
記住我

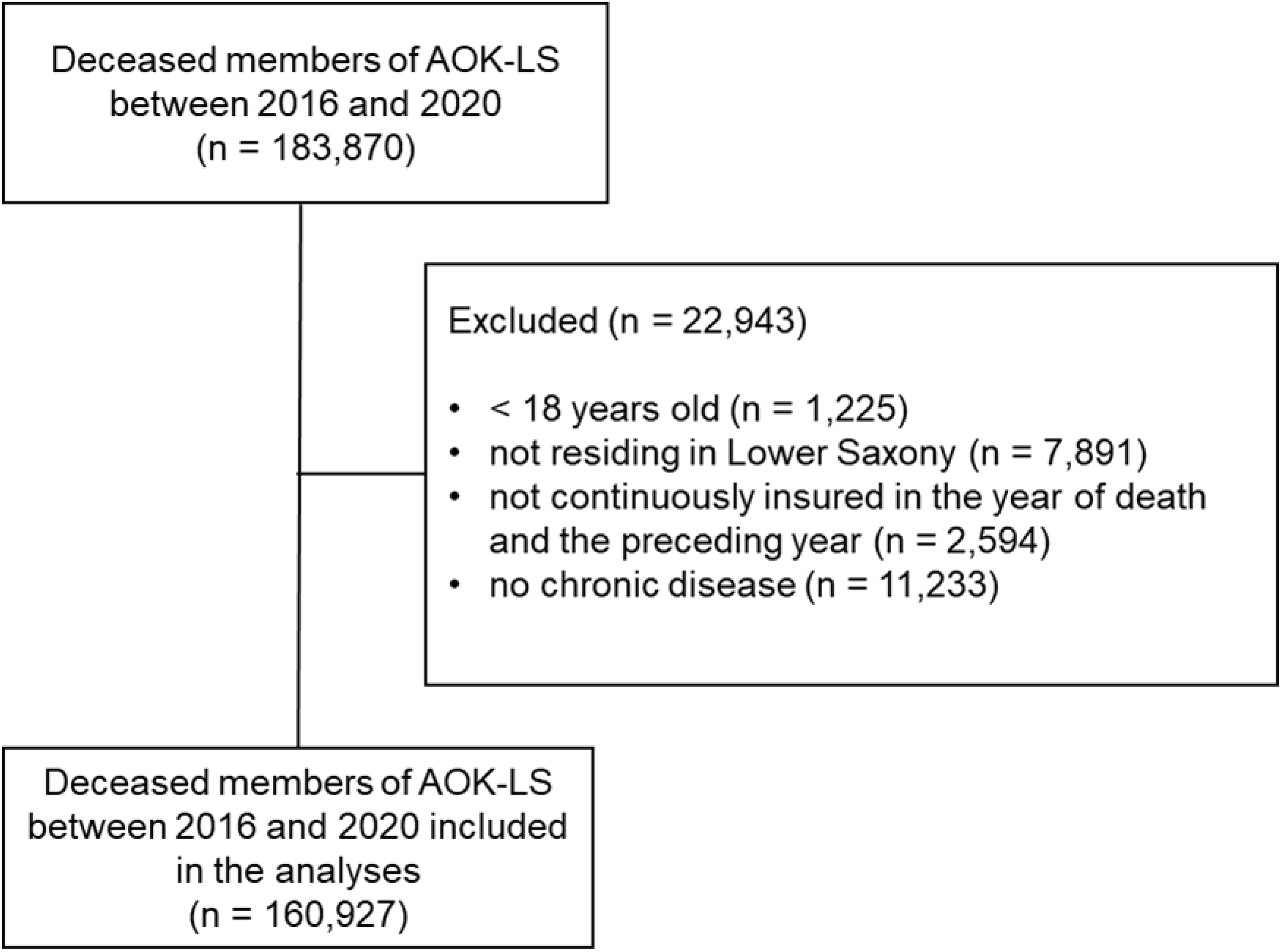








The initial search of databases produced 3,396 documents (Fig. 1). After removing duplicated studies, we screened 1,798 titles for eligibility from all databases. After initial screening of titles, we screened 76, and excluded 58 studies. Researchers read the remaining 18 full text studies and excluded 10 studies as they did not meet the eligibility criteria: one study was a case study, two studies were not conducted in a Middle Eastern country, and seven studies were assessed not to have relevant outcomes. We added one additional study, which had been identified from screening relevant review and reference lists of included studies. Therefore, nine studies are included in this review (Fig. 1). We had planned to exclude papers not written in English but in fact all papers identified through our search were written in English.
Fig. 1 Study characteristicsStudy designs
Study characteristicsStudy designsOf the nine included studies, three were quantitative, cross-sectional studies (Table 2), and six were qualitative studies (Table 3).
Methodological qualityThe six qualitative studies were classified as measured five and above out of eight [40,41,42,43,44,45]; and the three quantitative cross-sectional studies measured eight and above out of 10 [46,47,48]. using the JBI) critical appraisal tools (Table 4) (Table 5).
Table 4 JBI assessment for Quantitative studiesTable 5 JBI assessment for Qualitative studiesMain objectives of the studiesCross-sectional studies sought to measure ICU staff perceptions of barriers and supportive behaviors to the provision of end-of-life care in the intensive care unit [46,47,48]. The qualitative studies focus on exploring critical care nurses’ experiences and perceptions of providing end-of-life care for critically ill patients in an intensive care unit [43, 45]; evaluating nurses’ care practices at the end of life and their understanding of the provision of spiritual care at the end of life [41, 42]; identifying the needs, beliefs, and practices of Muslim family members during end-of-life care for a family member in the intensive care unit [40]; and the impact of organisational structures when integrating palliative care in intensive care units [44].
Study populationsWith the exception of one study that focused on family members [40], all the studies were of healthcare professionals. Participants in six studies of the studies were ICU nurses [41,42,43, 45, 46, 48]; one study involved ICU managers alongside health professionals [44] and another study involved ICU physicians and nurses [47].
Cultural contextThe findings of this review can only be fully understood in the light of the cultural and religious context of MENA countries, and the related professional cultures in healthcare. Both Arab and Muslim culture make professionals reluctant to withhold any intervention or medication for any patient in the ICU, and Muslim culture and practices (such as reading the Qur’an to the patient, performing prayer, placing the dying patient to face toward Mecca and saying the Shahadatain or testimony of faith) are often important to families. God is seen as the ultimate healer, who is able to heal the sick person at any stage, which feeds into a desire to keep the patient alive at all costs. Consequently, while some families are open about their loved one’s likely prognosis, discussion of death and dying is often avoided by both families and health care professionals [40], and withdrawing non-effective treatment may be seen as complicity in causing the patient’s death [44]. The patient’s death may not be faced until medical staff make a DNR decision and even this is sometimes opposed by families, which further limits discussion of EOL, and so curtails the EOL care offered to both patient and family.
Communication with the family and their involvement in decisions about the patient can vary greatly between ICUs in different regions [41, 44]. However, the professional culture in ICUs is often described as hierarchical, with medical staff reserving the right to speak with families about EOL care and yet often showing reluctance to make a DNR decision or to withdraw ineffective treatments. Nurses do not consider themselves professionally autonomous in these situations, and so are reluctant to speak openly with families without medical approval, resorting to hints and veiled references [41]. These difficulties in communicating with families are compounded by language barriers, in that many health care staff are from overseas [45]. Frequently, they do not share patients’ culture and beliefs, and usually speak English rather than Arabic, whilst Arabic is the first language for most families [41, 45, 46].
End-of-life care challenges and supportive behavioursWithin the overall cultural context described above, five main themes were identified as EOL care challenges and/or facilitators: organisational structure and management, (mis)understanding of end-of life care, spirituality and religious practices for the dying, communication about EOL care, and the impact of the ICU environment.
Organisational structure and managementMany ICUs lack policy and guideline documents in relation to palliative care. This leaves health care professionals without clear guidance and support in relation to DNR decisions and other clinical and ethical dilemmas. This means health care professionals are thrown back on their personal beliefs and cultural assumptions, as described above. This may create barriers for the integration of palliative care in ICU [44]. As noted above organisationally, ICUs may be hierarchical, with nurses deferring to doctors in end-of-life discussions with families, and a lack of professional autonomy and involvement in decision making. Yet medical staff were reluctant to speak plainly about death with families. Consequently, communication was unclear, treatments prolonged, and death sometimes unexpected by families. In addition, nurses identified a need for specialist education and training but reported none had received training in ethics or palliative care [41].
(Mis)understanding of end-of life careThe most reported challenge across the studies was related to different understandings of EOL care between healthcare team and family members [46,47,48]. Families may believe that introducing EOL care means actively ending the patient’s life, rather than providing the best supportive care and comfort measures when death has become inevitable. On the other hand, medical staff may avoid discussion with families about the patient’s prognosis and related EOL care, which contributes to the confusion for families and may lead to them not accepting the patient’s poor prognosis and misunderstanding what life-saving measures really mean. Some relatives may think that EOL care means abandoning the patient and neglecting ordinary care and treatment; or not appreciating how traumatic interventions such as CPR may be for the patient [46,47,48].
On the other hand, EOL care is facilitated when ICU staff take active steps towards patient and family-centred care. Family members can be taught how to approach caring for their dying relative. Agreeing a specific family member as the main communication link with the family enabled better communication of goals of care for the dying patient and avoided misunderstanding [48].
If family members are helped to accept that the patient is dying, this allows ICU staff to discuss EOL care and also provide appropriate support for the family, for example by providing a peaceful, dignified bedside scene for family members as their loved one approaches death, and by having the physician meet in person with the family after the patient’s death to offer support and reassure them that all possible care was given [47].
Spirituality and religious practices for the dyingFamily members of critically ill patients place a high value on the spirituality of death, and religious practices such as prayer, and appreciate it when these practices can be accommodated in the ICU. However, family members may believe that God is the ultimate healer, and so hold on to hope of recovery in the face of a poor prognosis, or even deny the possibility of death [40]. This presents a challenge to physicians who may wish to discuss EOL care and DNR decisions with family members [47]. On the other hand, nurses are capable of delivering end-of-life care in a culturally sensitive manner and aligned to Islamic values [41]. Engagement with family members (and sometimes patients) about spiritual needs when facing EOL allowed nurses to facilitate spiritual care, usually based on religious beliefs and practices [42]. Spiritual and physical care may overlap, as keeping the patient clean, having someone recite the Holy Qur’an to the patient, closing the person’s eyes as they die, and after death aligning the body towards Mecca, are all part of asking God to comfort, forgive, or heal the individual. Carrying out these practices may provide spiritual comfort to both families and nurses [43]. However the spiritual care appears insufficient in some ICUs due to diversity of beliefs among nurses [45].
Communication about EOL careFamily members of ICU patients suggested that the need for frequent updates about the health status and prognosis of their loved one was an important part of end-of-life care [40]. However, the majority of ICU nurses are non-Arabic speakers as a result they found it difficult to communicate with patients and their families about EOL care [45].
Family members of ICU patients suggested that nominating a particular member of the medical member to provide information during visiting hours aided communication, as did the presence of social worker. The input of a social worker is important when communicating bad news and clarifying complex issues around EOL care. In addition, Attia [48] found that 94.3% of critical care nurses report effective communication between physicians and nurses caring for the dying patient as facilitator. This can ensure the staff are updated about that all possible care was provided and that family support was given by a multi-professional team.
Impact of the ICU environmentOther frequently identified obstacles to EOL care, related to the ICU environment reported by health professionals include poor design of critical care units, restricted visiting hours, and nurses’ heavy workload [48]. It was noted that the ICU bedside of patient does not allow for privacy of dying patients or grieving of family members. Therefore, it was difficult for family members to stay as much as they wish close to the dying patient. Likewise, critical care nurses report that providing a peaceful, dignified bedside scene for family members to grieve in private helped facilitate EOL care for the family [47, 48]. It is also the case that nursing workload limits the time to provide the family with needed emotional support, which was reported as a further burden on nurses [40, 47].
留言 (0)