
記住我

OFD has a relatively low incidence, accounting for approximately 0.2% of all primary bone tumors [22]. Most authors reported that males have slightly higher OFD incidence than females [23]. However, Park et al. provided a female predilection in their study [4]. OFD is commonly found in infancy and childhood [11, 24, 25], whose ages are often lower than 20 years [4, 6, 22]. Gleason et al. reviewed 16 OFD patients and found that the median age of patients was 9.5 years, and 43.8% of the reviewed cases were younger than six years [23]. OFD frequently occurs in the intra-cortical of the tibia mid diaphysis but uncommonly involves the ipsilateral fibula [3, 7, 11]. The incidence of simultaneous invasion of both tibia and fibula was less than 12% [4, 6, 26], and isolated involvement of the fibula is only 3.8% [4]. In addition, bilateral tibia OFD has only been reported in 2 publications [8, 27].
Many authors believe that the disorder’s progression stops with the reaching of skeletal maturity [11, 12, 24, 26, 28,29,30]. Furthermore, Campanacci et al. [7] and Nagano et al. [4] propose OFD could regress spontaneously at puberty. Local curettage and excision have 25% recurrence postoperatively [31]. Surgical intervention is an alternative for children with pathological fractures, deforming, and extensive lesions before puberty [23, 26]. In addition, extra-periosteal “shark-bite” resection is the most widely used surgical strategy for a patient with OFD [3, 16]. We summarized the data on the epidemiology, clinical symptoms, treatment, and prognosis of OFD (Table 1).
Table 1 Clinical data of the study patientsClinical manifestationOFD can present with asymptomatic, mass, pain, swelling, deformity (anterior bowing of the tibia), and even pathological fracture [11, 24, 37]. Moreover, Gleason et al. [23] found that patients with OFD about 31% had pain, 13% experienced tibial bowing, 19% suffered pathologic fracture, the other 37% were found inadvertently on Imaging that was taken for other reasons, mostly after trauma [26]. Park et al. [4] reported a review of 80 OFD patients and had a similar incidence of each clinical sign compared to Gleason et al. [23]. The physical examination can reveal local tenderness over the tibia.
StagingOFD, differentiated adamantinoma (AD), and AD are three subtypes origin from the same family of bone tumors. OFD locates at the benign end of the spectrum, following differentiated AD lies mid-spectrum and AD at the malignant end [31]. Differentiated AD has extremely similar radiological features to OFD, and these neoplasm sub-types cannot be differentiated utilizing x-rays alone. Besides, AD might have more aggressive characteristics.
The total medullary cavity involvement is less frequently found in OFD and differentiated AD [31, 41, 42]. However, the complete involvement of the medullary cavity and cortex could be detected in most AD patients [31, 41, 42]. Besides, soft-tissue involvement and moth-eaten margins have also been described in AD patients [31]. Bethapudi et al. [31] reported that even though small lesions tend to support the diagnosis of OFD and differentiated AD more than AD, the size of lesions is less crucial in differentiating larger lesions [31]. To date, no distinguishing imaging characteristics to differentiate OFD from differentiated AD or AD have been established.
Radiological characteristicsRegarding radiography features of OFD, it can be divided into the following five subtypes based on radiological characteristics: ground glass type, cystic type, insect phagocytic type, towel gourd ladle type, sclerotic type (Fig. 1A-E). The x-rays in anteroposterior and lateral views are recommended for the affected area. Anterior eccentric lytic, cortical expansion, and intramedullary extension in the tibial were often found (Fig. 2). The tibia’s anterior bowing deformity, even pathological fracture, could also be detected on the tibial x-rays in patients with OFD. Besides, the lytic of OFD predominantly manifests as an intra-cortical lesion with well-circumscribed edges [43] and is sometimes encircled by a zone of sclerosis [4, 6, 11, 44]. Most, M.J et al. [26] indicated that multiple lucencies might be detected between the sclerotic areas and within the cortical bone, and the affected cortex of the tibia might be thickened or expanded, but the periosteal reaction in OFD patients is uncommon. In addition, as the disorder progresses, the lesion might affect the metaphysic and could show a longitudinal spread.
Fig. 1
The five subtypes of OFD on radiological. (A): ground glass type; (B): cystic type; (C): insect phagocytic type; (D): towel gourd ladle type; (E): sclerotic type
Fig. 2
Radiography features of OFD, differentiated AD and AD. (A, B): A newborn without birth complication and diagnosed with OFD. The left tibia’s frontal and lateral views explain the cortical disruption and oval lucency with cortical thinning. Citation: Jobke B, Bohndorf K, Vieth V, Werner M. Congenital osteofibrous dysplasia Campanacci: spontaneous postbioptic regression. J Pediatr Hematol Oncol 2014, 36(3):249–252. Copyright ©The Author(s) 2022. Published by Baishideng Publishing Group Inc [33]. (C, D): A 10-year-old girl presented with a 3-month history of pain in her left lower leg after bruising and was diagnosed with differentiated AD. X-rays revealed a 6-cm mass with multiple osteolytic and sclerotic lesions in the thickened anterior diaphysis of the left tibia. Citation: Yamamura Y, Emori M, Takahashi N, Chiba M, Shimizu J, Murahashi Y, Sugita S, Iba K, Hasegawa T, Yamashita T. Osteofibrous dysplasia-like adamantinoma treated via intercalary segmental resection with partial cortex preservation using pedicled vascularized fibula graft: a case report. World J Surg Oncol 2020, 18(1):203. Copyright ©The Author(s) 2022. Published by Baishideng Publishing Group Inc [12]. E-F: a 79-year-old man diagnosed as AD with lower leg pain and an enlarging tibial mass. Multifocal eccentric, expansile lytic lesions are evident, with intervening sclerosis, demonstrating the so-called soap bubble appearance. Citation: Most MJ, Sim FH, Inwards CY. Osteofibrous dysplasia and adamantinoma. J Am Acad Orthop Surg 2010, 18(6):358–366. Copyright ©The Author(s) 2022. Published by Baishideng Publishing Group Inc [26]
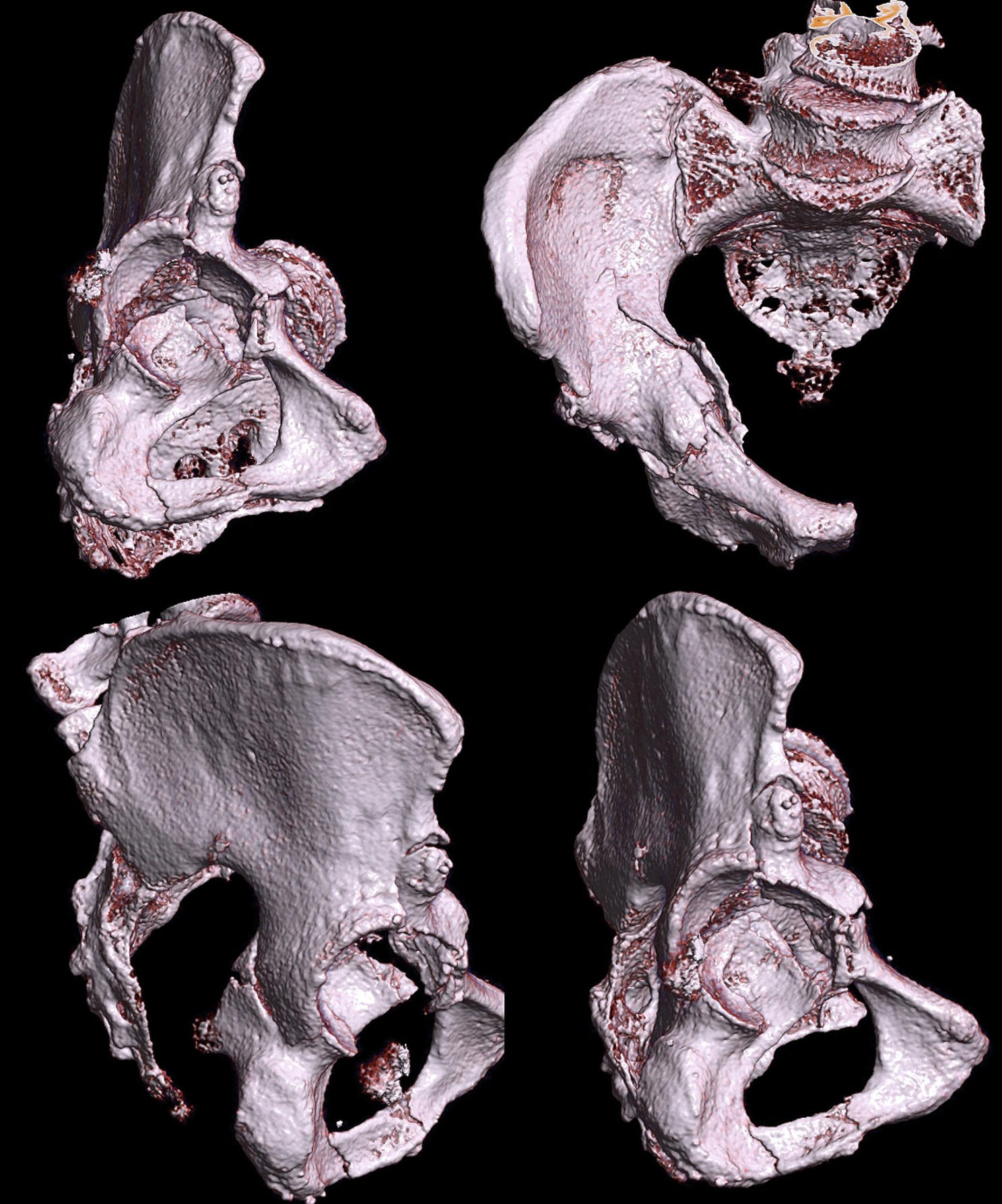
Computed tomography (CT) is better than MRI in evaluating cortical involvement, periosteal reaction, matrix mineralization, as well as pathological fractures (Fig. 3). Nevertheless, CT is only a complement to MRI in the comprehensive evaluation of the lesion but is not a substitute [31].
Fig. 3
CT features of OFD, differentiated AD and AD. (A): CT images of a 14-year-old white female with OFD showed an intracortical expanding lucent lesion with sclerosis of the inner margin. Besides, no intraosseous calcification or soft tissue mass was found. Citation: Ibrahim Fikry Abdelwahab, George Hermann, Joan Zawin, Michael M. Lewis, Klein MJ. Case report 543. Osteofibrous dysplasia of tibia. Skeletal Radiol 1989, 18: 249–251. Copyright ©The Author(s) 2022. Published by Baishideng Publishing Group Inc [75]. (B): The CT scans of a 10-year-old girl with differentiated AD revealed that a 6-cm mass was confined to the cortex of the tibia. Citation: Yamamura Y, Emori M, Takahashi N, Chiba M, Shimizu J, Murahashi Y, Sugita S, Iba K, Hasegawa T, Yamashita T. Osteofibrous dysplasia-like adamantinoma treated via intercalary segmental resection with partial cortex preservation using pedicled vascularized fibula graft: a case report. World J Surg Oncol 2020, 18(1):203. Copyright ©The Author(s) 2022. Published by Baishideng Publishing Group Inc [12]. (C): The CT images of a 38-year-old man with a classical AD showed obvious destruction of the tibial cortex. Citation: Bethapudi S, Ritchie DA, Macduff E, Straiton J. Imaging in osteofibrous dysplasia, osteofibrous dysplasia-like adamantinoma, and classic adamantinoma. Clin Radiol 2014, 69(2):200–208. Copyright ©The Author(s) 2022. Published by Baishideng Publishing Group Inc [31]
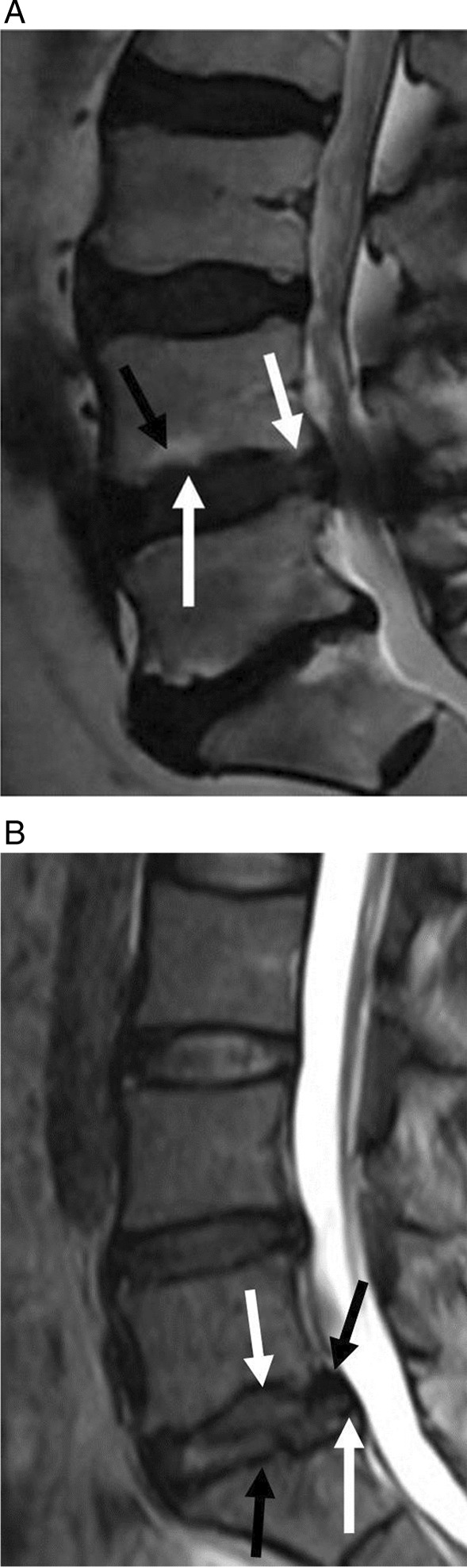
Concerning magnetic resonance imaging (MRI) findings of OFD, numerous authors have reported the MRI appearance of OFD, and they found that the OFD has the characteristic of an osteolytic lesion with a bubbly appearance and lobular loculations with well-circumscribed sclerotic edges [23, 31, 41, 45]. On MRI, Bethapudi et al. [31], Tehranzadeh et al. [41], and Utz et al. [45] found that OFD frequently involves the anterior diaphyseal cortex of the tibia or fibula with adjacent cortical expansion (Fig. 4A-E). Besides, anterior bowing deformity of the tibial diaphysis and intramedullary involvement are frequent complications as the disorder progresses [10, 16]. On MRI, the signal intensity of OFD shows intermediate to high on T2WI and intermediate on T1WI. Multiple factors can affect the signal intensity of OFD in MRI. Firstly, cystic, hemorrhagic, and even cartilaginous differentiation might influence the signal intensity and lead to heterogeneous signal intensity. Secondly, collagen density, the cells, and the degree of mineralization in the osteoid matrix could also affect the signal intensity. Moreover, the imaging features of OFD are similar to other fibroblastic stromal tumors that do not always show such different signal intensity patterns and can present a comparatively well-enhanced pattern that is likely to reflect rich fibrovascular stroma [45]. Thus, MRI can provide some evidence, but it is not the gold standard for diagnosing OFD. Accurate diagnosis directly affects treatment decision-making and prognosis in patients with OFD. Unilocular OFD in images needs to be differentiated with osteoid osteoma, intra-cortical abscess, and intra-cortical hemangioma. Meanwhile, multilocular OFD in images must be differentiated with AD, an aneurysmal bone cyst, osteoblastoma intra-cortical, and fibrous dysplasia.
Fig. 4
MRI of OFD, differentiated AD and AD. (A, B): Sagittal and axial T2-weighted fat-suppressed MRI images of a 15-year-old female patient with typical OFD showed that the sclerotic rim has an internal septa (white arrow), and the lesion involves the cortical (triangles) only and not the medullary [31]. The MRI of a 10-year-old girl with differentiated AD illustrated heterogeneously hypointense and isointense on a (C) T1WI and heterogeneously hyperintense on a (D) T2WI; Importantly, there is an incomplete involvement of the medullary cavity. Citation: Yamamura Y, Emori M, Takahashi N, Chiba M, Shimizu J, Murahashi Y, Sugita S, Iba K, Hasegawa T, Yamashita T. Osteofibrous dysplasia-like adamantinoma treated via intercalary segmental resection with partial cortex preservation using pedicled vascularized fibula graft: a case report. World J Surg Oncol 2020, 18(1):203. Copyright ©The Author(s) 2022. Published by Baishideng Publishing Group Inc [12]. E: Sagittal T1-weighted postcontrast MRI of a 10-year-old male child with a classic AD demonstrated an expansile lesion in the mid-tibial diaphysis and a thinning of the cortex (black arrow); Moreover, it explained complete medullary infiltration (white arrow). Citation: Bethapudi S, Ritchie DA, Macduff E, Straiton J. Imaging in osteofibrous dysplasia, osteofibrous dysplasia-like adamantinoma, and classic adamantinoma. Clin Radiol 2014, 69(2):200–208. Copyright ©The Author(s) 2022. Published by Baishideng Publishing Group Inc [31]
PathogenesisAs for cytogenetic of OFD, the authors analyzed the specimens of patients with OFD and found trisomy abnormalities on chromosomes 7, 8, 12, 21, or/and 22 [46]. Kanamori et al. [47] and his colleagues described the extra copies abnormalities on chromosomes 7, 8, 12, 19, or/and 21 in 2 of 3 patients with differentiated AD and 7 of 8 patients with classic AD. These cytogenetic studies show that OFD might be a clonal tumor lesion rather than a developmental dysplasia [46, 47]. The occurrence of AD may require several steps, including clonal chromosome anomalies, growth factors, and receptors, while OFD and differentiated AD have only undergone partly of them [23]. These three disorders are linked and consistent. However, whether one lesion develops or degenerates into another is still controversial.
Concerning the proteomics of OFD, Maki, and Athanasou [48] revealed a frequent expression of numerous proto-oncogenes, including c-jun and c-fos, and bone matrix proteins including collagen IV, laminin, and galectin 3 in both OFD and AD. Some of these proteins are associated with mesenchymal-to-epithelial differentiation, which provides evidence to interpret why the primary bone tumors contain epithelial components. Bovée et al. [49] researched the expression of growth factors in the epithelial and fibrous portions of AD; they concluded that both the epithelial and fibrous components express fibroblast growth factor receptor-1 and fibroblast growth factor-2, but only the epithelial tissue elements express high levels of epidermal growth factor receptor and epidermal growth factor [49]. Furthermore, AD has a higher epidermal growth factor receptor and epidermal growth factor in the epithelial cells than differentiated AD [49]. In addition, the previous studies found that a proliferation marker and the high levels of Ki-67 can be detected in the epithelial component only [26, 49], which indicating that the epithelial part may be related to malignant activity and tumor growth [26]. It also supports the precursor lesion theory because if the lesion develops from benign to malignant, epithelial cells can obtain a higher expression of fibroblast growth factor-2, epidermal growth factor receptor, epidermal growth factor, and a higher proliferative activity [26].
Concerning molecular analysis for OFD, somatic mutations of the guanine nucleotide-binding protein/a-subunit (GNAS) gene might lead to monostotic fibrous dysplasia, polyostotic fibrous dysplasia, McCune–Albright syndrome, and soft tissue myxoma coexisting with fibrous dysplasia [50]. GNAS gene has the function of encoding the a-subunit of the heterotrimeric G (Gsa) protein complex, and it is located on chromosome 20q13.3 [51]. Alman et al. [52] found two key mutations in exon 8 of the GNAS gene. These mutations are the substitutions of Codon 201, resulting in the substitution of arginine by cysteine (R201C) or histidine (R201H). In addition, there are also uncommon cases with replacement of glycine (R201G) [53], leucine (R201L) [54], and serine (R201H) [55]. Scholars have reported a rare case of fibrous dysplasia related to the mutation of exon 9, resulting in the substitution of glutamine at position 227 by arginine, leucine, histidine, or lysine [56]. In dysplastic cells, all mutations cause an increase in Gsa adenylate cyclase activity and lead to excessive cyclic adenosine monophosphate formation [50]. The increase of intracellular cyclic adenosine monophosphate level might lead to the excessive formation of c-fos, resulting in the uncontrolled expression of osteopontin, ultimately leading to the inhibition of the osteoblasts maturation and increase their proliferation [
留言 (0)