
記住我

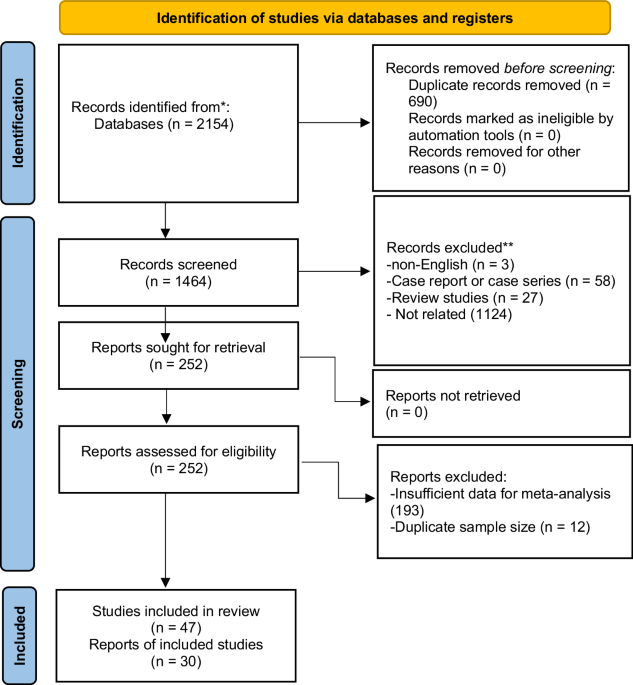
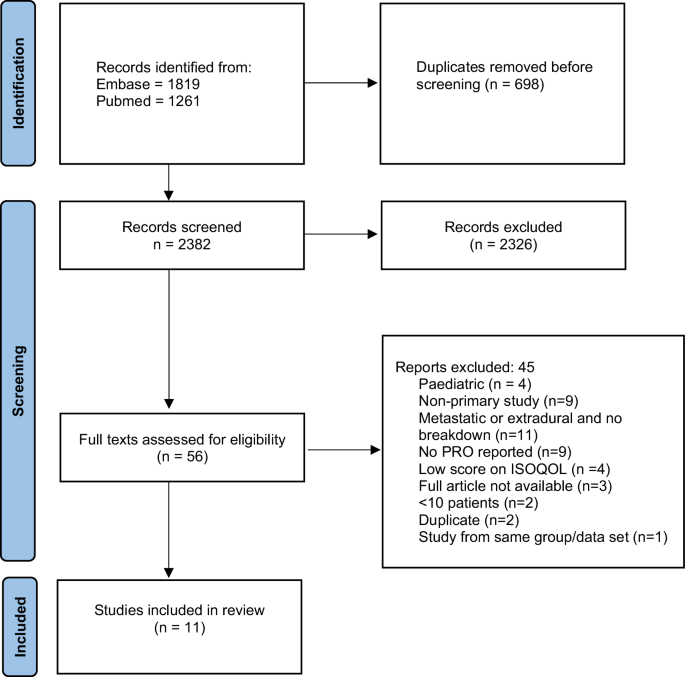

The literature search identified 2382 studies following removal of duplicates. Following abstract screening, 56 studies remained for full text review. A total of 11 studies were included in the final analysis. Figure 1 demonstrates this study’s PRISMA flowchart with reasons for exclusion after full text review.
Fig. 1: PRISMA flow diagram of search results.
PRISMA flow diagram demonstrating search results, excluded studies, and included studies.
Study characteristicsNearly half of included studies originated from North America (n = 5). The remainder were from Europe (n = 3), Japan (n = 2), and one study from South America. The total number of PSIT patients represented across these studies was 737 (range: 16–149). Of these, 392 were EMTs and 345 were IMTs. One study contained a control group in the form of brain tumour patients [12]. The commonest pathology was schwannoma (n = 190). The mean participation rate in these studies was 74% (range 43–97%). Where the mean age of the patients was reported, (n = 8 studies), the average age of all patients in this review was 44.6 years. Overall, 51.7% of patients were female.
Four studies were focused on EMT, five studies were on IMT, and two studies included both subtypes. In the two studies reporting on both pathological subtypes, outcomes were not broken down by EMT/IMT status. There were 4 cross sectional and 7 longitudinal cohorts. The longitudinal cohorts all assessed pre- and post-operative PROs. All studies were surgical series, and no study evaluated the impact of chemotherapy/radiotherapy. PRO assessments were collected through several different routes. This included completion by the patient online [12], in clinic [13,14,15,16], by mail [17,18,19], in person asked by an interviewer [20], via phone [21], or by a combination of methods [22]. For a full list with abbreviations of PRO tools used, see Table 2.
Table 2 Summary of study findings.Risk of bias in studiesThe results for risk of bias assessments are presented in Supplementary Appendix 3.
Quality of PRO reporting within studiesAll studies included in this review achieved satisfactory scoring on the modified ISOQOL reporting standards. Due to heterogeneous reporting, varied levels of granularity, and varied PRO tools used, quantitative meta-analysis of findings was not possible. A qualitative synthesis of findings was therefore used.
Outcomes reported in EMTs Global healthFor EMTs, numerous studies identified an improvement in overall quality of life post-operatively at 12 months [13, 21] and beyond [22]. Post-operative overall QoL as measured using the Visual Analogue Scale (VAS) component on the EQ-5D was middle to high [13]. Although ongoing presence of pain was associated with worsened QoL, the strongest predictors of this were bladder/bowel symptoms and motor deficits [13]. Presence of sensory deficits alone did not significantly influence overall QoL [13]. Where studies attempted to identify the impact of tumour location, cervical tumours were associated with the greatest improvement post-operatively [22].
Physical healthIn all EMT studies, significant improvement in post-operative pain at 12-months follow up were reported across a variety of reporting tools (Table 2) [13, 14, 21, 22]. This improvement occurred as early as <1-month follow-up [14] and was not associated with age, tumour type, or tumour location [13].
Physical functioning also improved post-operatively at 12-months measured using the Oswestry Disability Index (ODI), Neck Disability Index (NDI), or the Physical Component Score (PCS) component of the SF36 [21]. However, unlike the early improvement in pain reported above, an initial worsening in the ODI as well as the mobility and self-care EQ5D domains at <1-month was reported by Viereck et al, followed by improvement at all subsequent follow ups [14]. Assessed using the Brief Pain Index (BPI) and the MD Anderson Symptom Inventory (MDASI), Newman et al also reported significant improvements in physical health, general activity, walking ability, and sleep quality at >12-months [22].
Social healthSocial health in EMTs was assessed in two studies. Participation in usual social activities as measured using the EQ5D appeared to significantly improve by 3–12 months (Table 2) [14]. This change was sustained beyond 12 months as measured using the BPI and MDASI [22].
Mental healthSelf-reported depression and anxiety was measured using a variety of general tools including the EQ5D, SF36, BPI, and the MDASI (Table 2). In a cohort of 44 EMTs, Viereck et al reported a improvements in the anxiety and depression scores of the EQ5D post-operatively as early as <1-month, and at 1–3 months, 3-12 month, and > 12-month follow up [14]. Likewise, Chotai et al reported a significant improvement in overall mental health in a group of EMTs at the 12 month mark using the Mental Component Score (MCS) of the SF36 [21]. Overall mood and enjoyment of life also demonstrated significant improvement as measured using the BPI and MDASI at long term follow up [22].
Outcomes reported in IMTs Global healthIn contrast to EMTs, a general pattern of worsened overall QoL was reported for IMTs. Compared to national averages, overall SF36 scores were worse at a mean follow of 5.4 years post-operatively [17]. These were significantly associated with the existence of pain, as measured using the Neuropathic Pain Symptom Inventory (NPSI). In another cohort, although the minimal clinically important difference (MCID) in the EQ5D was reached in 28% of IMTs, the group average did not show a statistically significant improvement at a median of 12 months of follow up [16]. Ependymoma pathology was trending towards reaching MCID. In contrast to findings in EMTs by Newman et al, cervical location was associated with worsened outcomes in IMTs [22].
Three studies included ependymoma patients only. In a study of 16 ependymoma patients by Nakanashi et al. no improvement in total SF36 score post-operatively was identified at a follow up of 6–12 months [20]. At a median follow up of 5.4 years, Butenschoen et al noted an overall high disease burden and perceived disability in ependymoma patients as measured on the mean utility EQ5D [19]. A worsened outcome was associated with a worse neurological deficit as measured with the MMG, not being able to return to usual physical activities, and female gender. Acquaye et al compared ependymoma pathology in spinal versus cranial patients. They note a significantly higher symptom burden and symptom frequency in spinal ependymoma patients as well as overall worse SF36 scores as compared to cranial patients.
Physical healthIn contast to EMTs, improvements in pain were not as prevelant in IMTs. At a mean follow-up of 5.4 years, 56% of 85 IMTs were found to have remaining moderate to severe pain measured using the NPSI [17]. The paresthesiae/dysesthesia domain of the NPSI was significantly worse than other pain categories (burning, pressing, or paroxysmal). Acquaye et al found the commonest reported symptom in ependymoma patients being numbness/tingling (reported by 59% of 149 patients) as well as pain (reported by 46%) [12]. Tumour pathology was found to potentially influence the type of pain perceived with astrocytomas being associated with burning pain and hemangioblastomas being associated with paroxysmal pain [17]. The worsening pain scores were independent of improvements in functional status, as measured using the Japanese Orthopoedic Association score (JOA).
For overall physical health, at 22 months median follow up, Xiao et al reported no significant improvement in mean Pain Disability Questionnaire (PDQ) scores despite 28% reaching MCID [16]. Improvements were associated with ependymoma pathology and thoracic location, while a worsening of the PDQ was associated with cervical location and the development of cerebrospinal fluid leak post-operatively. Acquaye et al reported that the PCS of the SF36 was worse in spinal ependymoma than cranial ependymoma patients [12]. They also identified specific physical symptoms that were reported frequently by ependymoma patients to include fatigue (46%), weakness (47%), and sexual dysfunction (39%). Butenschoen et al reported the worst SF36 domains for ependymoma patients being vitality and role limitations due to physical constraints [19]. These were significantly worse in patients reporting difficulties returning to any sporting activity.
Social healthCompared to brain ependymoma patients, spinal patients demonstrated reduced return to work and participation in usual activities [12]. There was a general shift from full time employment pre-op to part time or early retirement. Commonest reasons reported for this was persistent pain or physical stress. Individual level participation in sports remained stable, although overall frequency of sporting sessions reduced as well as a reduction in participation in group sports. Commonest reported limitations for participation in sports were pain, coordination problems, motor deficits, and a fear of injury. Poorer participation in sports was associated with poorer MMG post-operatively and more extensive operative approaches ( > 5 levels or laminectomy/laminoplasty vs. unilateral laminotomy).
Mental healthIn a mixed group of IMTs [16], mean Patient Health Questionnaire 9 (PHQ-9) scores did not significantly differ between pre- and post-operative assessments (22-months median follow up). This was the only study where a dedicted mental health assessment tool was used. MCID in the PHQ-9 was reached in 16% of patients, but no predictors of improvement were identified. Compared to cranial ependymoma patients, the rates of self-reported depression were similar in spinal patients (19% vs. 15%) [12].
Outcomes reported in combined EMT/IMT cohorts Global healthTwo studies reported outcomes of EMTs and IMTs without reporting the outcomes for each pathology subgroup separately. In a mixed study of EMTs and IMTs, Bellut et al found that overall QoL was significantly improved with surgery at 3- and 12-month follow up [18]. They also identified significant satisfaction with surgery and a patient reported sense of surgery having been a useful intervention. In another combined series, Guirado et al reported a correlation with improved post-operative SF36 scores and post-operative neurological status as measuring using the MMG and the Aminoff-Logue Scale (ALS) [15]. Of note, in both studies where a mixed population is reported, the majority of pathologies were EMTs.
Physical healthAt a mean of 20 months follow up, Guirado et al reported a worsened PCS component of the SF36 in a combined EMT/IMT cohort which was associated with myelopathy subscales of the ALS (gait, micturition, and bowel) and with poorer post-operative MMG. The SF36 vitality domain was significantly associated with the bowel domain of the ALS. However, in another combined series, Bellut et al reported improvements in axial and peripheral pain measured using the Core Outcome Measures Index (COMI) as early as 3 months follow up, and this was sustained at 12-months follow up [18].
Social healthIn mixed IMT and EMT studies, overall social disability as measured using the COMI improved by 3 months [18], however work disability improvement was only detected at 12 months [18]. Overall improvement in social functioning as measured using the social functioning domain of the SF36 was associated with improved MMG post-operatively [15]. Prescence of bowel symptoms on the ALS was associated with a poorer role functioning score on the SF36 [15].
Mental healthIn a mixed cohort of IMTs and EMTs, presence of myelopathic symptoms as measured using the ALS was associated with poorer scores in the MCS of the SF36.
留言 (0)