maintenance methods on the treatment efficacy. The results showed there were no significant differences in clinical and biological indicators between the two groups (Supplementary Table S1), which may be limited by the small sample size. In addition, 68.75% of our cohort failed previous biologic treatments. Bio-naïve patients have a clinical remission rate of up to 66.7% at weeks 24–32. However, only a minority of our cohort were bio-naïve, so more date on exposure are needed to confirm this finding.
Traditional serological inflammatory markers such as CRP, ESR, albumin, and hemoglobin are associated with the disease activity of CD (23), Mallory et al. showed that CRP, ESR and albumin in most children with CD were significantly improved after UST treatment (21). In our study, CRP and ESR decreased and albumin and hemoglobin increased in most patients compared with baseline, which is consistent with the results of other studies. Many studies have shown that fecal calprotectin elevation is highly correlated with endoscopic disease activity, which can be used to evaluate the therapeutic effect of CD (24, 25). In this study, fecal calprotectin was significantly decreased in all patients, which also indicated the effectiveness of UST for the children with CD.
Compared with adult patients, children with IBD have a higher proportion of malnutrition which affects children’s growth and development (26). Mallory et al. showed that albumin and prealbumin of children were significantly improved after UST treatment, and their body weight increased significantly (21). In our study, the height Z-scores and weight Z-scores of patients increased compared with the baseline. Although there was no significant difference in the weight Z-scores, which may be limited by the small sample size.
Perianal disease seriously affect patients’ quality of life. Adult studies have shown that in adult CD patients treated with UST, the anal fistula remission rate over 24 weeks was 37.5% (27). In our study, the remission rate of anal fistula at 48–56 weeks was 2/4 (50%), which was higher than that in other studies, which may be related to the small sample size, and it is necessary to further expand the sample size to observe the effect of UST treatment of CD on perianal disease in children. UST is a fully humanized IgG1 monoclonal antibody that binds with specificity to the p40 protein subunit of interleukins IL-12 and IL-23 blocks the pathway mediated by downstream Th1 cells and Th17 cells, which reducing TGF-β and IL-17/22 production, thereby affecting myofibroblast formation and slowing down intestinal fibrosis (10, 11, 28). Our study showed that 5/8 (62.5%) of the children had varying degrees of improvement in intestinal stenosis, indicating that patients with stenosis can benefit from UST treatment.
Therapeutic drug monitoring (TDM) with UST is at its infancy. The clinical utility of TDM with non-anti-TNF mechanisms of action is not clear. A review of novel biologics for TDM in IBD recommended that UST concentrations of 3–7 ug/ml at week 8 and 1–3 ug/ml during maintenance have been associated with improved outcomes and dose optimization generally improves clinical outcomes in those with partial response or loss of response (29). In a recent post hoc analysis of UNITI studies (UNITI 1,2), Adedokun et al. reported that serum concentrations of UST during induction were correlated to the dose administration and therapeutic effect (30). The median trough concentration at weeks 24–32 in our study was 10.3 (5.35–14.3) ug/ml, and the median trough concentration for those in steroid-free remission was much higher than that patients who not in steroid-free remission at weeks 24–32. Although there was no statistical difference, this may be related to the small sample size. In addition, none of our patients had detectable anti-drug antibodies.
The safety of biologics in the treatment of CD in children is the most concerned issue for pediatricians and their families. A meta-analysis showed that 27% patients experienced adverse events, and serious adverse events was about 8.9%. Among the serious adverse events, infection was the most common, the incidence of tumor was 0.29%, and no tumor was reported in children (31). In this study, the patients were treated with a more active UST regimen. Although eight patients (50%) reported potentially treatment-related adverse events, all of the adverse events were mild and no children were discontinued as a result. However, the sample size is small, and it is necessary to further expand the sample size and prolong the observation time to obtain more reliable safety data of UST treatment of CD in children.
To date, UST treatment in children with monogenic IBD has been limited (32, 33). Of our two monogenic IBD patients, the one with BTK gene deficiency achieved a clinical response at 24 weeks, while the child with IL-10 gene deficiency did not achieve a clinical response at 24 weeks. Children with monogenic IBD face more difficult treatment challenges than those with non-monogenic. Biologics may be a viable option for partial monogenic IBD, but this needs to be validated with more research. Our study expands the experience of UST in the treatment of monogenic IBD.
In conclusion, our experience with the use of UST suggest that UST is efficacious and safe in pediatric CD patients. Given the real experience reported in our study and the various indications of use and phenotypes, it should be considered a viable treatment option for pediatric CD patients.
Data availability statementThe original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statementThe studies involving humans were approved by Ethical Committee of Children's Hospital, Fudan University, the Shanghai Tenth People's Hospital, Tongji University and Xinhua Hospital, School of Medicine, Shanghai Jiao Tong University. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributionsPL: Data curation, Formal Analysis, Investigation, Writing – original draft. LW: Formal Analysis, Investigation, Writing – review & editing. ZT: Formal Analysis, Investigation, Writing – review & editing. YW: Formal Analysis, Investigation, Writing – review & editing. ZL: Formal Analysis, Investigation, Writing – review & editing. WG: Formal Analysis, Investigation, Writing – review & editing. YH: Formal Analysis, Investigation, Supervision, Writing – review & editing.
FundingThe author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This study was supported by Natural Science Foundation of Shanghai Municipality (Grant Number: 21ZR1410300).
AcknowledgmentsThe authors would like to thank all the patients and their families who participated in the study.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary materialThe Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2024.1371322/full#supplementary-material
References1. Fumery M, Pariente B, Sarter H, Savoye G, Spyckerelle C, Djeddi D, et al. Long-term outcome of pediatric-onset Crohn’s disease: a population-based cohort study. Digest Liver Dis. (2019) 51(4):496–502. doi: 10.1016/j.dld.2018.11.033
Crossref Full Text | Google Scholar
2. Hyams J, Crandall W, Kugathasan S, Griffiths A, Olson A, Johanns J, et al. Induction and maintenance infliximab therapy for the treatment of moderate-to-severe Crohn’s disease in children. Gastroenterology. (2007) 132(3):863–73. doi: 10.1053/j.gastro.2006.12.003
PubMed Abstract | Crossref Full Text | Google Scholar
3. Hyams JS, Griffiths A, Markowitz J, Baldassano RN, Faubion WA, Colletti RB, et al. Safety and efficacy of Adalimumab for moderate to severe Crohn’s disease in children. Gastroenterology. (2012) 143(2):365-+. doi: 10.1053/j.gastro.2012.04.046
Crossref Full Text | Google Scholar
4. Sprakes MB, Ford AC, Warren L, Greer D, Hamlin J. Efficacy, tolerability, and predictors of response to infliximab therapy for Crohn’s disease: a large single centre experience. J Crohns Colitis. (2012) 6(2):143–53. doi: 10.1016/j.crohns.2011.07.011
PubMed Abstract | Crossref Full Text | Google Scholar
5. Ford AC, Sandborn WJ, Khan KJ, Hanauer SB, Talley NJ, Moayyedi P. Efficacy of biological therapies in inflammatory bowel disease: systematic review and meta-analysis. Am J Gastroenterol. (2011) 106(4):644–59. doi: 10.1038/ajg.2011.73
PubMed Abstract | Crossref Full Text | Google Scholar
6. Ben-Horin S, Chowers Y. Review article: loss of response to anti-TNF treatments in Crohn’s disease. Aliment Pharm Ther. (2011) 33(9):987–95. doi: 10.1111/j.1365-2036.2011.04612.x
Crossref Full Text | Google Scholar
7. Gisbert JP, Panés J. Loss of response and requirement of infliximab dose intensification in Crohn’s disease: a review. Am J Gastroenterol. (2009) 104(3):760–7. doi: 10.1038/ajg.2008.88
PubMed Abstract | Crossref Full Text | Google Scholar
8. Verstockt B, Dreesen E, Noman M, Outtier A, Van den Berghe N, Aerden I, et al. Ustekinumab exposure-outcome analysis in Crohn’s disease only in part explains limited endoscopic remission rates. J Crohns Colitis. (2019) 13(7):864–72. doi: 10.1093/ecco-jcc/jjz008
PubMed Abstract | Crossref Full Text | Google Scholar
9. Ollech JE, Normatov I, Peleg N, Wang JZ, Patel SA, Rai V, et al. Effectiveness of ustekinumab dose escalation in patients with Crohn’s disease. Clin Gastroenterol H. (2021) 19(1):104–10. doi: 10.1016/j.cgh.2020.02.035
Crossref Full Text | Google Scholar
10. Feagan BG, Sandborn WJ, Gasink C, Jacobstein D, Lang Y, Friedman JR, et al. Ustekinumab as induction and maintenance therapy for Crohn’s disease. New Engl J Med. (2016) 375(20):1946–60. doi: 10.1056/NEJMoa1602773
PubMed Abstract | Crossref Full Text | Google Scholar
11. Gisbert JP, Chaparro M. Ustekinumab to treat Crohn’s disease. Gastroent Hepat-Barc. (2017) 40(10):688–98. doi: 10.1016/j.gastrohep.2017.08.006
Crossref Full Text | Google Scholar
12. Levine A, Griffiths A, Markowitz J, Wilson DC, Turner D, Russell RK, et al. Pediatric modification of the Montreal classification for inflammatory bowel disease: the Paris classification. Inflamm Bowel Dis. (2011) 17(6):1314–21. doi: 10.1002/ibd.21493
PubMed Abstract | Crossref Full Text | Google Scholar
13. Turner D, Griffiths AM, Walters TD, Seah T, Markowitz J, Pfefferkorn M, et al. Mathematical weighting of the pediatric Crohn’s disease activity index (PCDAI) and comparison with its other short versions. Inflamm Bowel Dis. (2012) 18(1):55–62. doi: 10.1002/ibd.21649
PubMed Abstract | Crossref Full Text | Google Scholar
14. Yerushalmy-Feler A, Pujol-Muncunill G, Martin-de-Carpi J, Kolho KL, Levine A, Olbjorn C, et al. Safety and potential efficacy of escalating dose of ustekinumab in pediatric Crohn disease (the speed-up study): a multicenter study from the pediatric IBD porto group of ESPGHAN. J Pediatr Gastr Nutr. (2022) 75(6):717–23. doi: 10.1097/MPG.0000000000003608
Crossref Full Text | Google Scholar
15. Daperno M, D'Haens G, Van Assche G, Baert F, Bulois P, Maunoury V, et al. Development and validation of a new, simplified endoscopic activity score for Crohn’s disease: the SES-CD. Gastrointest Endosc. (2004) 60(4):505–12. doi: 10.1016/S0016-5107(04)01878-4
PubMed Abstract | Crossref Full Text | Google Scholar
16. Rosh JR, Turner D, Griffiths A, Cohen SA, Jacobstein D, Adedokun OJ, et al. Ustekinumab in paediatric patients with moderately to severely active Crohn’s disease: pharmacokinetics, safety, and efficacy results from UniStar, a phase 1 study. J Crohns Colitis. (2021) 15(11):1931–42. doi: 10.1093/ecco-jcc/jjab089
PubMed Abstract | Crossref Full Text | Google Scholar
17. Rutgeerts P, Gasink C, Chan D, Lang YH, Pollack P, Colombel JF, et al. Efficacy of ustekinumab for inducing endoscopic healing in patients with crohn’s disease. Gastroenterology. (2018) 155(4):1045–58. doi: 10.1053/j.gastro.2018.06.035
PubMed Abstract | Crossref Full Text | Google Scholar
18. Sandborn WJ, Gasink C, Gao LL, Blank MA, Johanns J, Guzzo C, et al. Ustekinumab induction and maintenance therapy in refractory crohn’s disease. New Engl J Med. (2012) 367(16):1519–28. doi: 10.1056/NEJMoa1203572
PubMed Abstract | Crossref Full Text | Google Scholar
19. Fumery M, Peyrin-Biroulet L, Nancey S, Altwegg R, Gilletta C, Veyrard P, et al. Effectiveness and safety of ustekinumab intensification at 90 mg every 4 weeks in Crohn’s disease: a multicentre study. J Crohns Colitis. (2021) 15(2):222–7. doi: 10.1093/ecco-jcc/jjaa177
Crossref Full Text | Google Scholar
20. Dayan JR, Dolinger M, Benkov K, Dunkin D, Jossen J, Lai J, et al. Real world experience with ustekinumab in children and young adults at a tertiary care pediatric inflammatory bowel disease center. J Pediatr Gastr Nutr. (2019) 69(1):61–7. doi: 10.1097/MPG.0000000000002362
Crossref Full Text | Google Scholar
21. Chavannes M, Martinez-Vinson C, Hart L, Kaniki N, Chao CY, Lawrence S, et al. Management of paediatric patients with medically refractory crohn’s disease using ustekinumab: a multi-centred cohort study. J Crohns Colitis. (2019) 13(5):578–84. doi: 10.1093/ecco-jcc/jjy206
PubMed Abstract | Crossref Full Text | Google Scholar
22. Takeuchi I, Arai K, Kyodo R, Sato T, Tokita K, Hirano Y, et al. Ustekinumab for children and adolescents with inflammatory bowel disease at a tertiary children’s hospital in Japan. J Gastroen Hepatol. (2021) 36(1):125–30. doi: 10.1111/jgh.15128
Crossref Full Text | Google Scholar
24. Vázquez-Morón JM, Benítez-Rodríguez B, Pallarés-Manrique H, Machancoses FH, Rodríguez JLR, Ramos-Lora M, et al. Accurate cut-offs for predicting endoscopic activity and mucosal healing in Crohn’s disease with fecal calprotectin. J Crohns Colitis. (2017) 11:S239-S. doi: 10.1093/ecco-jcc/jjx002.444
Crossref Full Text | Google Scholar
25. Narula N, Wong ECL, Dulai PS, Marshall JK, Colombel JF, Reinisch W. Week 6 calprotectin best predicts likelihood of long-term endoscopic healing in Crohn’s disease: a post-hoc analysis of the UNITI/IM-UNITI trials. J Crohns Colitis. (2021) 15(3):462–70. doi: 10.1093/ecco-jcc/jjaa189
PubMed Abstract | Crossref Full Text | Google Scholar
27. Biemans VBC, van der Meulen-de Jong AE, van der Woude CJ, Löwenberg M, Dijkstra G, Oldenburg B, et al. Ustekinumab for Crohn’s disease: results of the a nationwide prospective observational cohort study. J Crohns Colitis. (2020) 14(1):33–45. doi: 10.1093/ecco-jcc/jjz119
PubMed Abstract | Crossref Full Text | Google Scholar
28. Murate K, Nakamura M, Yamamura T, Maeda K, Sawada T, Mizutani Y, et al. Ustekinumab is effective against small bowel lesions in Crohn’s disease: two case reports. Clin J Gastroenterol. (2021) 14(1):129–35. doi: 10.1007/s12328-020-01242-0
PubMed Abstract | Crossref Full Text | Google Scholar
29. Restellini S, Afif W. Update on TDM (therapeutic drug monitoring) with ustekinumab, vedolizumab and tofacitinib in inflammatory bowel disease. J Clin Med. (2021) 10(6):1242. doi: 10.3390/jcm10061242
PubMed Abstract | Crossref Full Text | Google Scholar
30. Adedokun OJ, Xu ZH, Gasink C, Jacobstein D, Szapary P, Johanns J, et al. Pharmacokinetics and exposure response relationships of ustekinumab in patients with Crohn’s disease. Gastroenterology. (2018) 154(6):1660–71. doi: 10.1053/j.gastro.2018.01.043
PubMed Abstract | Crossref Full Text | Google Scholar
31. de Célix CR, Chaparro M, Gisbert JP. Real-world evidence of the effectiveness and safety of ustekinumab for the treatment of Crohn’s disease: systematic review and meta-analysis of observational studies. J Clin Med. (2022) 11(14):4202. doi: 10.3390/jcm11144202
Crossref Full Text | Google Scholar
32. Kyodo R, Takeuchi I, Narumi S, Shimizu H, Hata K, Yoshioka T, et al. Novel biallelic mutations in the gene underlying very early-onset inflammatory bowel disease: a case report. Clin Immunol. (2022):238. doi: 10.1016/j.clim.2022.109015
Crossref Full Text | Google Scholar
33. Khan F, Person H, Dekio F, Ogawa M, Ho HE, Dunkin D, et al. Crohn’s-like enteritis in X-linked agammaglobulinemia: a case series and systematic review. J Aller Cl Imm-Pract. (2021) 9(9):3466–78. doi: 10.1016/j.jaip.2021.04.070
留言 (0)