
記住我






WHAT THIS EVIDENCE ADDS
Current evidence: Numerous research studies have incorporated 3-dimensional instrumented gait analysis (3D-IGA) for children with impairments affecting walking. This research has been broadly summarized in a scoping review regarding the use of 3D-IGA for the management of walking in children with cerebral palsy as well as 2 systemic reviews of the clinical efficacy of instrumented gait analysis.1-3
Gap in the evidence: The scoping and systemic reviews do not provide guidelines for pediatric physical therapists and associated clinicians about how or when to incorporate the use of 3D-IGA in the care of children with cerebral palsy.
How does this study fill this evidence gap? These are the first clinical practice guidelines related to use of 3D-IGA in the management of walking for children with cerebral palsy. Guidelines address whether assessment that includes 3D-IGA changes treatment decisions and produces better outcomes compared with a plan of care that does not include 3D-IGA. These guidelines also address what information 3D-IGA provides independent from typical clinical evaluations and if 3D-IGA can be an appropriate tool to evaluate the biomechanical effects of interventions aimed at improving walking function. Finally, recommendations for the equipment, staffing, and reporting for 3D-IGA are described.
Implication of all the evidence to clinicians: Pediatric physical therapists and associated clinicians now have guidance on when assessment with 3D-IGA is appropriate for children with cerebral palsy based on evidence that has been rated on quality and summarized.
Summary of Action Statements B. Informing Orthopedic Surgical Interventions: Physical therapists, physicians, and associated clinicians should recommend 3D-IGA when a child with CP who walks with or without an assistive mobility device is considered for orthopedic surgery to improve gait. (Evidence Quality: II, Rec. Strength: Moderate) B. Gait Deviation Analysis: Physical therapists, physicians, and associated clinicians should recommend 3D-IGA when a child with CP presents with gait dysfunction and there is a need to identify, quantify, and differentiate deviations among individual segments/joints and planes (sagittal, coronal, and transverse). (Evidence Quality: II, Rec. Strength: Moderate) B. 3D-IGA to Evaluate Biomechanical Outcomes: When physical therapists, physicians, and associated clinicians need to evaluate biomechanical aspects of gait related to an intervention for children with CP, they should recommend baseline and post-intervention 3D-IGA. (Evidence Quality: III, Rec. Strength: Weak upgraded to Moderate for consistent results) C. Non-Surgical Interventions: Physical therapists, physicians, and associated clinicians may recommend 3D-IGA to inform non-surgical interventions for children with CP with gait dysfunction whose progress from rehabilitative interventions and conservative management has plateaued or shown substantial deterioration. (Evidence Quality: III, Rec. Strength: Weak) P. Instrumented Gait Analysis Equipment: When 3D-IGA is recommended for children with CP to assess gait patterns, physical therapists, physicians, and associated clinicians should recommend gait laboratories that can collect 3-dimensional kinematic, kinetic, and electromyography (EMG) data. (Evidence Quality: V, Rec. Strength: Best Practice) P. Interdisciplinary Team Approach: When 3D-IGA is recommended for children with CP to assess gait patterns, physical therapists, physicians, and associated clinicians should recommend a 3D-IGA laboratory that has an interdisciplinary team approach. (Evidence Quality: V, Rec. Strength: Best Practice) P. Comprehensive Reports: When 3D-IGA is recommended for children with CP to assess gait patterns, physical therapists, physicians, and associated clinicians should recommend 3D-IGA laboratories that provide comprehensive, timely, and interdisciplinary reports including: (a) referral source and reason for referral; (b) diagnosis including Gross Motor Function Classification System (GMFCS) level; (c) primary concerns or goals of the child, family, and health care professionals including physical therapists; (d) pertinent past medical history; (e) current orthoses and adaptive equipment; (f) findings of physical exam; (g) documentation of 3D-IGA results; (h) limitations in conducting the assessment and or technical issues; (i) interpretation of findings by licensed clinician(s) (eg, MD and/or PT); and (j) suggestions for interventions by licensed clinician(s). (Evidence Quality: V, Rec. Strength: Best Practice) INTRODUCTIONThe Academy of Pediatric Physical Therapy (APPT) of the American Physical Therapy Association (APTA) supports the development of evidence-based clinical practice guidelines (CPG) as a service to its members. The APPT appointed the Guideline Development Group (GDG) to develop a CPG for physical therapists (PTs) and other healthcare providers involved in the management of children with cerebral palsy (CP) describing the utility of 3-dimensional instrumented gait analysis (3D-IGA) in the clinical management of children who walk with dysfunction related to (CP). The GDG included pediatric PTs, clinical researchers, and a biomedical engineer; content experts in the areas of pediatric PT, gait/motion analysis, and systematic review methodology.
Purpose of the CPGThis CPG aims to help PTs, physicians, and associated clinicians involved in the care of children with CP to determine how 3D-IGA can be used to guide decision making about potential examinations and interventions, and to improve clinical outcomes. The guideline is focused on the use of 3D-IGA in the management of children with CP who can walk with or without an assistive mobility device and who have gait dysfunction. Throughout this guideline, 3D-IGA refers to analysis of 3-dimensional kinematic data from a motion capture system; it may be accompanied by related measurement technologies including force plates (kinetics) and electromyography (EMG), often done simultaneously.
Scope of the GuidelineThis CPG aims to address questions for PTs, physicians, and associated clinicians with regard to the utility of 3D-IGA in the clinical management of children who walk with dysfunction related to CP. PTs may be asked to consult with families about when 3D-IGA might be appropriate. This CPG is focused on understanding how and when 3D-IGA can be useful in the clinical decision-making process. This CPG does not consider the specific testing conditions or technological details to analyze a specific child’s walking performance. This CPG suggests (a) the minimum set of equipment/instruments that should be available for 3D-IGA for management of walking in children with CP; (b) the characteristics of the personnel and laboratories that perform 3D-IGA; and (c) what should be included in a comprehensive 3D-IGA report. The reader should note that the terms “walking” and “gait” are interchangeable except when referring to industry-related terms defined in the glossary, specific tests, processes and organizations.
Statement of IntentThis CPG is intended to help clinicians learn about the utility of gait analysis for the clinical management of children with CP. This CPG also intends to guide and inform PTs, family members, educators, physicians, orthotists, engineers, biomechanists, kinesiologists, and other healthcare providers about the utility of 3D-IGA in the management of children who walk and with CP. This CPG was not developed to be construed as or to serve as a standard of care, and adherence to the action statements will not guarantee a successful outcome with every child. Guideline action statements may not be inclusive of other appropriate methods of care aimed at the same outcomes or exclude other acceptable methods of care aimed at the same results. This CPG is a summary of action statements that are supported with current published evidence or standards of care. The CPG has been reviewed by an interdisciplinary group of interested people representing physical therapy, orthopedic surgery, engineering, kinesiology, educators, parents, and adults with CP. The action statements are guidelines only, not mandates. The ultimate decision or judgment regarding a particular clinical procedure or a specific plan of care must be made by the appropriate health care practitioner(s) in consultation with the child and family with regard to the child’s clinical data, the diagnostic and treatment options available, the clinician’s scope of practice and clinical expertise, and the child’s values, expectations, and preferences. However, it is recommended that significant departures from accepted guidelines be documented in children’s records at the time the relevant clinical decision is made.
METHODS Determining Priority ContentThe GDG conducted a needs assessment survey based on current 3D-IGA practice,1 completed a scoping review to understand the literature,2 solicited attendee feedback at the 2018 and 2019 meetings of the Gait and Clinical Movement Analysis Society (GCMAS), the primary professional organization focused on 3D-IGA in North America, and consulted with experts involved in CPG development and use of 3D-IGA in the management of children with CP.
The needs assessment survey identified the priorities of the clinical and research communities involved with 3D-IGA for children with CP.1 The survey was completed by 52 PTs and 44 other professionals involved with the care of children with CP. It informed development of the following 7 questions for the CPG relevant to the management of children with CP-related gait dysfunction: (1) When a child is considered for orthopedic surgery related to their gait dysfunction, does a plan of care that includes 3D-IGA change treatment decisions and produce better outcomes compared with a plan of care that does not include 3D-IGA? In this context, is 3D-IGA cost effective relative to other examination methods? (2) Can 3D-IGA provide information independent from typical clinical evaluations that identifies, quantifies and differentiates deviations among individual segments/joints and planes (sagittal, coronal, and transverse) underlying a child’s gait dysfunction? (3) Is 3D-IGA an appropriate tool to evaluate the biomechanical and neuromuscular effects of interventions aimed at improving walking for children with CP who walk? (4) When a child is considered for a substantial new episode of non-surgical treatment related to the child’s gait dysfunction, does including 3D-IGA when compared with not including 3D-IGA change treatment decisions and produce better outcomes following non-surgical interventions? (5) What minimum set of equipment/instruments should be available for children with CP who are referred for 3D-IGA? (6) What should be the composition and expertise of interdisciplinary personnel who plan, perform, and interpret 3D-IGA? (7) What information should be included in a comprehensive 3D-IGA report?
Literature SearchThe initial literature search for this CPG was conducted in the context of a previously published scoping review and 2 systematic reviews on the clinical efficacy of IGA.2-4 Two health sciences librarians assisted with establishing database specific optimal and reproducible search strategies to generate a comprehensive search. The initial search was completed in December 2019, was updated periodically, and included studies published through September 2022. Searches were performed using the following databases: Ovid/MEDLINE, EMBASE, the Cumulative Index to Nursing and Allied Health Literature (CINAHL), the Physiotherapy Evidence Database (PEDro), the Cochrane Database of Systematic Reviews, and the Cochrane CENTRAL database. Search terms included closely related terms, and combinations of terms: gait analysis, instrumented gait analysis, clinical gait analysis, kinematics, kinetics, electromyography, 3-dimensional motion capture, force plate, cerebral palsy, monoplegia, diplegia, athetoid, spastic, hypotonic, ataxic, gait, walking, ambulation, locomotion, child, adolescent, girl, boy, pre-school, school-age, high school, middle school, teen, youth, pediatric (Supplemental Digital Content 1 available at https://links.lww.com/PPT/A520).
Studies were eligible for inclusion in this CPG if they met the following criteria: (a) peer-reviewed research, (b) sample included children with CP (the term “children” is operationally defined as anyone up to 21 years of age), (c) investigated using 3D-IGA in treatment or assessment of gait dysfunction, and (d) in English. Exclusion criteria included: the article was a review, commentary, or conference abstract. Additional searches, including hand-searching, were performed, to identify resources for best practices in motion analysis laboratory quality and accreditation standards related to personnel, equipment, cost, and reporting.
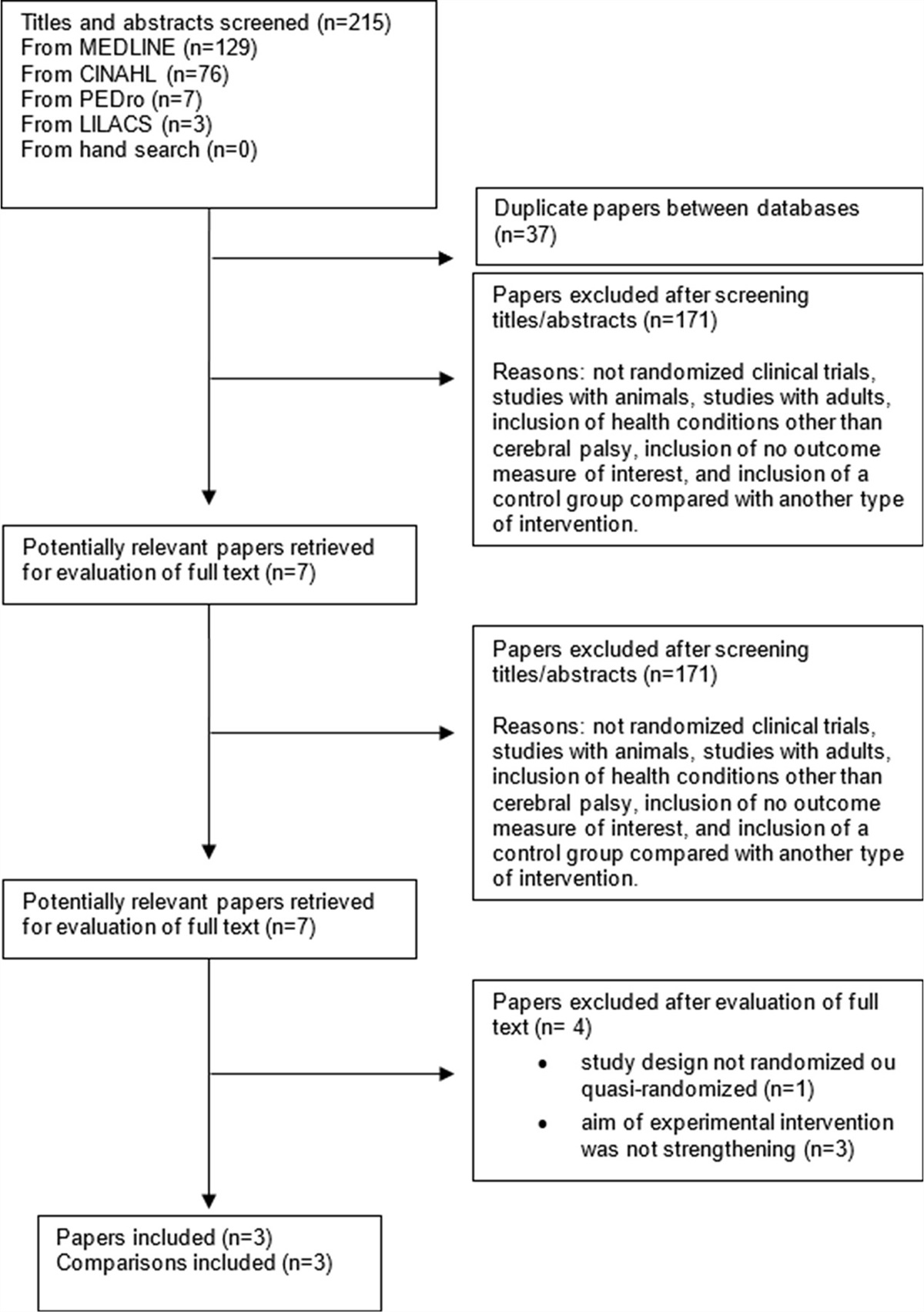
Study SelectionA literature search was defined in a scoping review and updated for the CPG in September 2022. Together 2179 citations were identified and screened for inclusion; they were simultaneously categorized regarding the CPG question to which they pertained. Reliability for inclusion and categorization were established among the 6 reviewers as described in the scoping review.2 Briefly, 6 reviewers independently reviewed and discussed 5 groups of 20 citations and abstracts to establish consensus and refine the checklist for inclusion and categorization. This was followed by independent blind assessment by pairs of reviewers for approximately half of the citations (~1050), then independent assessment of about 175 remaining citations by each of the 6 reviewers. Two authors conducted a final round of random checks of the selection and categorization judgments on over 500 citations to assure overall consistency. Overall, 969 studies were identified as relevant to 3D-IGA for the management of children with CP-related gait dysfunction; a subset of these are cited in the supporting evidence sections.
Data ExtractionData extraction for articles relevant to the CPG questions followed the procedures suggested by the APTA Clinical Practice Guideline Manual 2018.5 This included having a methodologist adapt the forms suggested in the CPG manual and from the Covidence tool (Veritas Health Innovation)6 for the various CPG questions. Along with basic design features, specific criteria to assess study quality and results were extracted. For experimental studies, pairs of GDG members extracted the data independently and discussed discrepancies. If discrepancies remained, a third GDG member assessed the study and consensus via discussion resolved the issue. For the cross-sectional and cohort studies, pairs of GDG members extracted data for 2 randomly chosen groups of 20 studies each to reach consensus on interpretation. Subsequently, GDG members individually conducted data extraction on approximately 50 remaining articles each, with ambiguities resolved by discussion with the GDG partner or a third GDG member as needed.
Critical Appraisal ProcessExperimental studies for CPG question 1, Evaluating orthopedic surgical interventions were appraised with the Critical Appraisal Tool for Experimental Interventions (CAT-EI V1.2).5 Two GDG members independently appraised study quality with 93% reliability on the 24 orthopedic surgical intervention studies. For CPG question 2, independent information from clinical measures, the Appraisal tool for Cross-Sectional Studies7 was applied to 20 articles randomly chosen from the included studies. Reliability of over 90% was achieved on the individual items and total score for these articles amongst the 4 reviewers. The remaining 109 cross-sectional studies were appraised by 1 of the reviewers, with discussion among pairs of reviewers to categorize uncertainties. Literature addressing CPG question 3, 3D-IGA to evaluate biomechanical outcomes was not rated for the quality of the research design. That CPG question aimed to describe the utility of using 3D-IGA as a measurement tool to quantify changes, not to determine the effectiveness of the study’s intervention. Hence, we assessed whether any of its 3D-IGA outcome measures were responsive to the intervention by assessing whether at least 1 3D-IGA measure supported a statistically significant difference. This methodological choice is discussed further in the Supporting Evidence for Action Statement III. For CPG question 4, nonsurgical interventions, the relevant literature consisted of intervention studies, thus, they were assessed using the CAT-EI in the same method as for CPG question 1. Since the 5th, 6th, and 7th CPG questions addressed standards for best practices in equipment, personnel, and reporting, evidence was derived from clinical perspectives, accreditation, and other guidance statements rather than from empirical studies.
Of the 24 orthopedic surgical intervention publications, 2 were high quality, 10 acceptable, 7 low quality, and 5 were unacceptable based on their CAT-EI ratings. Many of these studies were multi-year retrospective investigations of patient registries from large and well-established gait labs. As such, randomization, a-priori power analyses or inclusion of a control group were not used. Most studies included rigorous inclusion/exclusion criteria, standardized and validated protocols for measuring and analyzing data, and experienced interdisciplinary teams to conduct the investigation and interpret the data. Most studies minimized recruitment bias by including a consecutive sample of children referred to individual labs. There was clear adherence to the established protocol as methods describing the biomechanical models for processing 3D-IGA data were either detailed or referenced.
The 129 studies on deviations of segments/joints and planes (sagittal, coronal, and transverse) were assessed using the Appraisal Tool for Cross-Sectional Studies7 with the following adaptations. Three items were assigned a value of Not Reported as they did not apply to the descriptive nature of the studies: were measures undertaken to address and categorize non-responders? Does the response rate raise concerns about non-response bias? If appropriate, was information about non-responders described? The item regarding funding sources was reverse coded so that authors who reported funding without conflicts of interest received a positive score. Given these adaptations, the total possible score was 17 rather than 20; 90 were rated as high quality, 36 were moderate, and 3 were low quality.
Only 2 studies (4 publications) addressed CPG question 4, nonsurgical interventions. Three articles were rated high quality based on the CAT-EI, and 1 was rated as acceptable; inter-rater agreement for these articles was 97%.
Determination of Action StatementsThe BRIDGE-Wiz software8 was used to assure that action statements aligned with the Institute of Medicine’s standards for transparency through its process and the template of headings.9
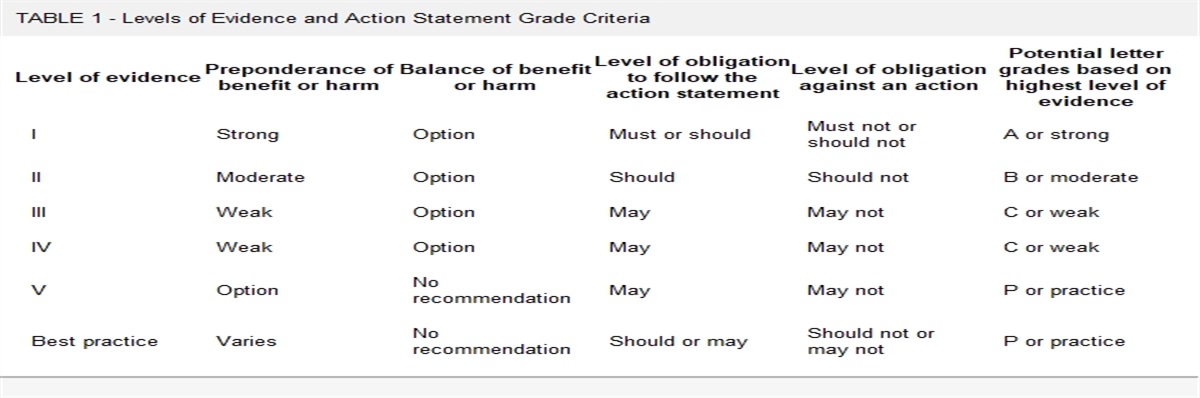
The evidence quality and grade for each action statement were assigned through consensus of the GDG (Tables 1 and 2) based on the APTA Clinical Practice Guideline Manual.5 This included consideration of critical appraisal of results, the extent to which the set of available studies specifically answered the CPG question (indirectness as defined by GRADE), consistency of results, and volume of supporting evidence.10
TABLE 1 - Levels of Evidence and Action Statement Grade Criteria Level of evidence Preponderance of benefit or harm Balance of benefit or harm Level of obligation to follow the action statement Level of obligation against an action Potential letter grades based on highest level of evidence I Strong Option Must or should Must not or should not A or strong II Moderate Option Should Should not B or moderate III Weak Option May May not C or weak IV Weak Option May May not C or weak V Option No recommendation May May not P or practice Best practice Varies No recommendation Should or may Should not or may not P or practiceSystematic review of prospective cohort studies
High-quality prospective cohort study (b)
Systematic review of high-quality diagnostic studies
High-quality diagnostic study with validation (c)
Systematic review of high-quality cross-sectional studies
High-quality cross-sectional study (d)
Systematic review of prospective cohort studies
High-quality prospective cohort study
II. Evidence obtained from lesser-quality diagnostic studies, prospective studies, or RCYs (eg, weaker diagnostic criteria and reference standards, improper randomization, no blinding, less than 80% follow-up)Systematic review of high-quality cohort studies High-quality cohort study (b)
High-quality outcomes research High-quality quasi-experimental study (g)
High-quality single-subject design (h)
Lower-quality RCT
Systematic review of retrospective cohort studies
Lower-quality prospective cohort study
High-quality retrospective cohort study
Consecutive cohort study
Outcomes study or ecological study (f)
Systematic review of exploratory diagnostic studies or consecutive cohort studies
High-quality exploratory diagnostic study
Consecutive retrospective cohort study
Systematic review of studies that allows relevant estimate
Lower-quality cross-sectional study
Systematic review of lower-quality prospective cohort studies
Lower-quality prospective cohort study
III. Case-controlled studies or retrospective studiesSystematic review of case-controlled studies
High-quality case-controlled study
Outcomes study or ecological study (f)
Lower-quality cohort study
Lower-quality retrospective cohort study
High-quality cross-sectional study case-controlled study
Lower-quality exploratory diagnostic study
Nonconsecutive retrospective cohort study
Local nonrandom study High-quality cross-sectional study IV. Case series Case series Case series Case-controlled study Lower-quality cross-sectional study V. Expert opinion Expert Opinion Expert Opinion Expert Opinion Expert Opinion Expert Opinion(a) High quality includes RCT>80% follow-up; blinding; appropriate randomization procedures. (b) High-quality or dramatic effect cohort study includes >80% follow-up. (c) High-quality diagnostic study includes consistently applied reference standard and blinding. (d) High-quality prevalence study is a cross-sectional study that uses a local and current random sample or censuses. (e) Weaker diagnostic criteria and reference standards, improper randomization, no blinding, <80% follow-up may add threats to bias and validity. (f) High-quality outcome or ecological studies use instrumental variable(s) or other control for confounding factors. (g) High-quality comparative study without random assignment to groups. (h) Must have a minimum of “a” and “b” phase.
A CPG Advisory Board consisted of interested parties with experience in 3D-IGA, including professionals, children, and families of individuals who experienced 3D-IGA (Supplemental Digital Content 2 available at https://links.lww.com/PPT/A521). Roles of the Advisory Board were to review and comment on the CPG scope, CPG questions, first draft review, and second revised draft prior to publication. The second draft was posted for public comment through the APPT Milestones newsletter. An electronic newsletter was sent to APPT members, literature appraisers, and clinicians who inquired about the CPG during development. The GDG recorded and considered comments from each round of reviews to edit the CPG prior to final submission for publication.
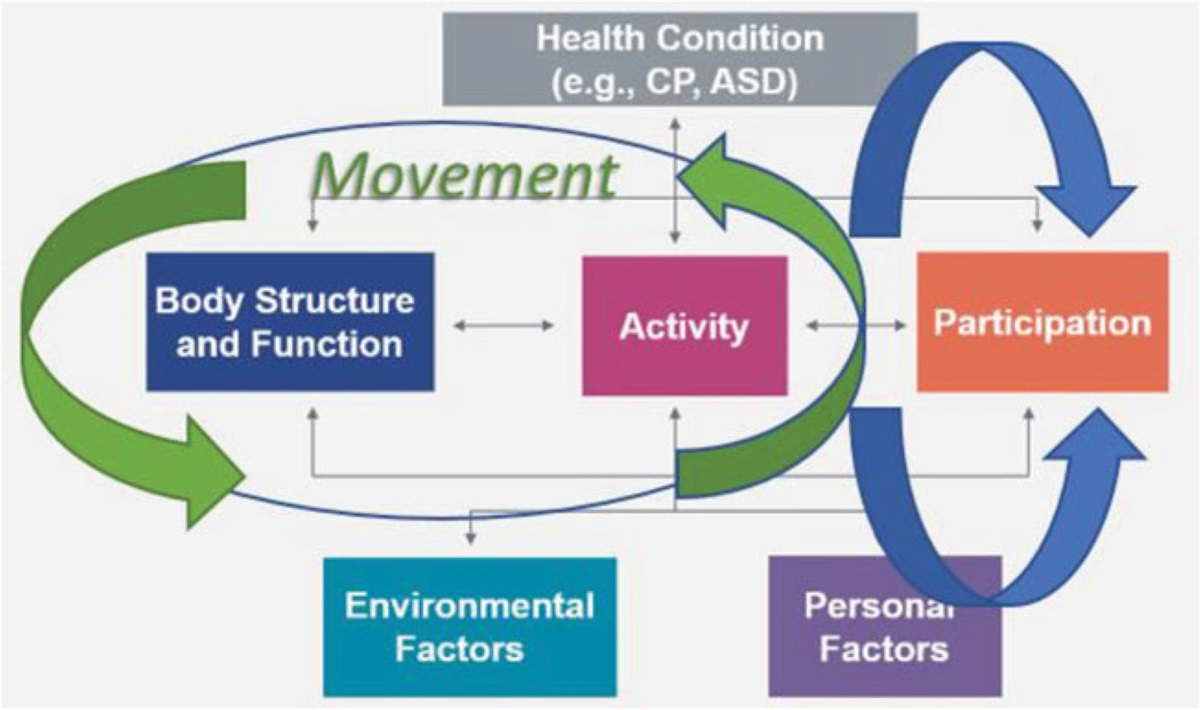
BACKGROUND Cerebral PalsyCerebral palsy describes a group of disorders in the development of movement and posture, causing activity limitations and participation restrictions, attributed to non-progressive disturbances that occurred in the developing fetal or infant brain.11 CP is the most common neuromotor disorder among children with an overall prevalence 2.1 cases per 1000 live births.12 The motor disorders seen in children with CP are often accompanied by disturbances of sensation, perception, cognition, communication, behavior, and seizure disorders and by secondary musculoskeletal complications.11,13,14 CP can be described by the types of motor impairment including spastic, dystonic, dyskinetic, ataxic, hypotonic, rigid, or mixed type15 or according to the distribution of impairments as unilateral including hemiplegia, bilateral including diplegia, or total-body involvement (eg, quadriplegia, tetraplegia).14 Functional motor skills of children with CP are also classified using the Gross Motor Function Classification System (GMFCS),16 a 5-level ordinal measure with foci on posture and mobility. Level I represents the highest functional motor ability and Level V the lowest; motor skills expected for various age groups are described for each GMFCS level.16,17
Children with CP often have complex gait dysfunction which can limit activities and participation in family, school, social, and workplace settings and may result in significant deformities that require complex medical, rehabilitative, and surgical interventions. Approximately, 70% of persons up to age 21 years,18,19 walk with or without an assistive mobility device (ie, walker, crutches, etc.). Altered walking may result in tripping/falling, fatigue, limited participation in activities, joint pain, segment/joint deformities and premature development of osteoarthritic changes.20-22 Children with CP and their families often have concerns about the appearance and/or quality of their walking (eg, limping, stiff knee(s), flexed knee(s), in-toeing, toe walking, etc.), tripping and falling, their speed and endurance, as well as pain.23-25 Gait patterns in children with CP vary depending on the type of CP, distribution of impairments (hemiplegia, diplegia, and quadriplegia), severity, available range of motion and flexibility, strength, muscle tone involvement, selective control, dynamic balance, involvement at joints, segments and planes (sagittal, coronal, and transverse), and associated orthopedic deformities. Atypical gait pattern descriptions in children with bilateral and unilateral involvement may involve sagittal plane deviations26-28; however, multi-segment/joint deviations in the coronal and transverse planes as well as additional compensatory gait deviations can further affect gait pattern.29-32 Common gait patterns seen in children with CP include, but are not limited to:
Equinus gait: the foot/ankle is in plantar flexion resulting in toe walking. Jump gait: the foot/ankle is in plantar flexion and the knees are flexed. Apparent equinus gait: toe walking due to knee flexion, not excessive ankle/foot plantar flexion. Crouch gait (with and without inflexible knee): the hips and knees are flexed and the ankles are dorsiflexed, or the forefoot is dorsiflexed relative to the hindfoot (ie, flatfoot with midfoot instability) in stance. Asymmetrical gait: may include some combination of gait patterns. Scissor gait: legs cross when walking which can come from increased internal hip rotation or hip adduction. Rotational malalignment: excessive femoral anteversion or retroversion and/or tibial internal or excessive external torsion and/or foot malalignment resulting in either in-toeing, out-toeing, or even a neutral foot progression angle (ie, miserable mal-alignment, or pelvic rotation asymmetry). Instrumented Analysis of GaitThere are various ways to assess gait dysfunction in children with CP including observational analysis of gait, standardized rating scales, 2-dimensional (2D) digital video recording, mobile device software applications, temporal-spatial measurement of footfalls, use of isolated body worn sensors, eg, foot pressure sensors or inertial sensors, and 3D-IGA. Unlike simpler forms of analysis, such as observational analysis or 2D motion analysis, only 3D-IGA provides a comprehensive analysis and assessment of typical and pathological walking. 3D-IGA is used to identify specific gait deviations and possible causes of atypical gait patterns, analyze how specific gait deviations influence function, understand typically developing walking, guide decision making about intervention strategies, and evaluate treatment outcomes.33-35
3D-IGA provides detailed information on kinematics (spatiotemporal parameters, joint positions, and motions), and often includes simultaneous capture of kinetics (joint forces, moments, and powers) in the child without assistive devices or external support and muscle activity (via EMG). 3D-IGA measures sagittal, coronal, and transverse plane motions and accounts for the relative positions of the joints and segments in 3D. 2D observational analysis is neither sensitive nor reliable enough to assess the complex gait patterns of children with CP.36,37 2D gait analysis cannot account for movements not aligned with the point of view. For example, the sagittal plane position and motion of the knee will be underestimated if there is simultaneous internal hip rotation, a common walking problem in persons with CP. In the frontal plane, with internal hip rotation and knee flexion, 2D analysis improperly identifies this situation as valgus. 3D gait analysis defines joint and segment angles in all 3 planes of motion and thus documents anatomically relevant joint angles.
Optical motion capture remains the preferred technology for generating 3D kinematics. Recent technology advances have led to other devices, such as inertial measurement units and markerless motion capture systems. However, these technologies are still developing and require further assessment before use in clinical 3D kinematics analysis. 3D kinematic analysis traditionally uses active or passive reflective marker set(s) and optical cameras to track the 3D location of the marker trajectories over the course of movement. A biomechanical model then uses the marker positions to determine the 3D segment position and orientation, and joint angles are derived from the orientation of relevant segments.38 Kinematic data provide dynamic angular measurements of the different joints and body segments across the gait cycle. The kinematic data for each segment/joint and plane (sagittal, coronal, and transverse) can be displayed as a series of graphs for a single (or average) gait cycle. In addition, spatiotemporal gait parameters can be calculated to include measurements of gait speed, step and stride length, step width, and cadence.
Kinetic analysis requires that at least 1 force platform be included in the 3D-IGA setup to measure 3D ground reaction forces. Kinetic data are computed using inverse dynamics and are possible when kinematic data are collected synchronously with force plate data. The most commonly used kinetic data in the assessment of gait dysfunction in CP are the sagittal and coronal plane hip, knee and ankle joint moments, and powers. Kinetic data are difficult to collect when children have step-lengths too short to have 1 foot on the plate at a time. Kinetic data also cannot be calculated when children use assistive mobility devices that share the load of body weight (unless the assistive devices are also instrumented). The kinetic data for each joint can also be displayed as a series of graphs of a single gait cycle.
Electromyography is used to measure muscle activity that underlies motion. EMG uses sensors placed over the surface of target muscles (ie, surface electrodes), or sensors inserted within the targeted muscles (ie, fine wire electrodes), to record electrical signals from activated muscle fibers. For children with CP, 3D-IGA typically uses surface electrodes. EMG is the only way to confirm what and when muscles are contracting during walking. EMG combined with 3D motion analysis system is used to measure muscle activation and timing during walking. The pattern, timing, and amplitude of muscle activation can be displayed as a set of graphs for a single or series of gait cycle(s).33,39-42
Clinical Management of Children with Cerebral PalsyThere are no curative treatments for the neurological disturbances leading to motor dysfunction associated with CP, either through surgical, pharmaceutical, or other known methods. The current management of movement limitations from CP includes medical or surgical treatment, orthoses, and rehabilitation. Medical management of seizures and spasticity may involve oral medications, intrathecal medications, or injections. Orthopedic surgical procedures to address contractures, bony alignment issues, spasticity, and pain, include muscle/tendon lengthenings/releases and transfers, osteotomies (femur and tibia rotations, foot, extension osteotomies), joint fusion, selective dorsal rhizotomy, pelvic and femur osteotomies for hip subluxation, and scoliosis surgeries.43
Rehabilitation for children with CP includes a wide range of approaches, such as therapeutic exercise and activities, hands-on and manual techniques, bracing, serial casting, electrical stimulation, mechanically assisted gait training using assistive mobility devices or treadmills, and augmented reality technology. The variability, complexity, and dynamic nature of CP contribute to individualized treatment approaches with variable outcomes. While there is growing evidence to aid the clinician in selection of primary and adjuvant interventions, including recent systematic reviews investigating the effectiveness of some therapeutic interventions,43-45 comprehensive rehabilitative decision making for children with CP remains poorly studied. This CPG focuses on the use of 3D-IGA to enhance the overall management of children with CP and have gait dysfunction. The CPG does not describe or assess the efficacy of specific physical therapy interventions for children with CP.
ACTION STATEMENTS Action Statement I: Informing Orthopedic Surgical InterventionsB. Physical therapists, physicians, and associated clinicians should recommend 3D-IGA when a child with CP who walks with or without an assistive mobility device is considered for orthopedic surgery to improve walking. (Evidence Quality: II, Rec. Strength: Moderate)
Aggregate Evidence QualityLevel II based on 2 moderate quality randomized controlled trials (RCTs) reported in 3 publications46-48 and 8 low quality quasi-experimental studies
Benefits Conducting 3D-IGA prior to planning orthopedic surgery may identify children who will not benefit from orthopedic surgery. Conducting 3D-IGA prior to planned orthopedic surgery informs the selection of and dosing of surgical procedures to improve walking. When 3D-IGA recommendations are followed, post-operative outcomes are improved across International Classification of Functioning, Disability and Health domains. Over a lifetime, conducting 3D-IGA prior to planned surgeries may reduce the frequency and lifetime costs of surgeries. Conducting 3D-IGA prior to planned orthopedic surgery may increase family confidence in the benefits of that surgery. Risk, Harm, Cost Conducting 3D-IGA can be expensive and third-party coverage varies. Access to 3D-IGA labs may be limited in some geographic areas. Families and children may need to devote substantial time and effort for travel, to attend 3D-IGA session, to wait for data processing and evaluation, and to attend additional appointments that may delay implementation of orthopedic surgical treatment. Benefit-Harm AssessmentPreponderance of benefit
Value JudgmentsNone
Intentional VaguenessThe CPG does not endorse any brand or constellation of equipment, modeling, protocol, or evaluative processes for 3D-IGA. While 3D-IGA action statements are designed to aid surgical planning, actual surgical procedures are determined by many factors, such as child/family goals, the surgical techniques, surgeon experience, post-operative rehabilitation approaches, and intended surgical outcomes.
Role of Child/Family PreferencesFamilies should have a basic understanding of 3D-IGA processes to inform their decision making and help explain the purpose and testing process to their child. Children and families should participate in shared decision making with their clinicians regarding the outcome of 3D-IGA to establish realistic goals and expectations. Ultimately, it is up to the family, the treating surgeon and the interdisciplinary team to reconcile recommendations derived from 3D-IGA evaluation in the plan of care.
ExclusionsChildren who do not walk (GMFCS Levels IV–V), children who require gait trainers to complete 3D-IGA, children who cannot follow simple directions due to age, or children with cognitive or behavioral limitations that would prevent completion of gait analyses may not be appropriate for referral. If a child does not have goals or a prognosis to improve walking, 3D-IGA should not be used.
Quality ImprovementIntegration of 3D-IGA results with consideration of orthopedic surgery improves walking outcomes for children who walk with CP and reduces unnecessary surgeries.
Implementation and AuditShare the 3D-IGA CPG with physicians and other health care professionals to increase awareness of the action statements.
Develop a list of 3D-IGA labs in the geographic area who have physicians or surgeons affiliated with the gait lab to expedite referrals for 3D-IGA and possible orthopedic surgical interventions.
Develop consumer friendly supplements for parents and children about 3D-IGA and how it may assist in orthopedic surgical decision making.
Physical therapy documentation should include information supporting the reason for referral for 3D-IGA along with family or physician reported plans for orthopedic surgery.
Supporting Evidence and Clinical InterpretationNine studies aimed to identify whether 3D-IGA changed orthopedic surgical planning for children with CP.46,49-56 All supported that adding 3D-IGA to the clinical examination findings influenced orthopedic surgical decision making. Eight of those 9 studies addressed whether use of 3D-IGA changed the specific orthopedic surgical procedures planned, such as including or eliminating a hamstring lengthening.
Orthopedic Surgical Planning: One RCT46 compared the ultimate orthopedic surgery performed in a group that used 3D-IGA in the surgical planning algorithm to a control group that did not use 3D-IGA for surgical planning. In both groups, the ultimate surgery performed was altered from the original plan given new clinical information, such as radiographs and reassessment.46 This RCT found a significantly greater change in orthopedic surgical planning when 3D-IGA was applied than in the control condition. When 3D-IGA did not support a planned orthopedic surgical procedure, surgical procedures were eliminated more frequently than in the control group; when 3D-IGA supported a surgical procedure, surgical procedures were added more frequently than in the control group. Finally, when 3D-IGA supported previously planned orthopedic surgery, surgery occurred more frequently in the 3D-IGA group than in the control group (91% vs 70%, P < .001).
Eight studies49-56 had lower quality ratings because none included a control group for comparing orthopedic surgical treatment plans without 3D-IGA. Despite this limitation, all studies concluded that 3D-IGA altered orthopedic surgical planning. In each study, the orthopedic surgical plan for children with CP was recorded based on physical exam and qualitative visual assessment of walking. The children then underwent 3D-IGA, after which another orthopedic surgical plan was developed. Post-IGA plans differed from pre-IGA plans in all 8 studies (Table 3). In 6 studies, the initial referring physician differed from the physician making the post-IGA orthopedic surgical plan.50-54,56
TABLE 3 - Changes in Orthopedic Surgical Treatment Recommendation after 3D-IGA by Anatomy Study Type or location of orthopedic surgery Psoas Hip adductors Hamstrings Rectus femoris Gastrocnemius/soleus FDRO TDRO Cook, 200349 More Less Less More Less Less Less DeLuca, 199750 Less Less Less More More Less Less Ferrari
留言 (0)