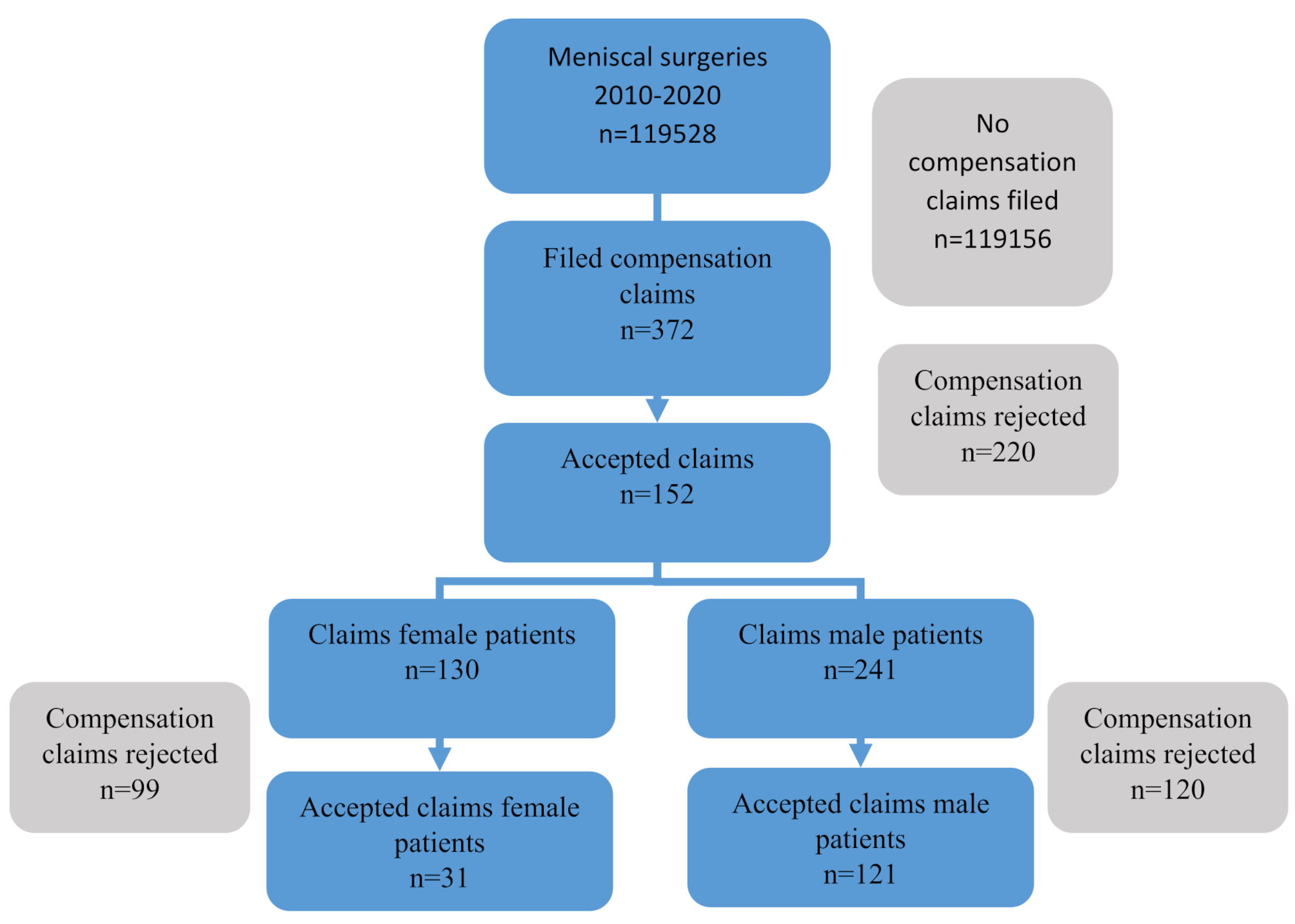
Our initial extract included 40,271 surgical cases from 2020 to 2021 (Fig. 1). Several exclusions were applied to the dataset, including endoscopy, obstetric, non-operating room, cardiac, and ophthalmology cases. After these exclusions, a total of 18,578 procedures remained for analysis. Further exclusions were made for cases with provider overlap, patients intubated on arrival or not extubated at the end of the procedure, cases with natural airways, cases with ambiguous start/stop times, and cases with documented equipment or post-anesthesia care unit (PACU) delays. The final dataset consisted of 15,084 surgical cases.
The breakdown of procedures by anesthesia provider group was as follows: 939 were performed by solo anesthesiologists, 2644 with attending/resident pairing, and 11,501 with attending/CRNA/CAA pairing. Residents were grouped as a single cohort as no significant differences were observed within the resident cohort based on clinical anesthesia year (CA 1–3) for anesthesia ready time, out-of-room time, total anesthesia-control time, and prolonged out-of-room times (Table 1).
Table 1 Induction, Extubation, and Anesthesia-Controlled times for Anesthesia ResidentsTable 2 presents patient demographics and associated comorbidities for the different anesthesia provider groups. While statistically significant, the clinical relevance of differences in age and BMI among the three groups is limited. There were significant differences in the racial distribution of patients, with a higher percentage of Black individuals in the resident cohort. This difference can be attributed to hospital location, with a higher percentage of Black patients at the Medical Center (37.9%) than the community hospital (29.2%). The resident and CRNA/CAA groups had a higher incidence of cardiovascular, pulmonary, vascular, and renal comorbidities than the anesthesiologist group. The ASA status was also higher for the resident and CRNA/CAA groups (3 [2 - 3]) compared to the anesthesiologist solo group (2 [2 - 3], p < 0.001), reflecting differences in comorbidities.
Table 2 Demographics and Co-Morbidities for anesthesia provider groupsTable 3 summarizes perioperative procedure characteristics, including surgical location, service category, and procedural times. The surgical locations are a community hospital practice, the medical center at UF Health-Jacksonville, and a free-standing ambulatory surgery center. Of the anesthesiologist-only cases, 93.5% were done at the community hospital, 5.4% at the medical center, and 1.2% at the ambulatory surgery center. In contrast, the care team procedures were done predominantly at the medical center for residents (93.3%) and CRNA/CAA (67.1%). The breakdown of surgical service categories shows that anesthesiologist-only care was more common in general/plastics and gynecology and less likely for head and neck, acute care surgery, thoracic, and vascular procedures. Residents were assigned significantly more thoracic, vascular, and acute care surgery cases than the CRNA/CAA or anesthesiologists-only groups. The remainder of the surgical services were comparable between the groups.
Table 3 Perioperative Characteristics– Location, Surgical Service, Induction, Extubation, and Anesthesia-Controlled Times for the Anesthesia Provider GroupsCompared to the anesthesiologist or CRNA/CAA groups, the resident group had longer anesthesia-ready times, 10.5 [8.5–13.4] vs. 9.5 [7.7–12.0] for the CRNA/CAA group and 8.7 [7.0-10.7] minutes for the anesthesiologist only group (Table 3, p < 0.001). Similar trends were seen in the surgery end-to-extubation and out-of-room times– resident, 14.9 [11.7–19.3], CRNA/CAA, 13.9 [10.8–18.0], and anesthesiologist solo,12.1 [9.5–15.1] minutes, respectively (p < 0.001). Overall, anesthesia-controlled times were significantly shorter in the anesthesiologist-only group at 21.0 [17.9–25.4] compared to 23.9 [19.7–29.5] for the CRNA/CAA group and 26.1 [21.7–32.0] minutes in the resident group (p < 0.001). Procedural times, including anesthesia ready-to-procedure start, procedure time, and total time in the operating room, were significantly shorter in the anesthesiologist-only practice than in the care team model, reflecting the community hospital practice.(Table 3) However, analysis of the total anesthesia-controlled time by general linear regression analysis adjusted for covariates (age, BMI, ASA classification, comorbidities, arterial line insertion, surgical service, and surgical location) did not show a statistically significant difference between the provider groups for estimated marginal mean for the anesthesia-controlled times. (Supplemental Tables 1 A-D) Prolonged extubation times (>15 min) were significantly less common in the anesthesiologist-only group compared to the care team groups (p < 0.001). This difference was still present after binary logistic regression for the resident group compared to the anesthesiologist solo group.(Supplemental Table 1E).
Table 4 presents the clinical outcomes based on the anesthesia provider group. The occurrence and duration of decline in mean arterial pressure (MAP) below 55 or 65 mmHg were similar for all groups.
A binary logistic regression analysis was performed to determine the effects of the significant univariate factors on the likelihood of a MAP < than 55 mmHg (> 1 min or > 10 min) or < 65 mmHg (>15 min). The Anesthesiologist group had slightly increased odds for low mean arterial pressures (1.2–1.7). The surgical location (medical center), surgical services, anesthesia duration, and various comorbidities (cardiac arrhythmia, pulmonary disease, complicated diabetes, and peripheral vascular disease) were associated with increased odds of low mean arterial pressure.(Supplemental Tables 2 A-C) The odds ratio effect sizes in the final models were generally small (OR < 1.86) [23, 24].
The univariate incidence of cardiac complications, pulmonary complications, and AKI were similar in all groups, as well as the 30-day mortality.(Table 4) Within the Multicenter Perioperative Outcomes Group dataset, a pulmonary complication comprises over 50 ICD 10 codes documented from the day of surgery through 90 days after surgery. These complications can be grouped into three general categories - respiratory failure, pneumonia, and pulmonary embolism. The univariate incidence of pulmonary complications was similar in the resident, CRNA/CAA, and anesthesiologist-only group. After logistic regression, the provider group and location had no significant impact on the pulmonary complications. (Supplemental Table 3)
Similarly, after binary logistic regression, the provider groups and locations had no increased odds of cardiac complications, myocardial infarction, or mortality, while age, anesthesia duration, and various comorbidities significantly impacted those outcomes. (Supplemental Tables 4–6)
After binary logistic regression, the odds ratio for AKI grade 1–3 remained similar for the provider groups with decreased odds of procedures performed at the ambulatory center. (Supplemental Table 7) Finally, the length of stay differences between provider groups was insignificant after adjusting for significant covariates and location. (Supplemental Tables 8 A-C)







留言 (0)