
記住我

All 187 patients enrolled from Xiangya Hospital Central South University were followed up until February 2023, with a median follow-up duration of 26 months (IQR 17-45). The baseline clinicopathological characteristics and outcomes of the cohort at diagnosis are described in Tables 1, 2, and 3.
Table 1 Clinical characteristics at AAV diagnosis according to platelet countTable 2 Pathological presentation at AAV diagnosis according to platelet countTable 3 Main outcomes of AAV patients according to platelet countThe median age of the whole participants was 64 years old (IQR 56-71) and 96 (51.3%) patients were male. Among the cohort, 178 (95.2%) patients were positive for myeloperoxidase-ANCA and 8 (4.3%) patients were positive for proteinase 3-ANCA. The median BVAS was 18 (IQR 14-20) at diagnosis in AAV. Kidney was the most commonly affected organ followed by lung and systemic involvement [172 (92%) and 102 (54.5%), respectively]. At the baseline, the median serum creatinine and eGFR were 381 μmol/L (IQR 206.7-577) and 12.34 ml/min per 1.73 m2 (IQR 6.81-24.91), with a median proteinuria of 1.41 g/24 h (IQR 0.78-2.53). Kidney biopsies were performed in 74 (39.6%) patients. According to the Berden classification to evaluate the pathological lesions in biopsy specimens, Class I (focal), Class II (crescentic), Class III (mixed), and Class IV (sclerotic) were found in 15 (21%), 9 (12%), 41 (56%), and 8 (11%) patients, respectively [31]. During follow-up, 133 (71.1%) and 65 (34.8%) patients progressed to ESRD and death, respectively, defined as mentioned above.
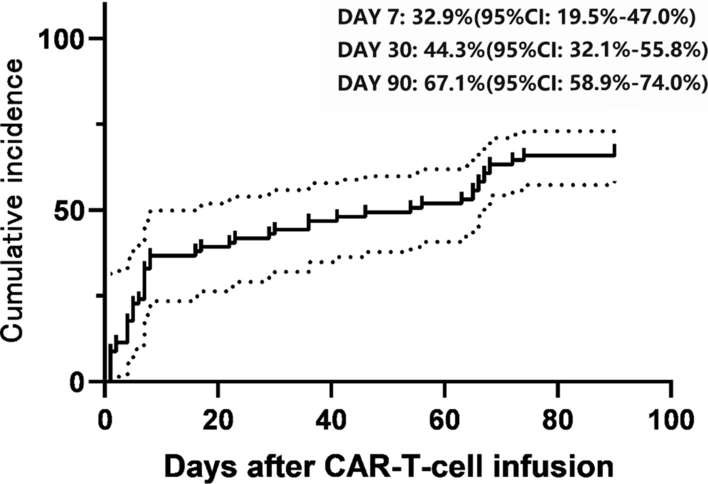
Comparison of variables between patients with low and high platelet countWe performed the ROC curve analysis with an area under the ROC curve (AUC) of 0.7338 and obtained the optimal platelet count cutoff of 264.5 × 109/L for predicting progression to ESRD (Fig. 1). Among the 187 AAV patients, 111 (59%) patients presented with a low platelet count, and 76 (41%) patients had a high platelet count, in which forty-nine patients had a platelet count above the upper limitation of normal range 300 × 109/L. Detailed contrast of characteristics between the two group of AAV patients at onset is shown in Tables 1, 2, and 3.
Fig. 1
Receiver operating characteristic curve showing the sensitivity and specificity of platelet count for predicting progression to ESRD of AAV patients
It was not statistically significant in demographic data with a median age of 63 years old (IQR 55-71) versus 65 years old (IQR 56-71) between patients with low and high platelet counts. Patients with low platelet count exhibited lower incidences of systemic (45% versus 68.4%; P = 0.002) and neurological (7.2% versus 17.1%; P = 0.035) manifestations while higher frequency of renal involvement (100% versus 94.7%; P = 0.026). Regarding laboratory results, AAV patients with lower platelet count presented with lower leukocytes [6.8 × 109/L (IQR 5.5–8.4) versus 9.9 × 109/L (IQR 8.05–12.83); P < 0.001], hemoglobin [79 g/L (IQR 67–88) versus 86.5 g/L (IQR 75–101); P = 0.003], serum complement levels [sC3 of 730 mg/L (IQR 619–827) versus 888.5 mg/L (IQR 719.5–1085); P < 0.001; sC4 of 228 mg/L (IQR 179–284) versus 267 mg/L (IQR 206.5–322.5); P = 0.015, respectively], ESR [59 mm/h (IQR 35–92) versus 104 mm/h (IQR 60.75–120); P < 0.001], CRP [13.1 mg/L (IQR 4.09–63.6) versus 38.6 mg/L (IQR 16.33–99.73); P < 0.001] as well as higher albumin [33.25 g/L (IQR 29.73–36.9) versus 30.75 g/L (IQR 27.28–34.53); P = 0.025]. In addition, compared to the cases with high platelet count, patients with low platelet count had lower eGFR [9.27 mL/min/1.73 m2 (IQR 5.9–15.98) versus 22.44 mL/min/1.73 m2 (IQR 10.67–42.84); P < 0.001] while more urine erythrocyte counts [164.5/μl (IQR 56–445.67) versus 51.5/μl (IQR 15–241.56); P = 0.001], proteinuria [1.62 g/24H (IQR 0.93–2.74) versus 1.08 g/24H (IQR 0.65–2.00); P = 0.015] and higher serum creatinine [489 μmol/L (IQR 305.1–627) versus 247 μmol/L (IQR 130.5–410); P < 0.001].
Regrettably, in terms of patients’ pathological findings, when examining the patients' pathological findings, no significant differences were identified in glomerular involvement, tubulointerstitial lesions, or the distribution of pathological classification between the patients with low and high platelet count—except for the interstitial inflammatory cell infiltration integral (P = 0.003). In regard to the Berden Classification, patients predominantly exhibited mixed ANCA-associated glomerulonephritis with a median platelet count of 252 × 109/L (IQR 203–313). Similarly, there was still no statistical significance about platelet count at diagnosis in the four distinct pathological forms of AAV patients according to Berden Classification (Supplementary data, Fig. 1).
Compared to those with high platelet count, patients with low platelet count were more prone to undergo kidney replacement therapy and had higher frequency of progression to ESRD (85.6% versus 50%; P < 0.001) accompanying with lower one-year and three-year overall survival rates (78.4% versus 92.1%; P = 0.012 and 63.1% versus 78.9%; P = 0.020, respectively). Consistently, patients with lower platelet counts exhibited comparatively higher percentage of death numbers than those with higher platelet counts (40.5% versus 26.3%; P = 0.045). In addition, we compared the circulating platelet counts at the onset in patients with varying disease activity levels and outcome statuses. Exactly, platelet levels were significantly lower in patients who needed KRT for more than 3 months and who progressed to ESRD as well as death (Fig. 2A, P < 0.0001; Fig. 2B, P < 0.0001; Fig. 2C, P = 0.0308; respectively). There was no significance of platelet counts in patients between BVAS ≤ 16 and BVAS > 16 (Fig. 2D, P > 0.9).
Fig. 2
Platelet count according to relevant outcomes A Need for KRT during follow-up B Renal survival (ESRD) C death. D BVAS
Correlations of platelet count with clinical characteristics in AAVWe analyzed correlations between the count of platelet and clinical features at diagnosis in AAV. Platelet level showed no relevance with baseline parameters including age and BVAS. Obviously, platelet count was positively associated with leukocytes, serum complement level, inflammatory indicators (ESR and CRP), and eGFR (r = 0.4665, P < 0.0001; r for sC3 = 0.4564, P < 0.0001; r for sC4 = 0.2147, P = 0.0047; r for ESR = 0.4122, P < 0.0001; r for CRP = 0.2715, P = 0.0002; r = 0.3807, P < 0.0001; respectively), while negatively correlated with albumin and renal involvement parameters such as urine erythrocyte counts, proteinuria, UACR, serum creatinine, blood urea nitrogen (r = − 0.1774, P = 0.0163; r = − 0.2547, P = 0.0009; r = − 0.2102, P = 0.0076; r = − 0.1866, P = 0.0251; r = − 0.3814, P < 0.0001; r = − 0.4012, P < 0.0001; respectively). Collectively, our data suggested that the lower platelet level of AAV patients may be closely related to severer renal damage and worse renal outcomes (Table 4).
Table 4 Correlations of platelet count with laboratory findings in AAV patientsAAV patients with low platelet count had poorer disease phenotypes and prognosisAiming to further verify the prognostic value of platelet count in patients with AAV, we next performed the Kaplan–Meier survival analysis. The results demonstrated that patients with low platelet counts had a worse overall survival rate and ESRD-free survival rate (Fig. 3A–B; P < 0.0001 and P = 0.0114, respectively).
Fig. 3
Kaplan–Meier curve for renal survival and all-cause mortality of AAV patients with low and high platelet count A renal survival and B overall survival according to platelet count. In red, patients with low platelet count (< 264.5 × 109/L); in blue, patients with high platelet count (> 264.5 × 10.9/L)
In the univariate Cox regression analysis of predictors for ESRD in AAV, age, BVAS, erythrocytes, hemoglobin, low platelet count, lymphocytes, serum C3, serum creatinine, eGFR, histopathological classification, percentage of crescentic glomeruli, moderate interstitial fibrosis integral and KRT condition were predictors of progression to ESRD (Supplementary data, Table 1). However, in the multivariate analysis, only low platelet count [HR 1.670 (95% CI 1.019–2.515), P = 0.014], serum creatinine [HR 1.002 (95% CI 1.001–1.002), P < 0.001] and age [HR 1.016 (95% CI 1.001–1.032), P = 0.038] remained as significant risk factors for ESRD occurrence (Fig. 4 and Supplementary data, Table 1). In other words, low platelet count was associated with a high risk of progressing to ESRD in AAV. Furthermore, although platelet status was a predictor for death in the univariate regression analysis, no correlation was found between platelet count and overall survival rate in the multivariate analysis (data not shown).
Fig. 4
Forest plot of multivariate Cox model for ESRD prediction
留言 (0)