
記住我





The prospective, randomized, double-blinded, single-center trial was approved by the Ethics Committee of the First Affiliated Hospital of Sun Yat-sen University (Guangzhou, Guangdong, China. No. [2019]334, chairperson Churong Ji) on 12/09/2019. Written informed consent was obtained from all subjects participating in the trial. The trial was registered prior to patient enrollment at Chinese Clinical Trial Registry (ChiCTR1900028404, Principal investigator: Xia Feng, Date of registration: 12/20/2019). At enrollment, all participants provided written informed consent. The Consolidated Standards of Reporting Trials (CONSORT) guidelines were followed in this study (Fig. 1). Recruitment was discontinued when enrollment reached the number suggested by projections to yield sufficient statistical power. A research monitor, independent of the investigative team and approved by Human Research Protection Office, served as an advocate for the safety of the study participants. The research monitor thoroughly reviewed all amendments to the protocol as well as any adverse events, protocol deviations, and other relevant event reports. The monitor diligently assessed the accumulating data from a clinical trial in terms of progress, participant safety, critical efficacy results, and subsequently offer recommendations for potential modifications, continuations or terminations if necessary.
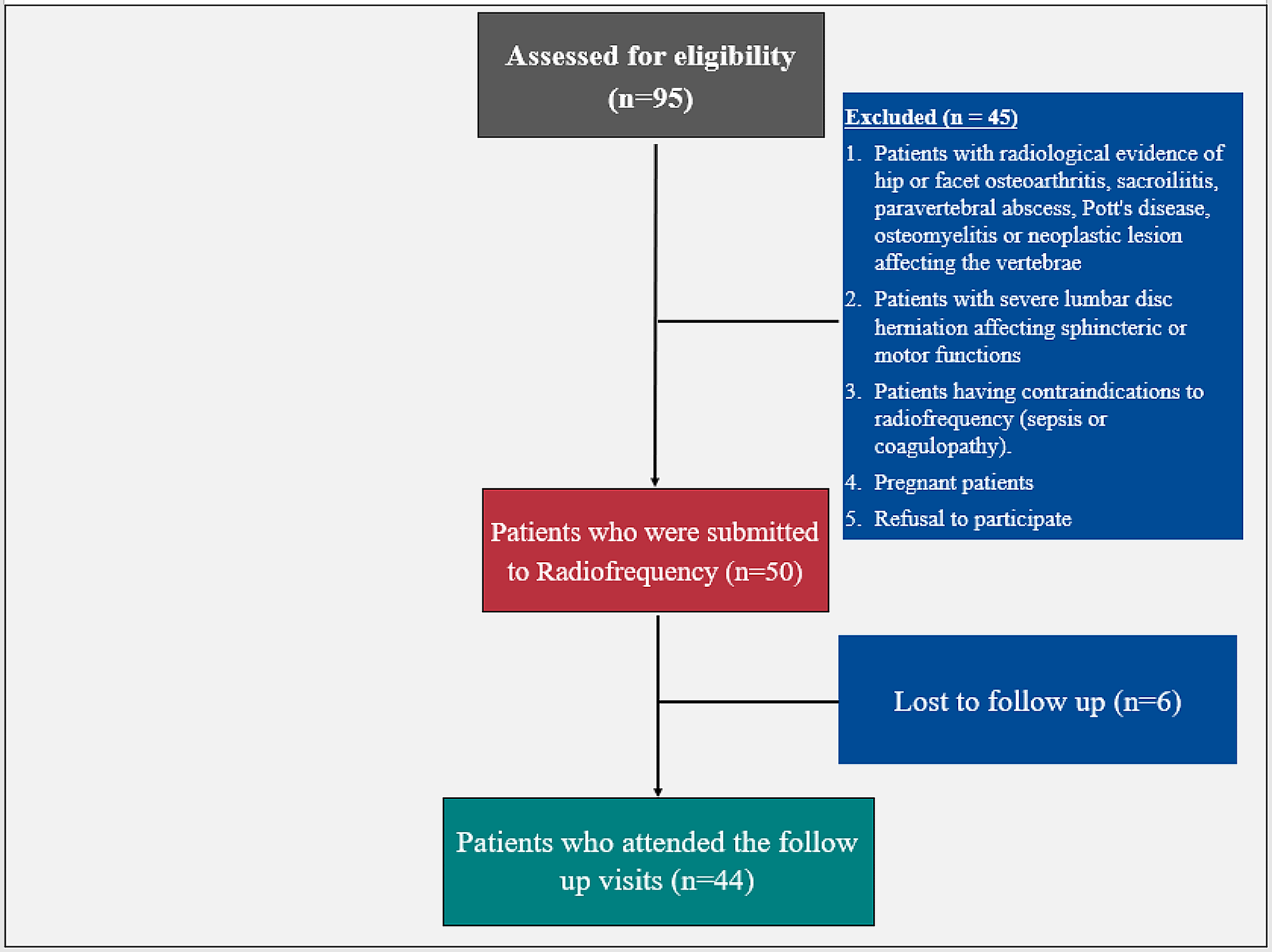
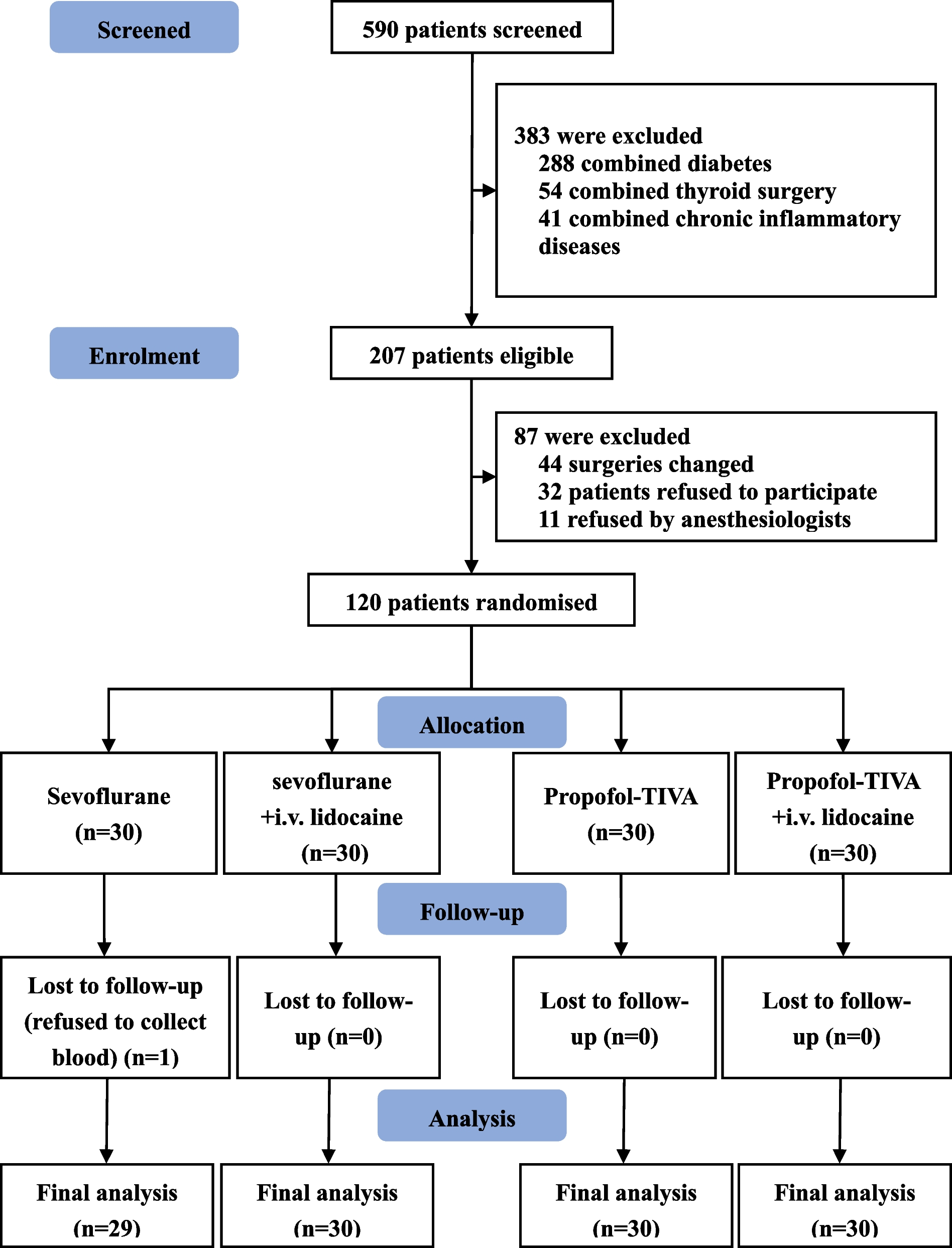
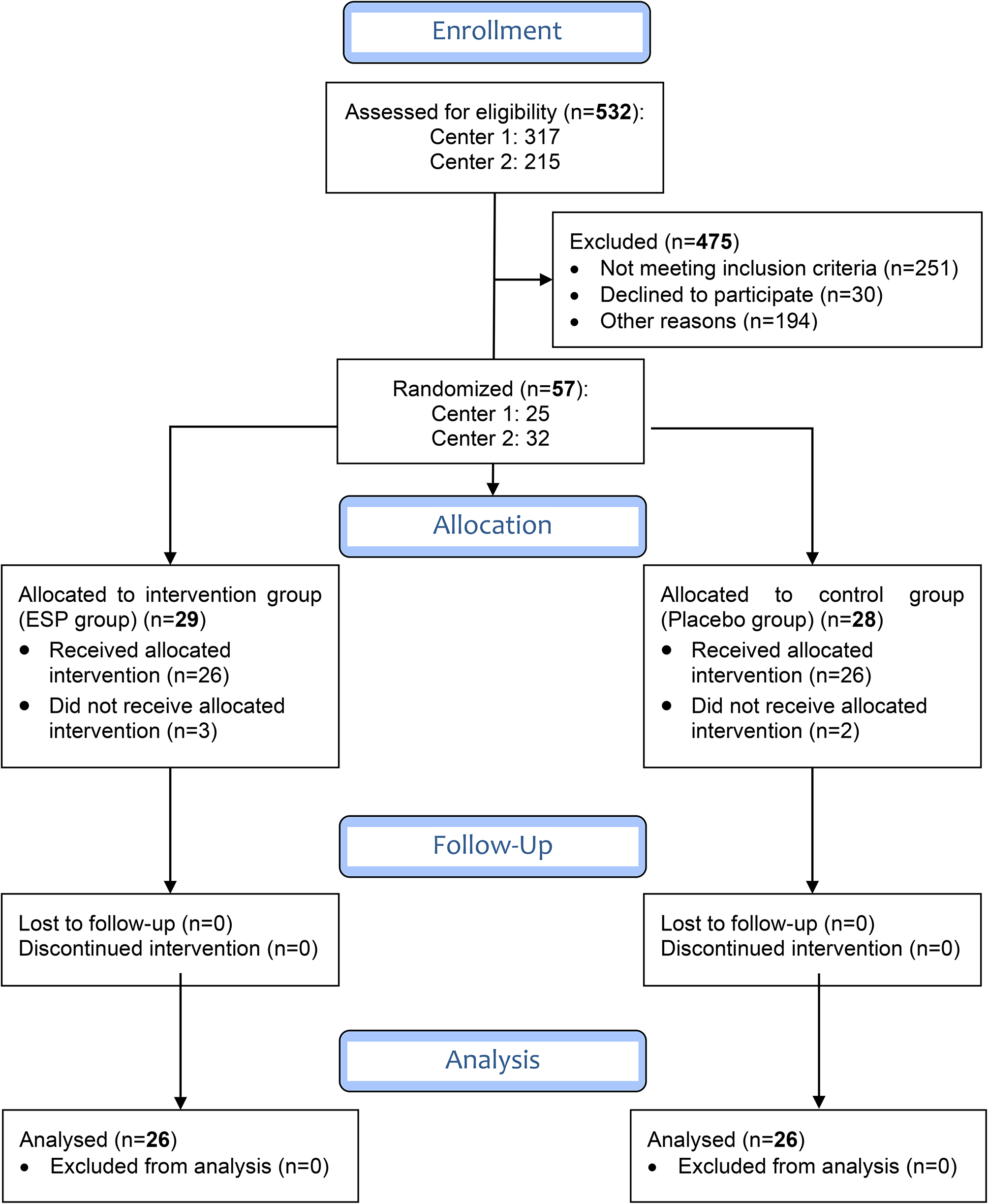
Fig. 1
CONSORT flow chart for this study. CONSORT indicates consolidated standards of reporting trials
Trial participantsKey inclusion criteria included aged 18-70 yr, with the American Society of Anesthesiology (ASA) I-III undergoing laparoscopic radical resection of CRC, fit for elective surgery, and a preoperatively signed informed consent. Key exclusion criteria included emergency operations, operation with enterostomy, patients with communication difficulties before surgery, other serious underlying diseases, and brady-arrhythmias.
All patients were asked to fast preoperatively without premedication. Standard monitoring, including non-invasive blood pressure, heart rate, continuous ECG, oxygen saturation, and end-tidal carbon dioxide, was performed before anesthesia induction. Intravenous access was established, and patients were kept warm with a thermal blanket upon entering the room. Nasopharyngeal temperature, central venous pressure (CVP), Narcotrend value were also recorded after anesthesia induction during the surgery. General anesthesia was administered to all patients, as described below.
Participants were randomized by random numbers generated by software to either a normal saline group (Control group) or a ropivacaine group (SGB group) preoperatively. Software (Microsoft Excel, Version 2013, USA, www.microsoft.com) was used for randomization. Following allocation results, the medication was prepared by an anesthesiologist who was not involved in the study. Study medication included either 10 mL of normal saline (Control group) or 10 mL of 0.2% ropivacaine (SGB group). Anesthesiologists and surgeons were blinded to different local anesthetic regimes.
Anesthesia procedures and perioperative managementAll patients enrolled in this trial received general anesthesia. Anesthesia induction involved intravenous administration of propofol (2 mg/kg), sufentanil (0.2 ug/kg) and cisatracurium (0.2 mg/kg). Following tracheal intubation, propofol (TCI, 1-2ug/ml), remifentanil (TCI, 2–4 ng/ml), and 1% sevoflurane were administered to maintain anesthesia. Internal jugular vein puncture and catheterization were performed after the SGB procedure. Narcotrend monitoring was employed to regulate the sedative stage, maintaining values within the range of 40–60. Perioperative analgesic and anti-emetic management were standardized as sufentanial and palonosetron. Patient-controlled intravenous analgesia (PCVA) with sufentanil was used for postoperative analgesia. The PCVA regimen typically involved a mixture of sufentanil (150 μg) with normal saline, resulting in a total volume of 150 ml. Sufentanil was administered via a pump programmed to deliver a continuous background infusion at a rate of 1 ml/h, with an additional 2 ml available on demand. Patients with a postoperative VAS score of 4 or higher were permitted to self-administer the necessary bolus dose by pressing a button until their VAS score reached ≤ 3.
Ultrasound-guided SGB procedureThe ultrasound-guided SGB was performed after induction of anesthesia. Patients were in the supine position for the ultrasound-guided (X-PORTE; SonoSite Inc., USA) SGB, which was performed by experienced anesthesiologists (who has performed ultrasound-guided SGB for over 30 cases) to identify appropriate anatomical landmarks, avoid intravascular injection, and guide injectate placement [13]. 10 mL of ropivacaine, 0.2%, was injected around and into the site of the ganglion at the level of the C6 anterior tubercle after a negative puff test to exclude intravascular injection and a negative cerebrospinal fluid aspiration. Under out-of-plane ultrasound guidance, a 20-gauge Tuohy needle was applied percutaneously to the anterior or anterolateral edge of the longus colli muscle for participants receiving the active SGB. A short-axis ultrasound view confirmed injectate spread along the longus colli muscle (Fig. 2). Efficacy of the block was confirmed by the specific observer who is aware of the assignment by a temperature change of at least 1 °C in the ipsilateral upper extremity. Horner sign was not included for the patients has already intubated after induction of anesthesia. The sham procedure used the same technique, except normal saline was injected in soft tissues superficial to the anterior tubercle of C6 [14]. All other clinical and study personnel were unaware of treatment assignment.
Fig. 2
Schematic diagram of the SGB procedure. PTTP, posterior tubercle of transverse process. ATTP, anterior tubercle transverse process. N, nerve. LCM, longus colli musculus. IJV, internal jugular vein. CCA, common carotid artery. SCM, sternocleidomastoid muscle. ☆, target site
Possible adverse events related to SGB and their preventive and treatment measures are as follows: potential severe complications, such as intravascular injections, retropharyngeal hematoma, and brachial plexus injury, may arise [15]. While ultrasound guidance was utilized, absolute prevention of these events cannot be guaranteed. Therefore, preventive measures include: precise identification of tissue fascia planes and crucial blood vessels via pre-scan ultrasound, careful planning of a safe needle insertion trajectory, and immediate cessation of the procedure upon encountering a blood vessel or important structure, followed by appropriate handling.
Treatment measures involve applying adequate compression to manage bleeding upon vessel contact, vigilant monitoring of vital signs for signs of local anesthetic poisoning (e.g., increased heart rate), continuous intraoperative ultrasound surveillance for progressive changes in the affected area, post-surgical assessment of nerve damage, swallowing, and vocal function changes, and timely involvement of otolaryngology and vascular surgery departments for assistance as needed.
Outcome measurementsOutcome analysis was conducted via per-protocol analysis. The primary outcome was the time to flatus after surgery as previously reported [9, 10]. As secondary endpoints, we measured the time to the first bowel movement, serum cortisol levels, a solid diet tolerance, additional analgesic requirements, intraoperative complications, postoperative pain score, postoperative complications, hospital stay duration, and 3-year mortality.
The time to flatus was defined as the time to the first audible bowel sound during routine postoperative care. The nurses or assistants checked the patients hourly for bowel sounds and asked them to note the time to flatus and defecation and then inform them. Pain was assessed using a VAS ranging from 0 (no pain) to 10 (extreme pain). The pain assessment was carried out by an assistant doctor who was unaware of the clinical trial, as part of the clinical care given to all patients (6, 12, 24, and 48 h postoperatively). The hospital stay was defined as the number of nights spent in the hospital after surgery. The period of tolerating a solid diet was measured from the time the patient awoke from anesthesia until the time they were able to consume solid food (i.e., any food requiring chewing) without vomiting or experiencing significant nausea within 4 h of consuming the meal. Lying in bed time was defined as the time from returning to the bed in the ward after surgery until the first ambulation. Intraoperative complication includes, but not limited to, hypotension, cardiovascular event, severe subcutaneous emphysema, etc. Postoperative complication includes, but not limited to, nausea, vomiting, abdominal distension, hypotension, dizziness, fever and ileus, etc. A sample of 5 mL of peripheral blood was collected before induction of anesthesia and 0.5 h after surgery. We centrifuged the blood specimen at 3000 rpm for 5 min, and the supernatant was stored in the refrigerator at -80 °C. Enzyme linked immunosorbent assay (ELISA) was used to measure the stress hormone cortisol in the serum, a biomarker of stress responses. Blood glucose levels were also measured preoperatively (just as anesthesia begins) and postoperatively (30 min post operation). Additionally, analgesic requirements were assessed using electronic records, and the total consumption of sufentanil was calculated. In addition, we assessed postoperative emotional states of patients using the Hamilton Anxiety Scale (HAMA) [16] and the Patient Health Questionnaire-9 (PHQ-9) [17] after surgery on the third postoperative days. All patients were followed for at least 3 years to obtain the mortality rates.
Detection of serum cortisol by ELISAThe detection of serum cortisol by ELISA has been described before [18]. Before determination, the serum supernatant was reconstituted in 4 °C ice water, then centrifuged again at 3000 rpm for 5 min. The corticosterone levels were determined by using an ELISA kit (Abbott, U.S.) according to the manufacturer's instructions. The procedure was strictly adhered to, and the absorbance (OD values) of each well was determined at 450 nm wavelength. The multinomial quadratic regression equation of the standard curve was calculated using the concentration of the standard material as the longitudinal coordinate and the OD value as the transverse coordinate. The OD value of the sample was replaced by the equation, and the concentration of the sample was calculated, multiplied by the dilution multiple, which represents the actual concentration.
Statistical analysisThe average time to flatus of CRC patients at our center was calculated using our preliminary experimental results. Based on our pilot findings, the average time to flatus was about 27 h in the control group versus about 20 h in the SGB group as more than 25% reduction in time after SGB procedure. On the basis of our institutional data, a sample size of at least 31 patients per arm was calculated to have a power of 0.80 and a significance level of 0.05. Finally, we included 34 patients in each group to account for possible dropouts. Variables were reflected as means with standard error of mean or interquartile range. In the case of continuous variables, t-tests were used when they were normally distributed, otherwise, Mann–Whitney U tests were used. The χ2 test was used for comparison of categorical variables and 2-way ANOVA for repeated measures was performed for comparisons between the groups in time. Nonparametric data were analyzed using Kruskal–Wallis tests. The statistical analyses were performed using GraphPad Prism version 8.0 (GraphPad Software, San Diego, California). P < 0.05 were considered significant.
留言 (0)