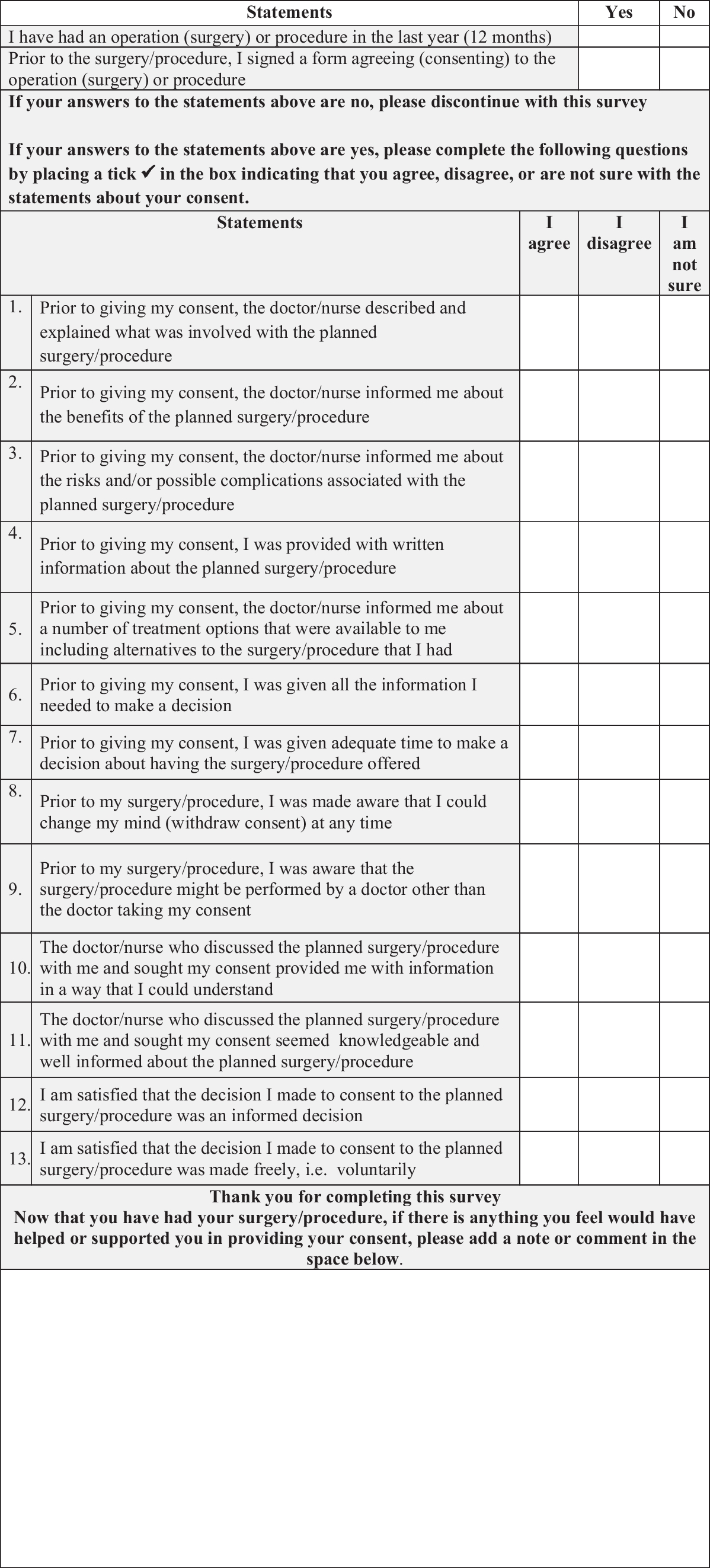
The results of this study highlight some interesting similarities and differences between members of the public thinking about a possible treatment and those patients who have actually been through the process in the past 12 months. In relation to making informed decisions, members of the public agreed that the most important information to be provided with before treatment would be information about the risks and complications associated with the proposed treatment. However, for patients who had been through the process more recently, while they felt they had been given all the information they needed to make a decision (88%) including information on risks and benefits (87%), some patients noted some aspects of their experience that could be improved. These included receiving written patient information material (PIM) in advance, being informed that the clinician obtaining consent might not be the same as the clinician performing the treatment, and receiving information on a number of treatment options that were available to them including alternatives to the treatment that they had. Members of the public would also like more details on the potential impact of the planned treatment on their life (99.2% noted this was important).
In relation to making voluntary decisions, 100% of patients felt they had made a voluntary decision. Being able to make a voluntary decision was also important to members of the public—with 85% noting that it was important that they were assured that whatever choice they made they would receive the best care possible. Thirty-eight percent of the public respondents agreed this was most important dimension in relation to questions under the voluntary criteria.
In relation to the capacity questions, the public reported that what was most important to them was that the medical team would assist them in making a decision by providing them with additional information in a way they can understand (80% agreed it was important; 50% agreed it was most important). After this, the most important thing for members of the public would be that the medical team contacted their ‘next-of-kin’ or ‘contact person’ and asked them for help in making a decision (38% noted it was important; 16% noted it was most important). Even though this term ‘next-of-kin’ is no longer a valid legal term, this was used in the survey as it is still commonly used by both staff and patients across the hospital.
It must be noted however that all of our patient respondents were people who had surgery in the last 12 months and this may be a factor in our mostly positive results from patients and hence a limitation of our study. Lattig et al. [14] found that surgeons believe that ‘patients consistently had higher expectations’ after the pre-operative discussion than the surgeons did. MacMahon et al. [15] found that more than two-thirds of patients had significantly higher expectations than their surgeons following discussions. For surgeons, responsibility for decision-making is very important [16]. In their meta-synthesis of surgeons’ perspectives, Orri et al. found that although surgeons took personal responsibility for choosing to operate on a patient, the need to share this responsibility with patients was also clearly expressed by surgeons [16]. Surgeons felt their responsibility as a personal commitment to deal with any complications that might arise during the surgery. A mutual commitment through post-operative care was thus actively sought by surgeons during the pre-operative encounters and consent conversations. Consent to surgery is taken in written from and thus explicitly given. Not all forms of consent in health and social care settings are given in written format.
A human rights–based approach to consent involves health and social care professionals engaging in shared decision-making (SDM) with patients [17]. SDM is a joint process in which a healthcare professional works together with a person to reach a decision about care, and involves choosing tests and treatments based both on evidence and on the person's individual preferences, beliefs and values.
In order to facilitate effective SDM, patients need to be informed of the risks, benefits, and possible consequences associated with the different treatment options available to them through clear and accessible discussions [17]. Engaging in real SDM however can be challenging for both clinicians and patients. Barriers to SDM can include clinician understanding of what is important to patients (e.g. the burden of treatment, treatment focusing on comfort or on living as long as possible, or side effects). Tools that support ascertaining patients’ preferences in medical decision-making are often limited to supporting patients to express preferences about a fixed set of treatment options [18]. Rietjens et al. [18] argue that what is needed is a radical new type of conversation tool, one that invites clinicians, patients, and their wider support system to engage in meaningful conversations about the ‘lived experience’ of illness while appreciating the different ways in which patients experience and navigate their illness. Such tools would also support more informed consent conversations.
This study has led to the development of recommendations for improvement in the hospital. One key area for improvement arising from this study is in relation to supporting consent conversations through providing patients as early as possible with PIMs about their treatment and the risks and benefits of that treatment. PIMs can provide a useful support tool for both patients and staff to facilitate consent conversations if they are tailored to the individual through discussions with their clinician, as the national consent policy notes ‘the risks that an individual person considers significant and relevant to their decision-making, can only be determined by discussion with them and by considering their will and preferences… Factors such as a persons’ occupation, lifestyle or culture may, for example, influence those risks that the person considers to be significant or particularly undesirable’ [1, p.22]. PIMs need to address the risks and benefits of all treatment options including none, and as found in this study and others, patients want information about the impact of the treatment options on their daily life in the short and long term [19]. It is also recommended that once patients have PIMs, they need ‘time out’ to review them and be able to come back to the conversation with their clinician with any questions relating to the information in the PIMs [19]. The hospital is currently exploring information and communication technology solutions that would support the tailoring of PIMs by clinicians for individual patients and their families and iterative interactive communication between clinicians and patients.
A second key area for improvement that the survey results have prompted is in relation to the tools used within the hospital to support the recording of consent conversations. The hospital has an electronic health record (EHR) and this may be used to support this process. In the first instance however, the paper-based form currently used to capture the consent conversation will be redesigned based on feedback from these surveys to better support a SDM process [17] in relation to the treatment. This form will then be embedded into the EHR system.
Other recommendations arising from the results of this study are to explore the perspectives of junior doctors (defined as those doctors who have graduated from medical school in the last year (interns) and two to 3 years (senior house officers (SHOs)) [20] and nursing staff in relation to their needs and experiences of consent practices. An information and awareness campaign for patients and their families about their role in consent conversations and SDM and the hospital being a teaching and research active hospital is also being undertaken. Empowering patients to engage in consent conversations and SDM is also essential to improving health literacy, which is a key objective of the World Health Organization [21]. Improving health literacy may also give public patients the skills to move beyond feeling the need to be a ‘model patient’ [7] and instead to be more actively engaged in understanding the risks and benefits of all their treatment options including none. When patients are more actively engaged in all aspects of their care, this can lead to greater improvements in quality and safety of care [22].
Strengths and limitations
Members of the public were recruited through our hospital’s social media accounts which may have introduced bias as people who follow the hospital on social media may have had themselves, or members of their family or friends, a predominately positive experience of their care in the hospital. Questions were phrased in such a manner however to elicit what was most important to them. Also, the free text comments reflected both positive and negative experiences. Future research should try to engage more diverse representation from both patient and public groups. Future research also needs to focus on consent in other aspects of health and social care, particularly those for which currently explicit consent is not always sought, e.g. taking bloods and moving and handling patients.
This study did not explore fully the issue of capacity where there was any question that the patient did not have the ability to make this particular decision in this moment. Capacity in this study was related to a patient being given enough information and in a way they could easily understand, which enabled them to make their own decision.





留言 (0)