
記住我




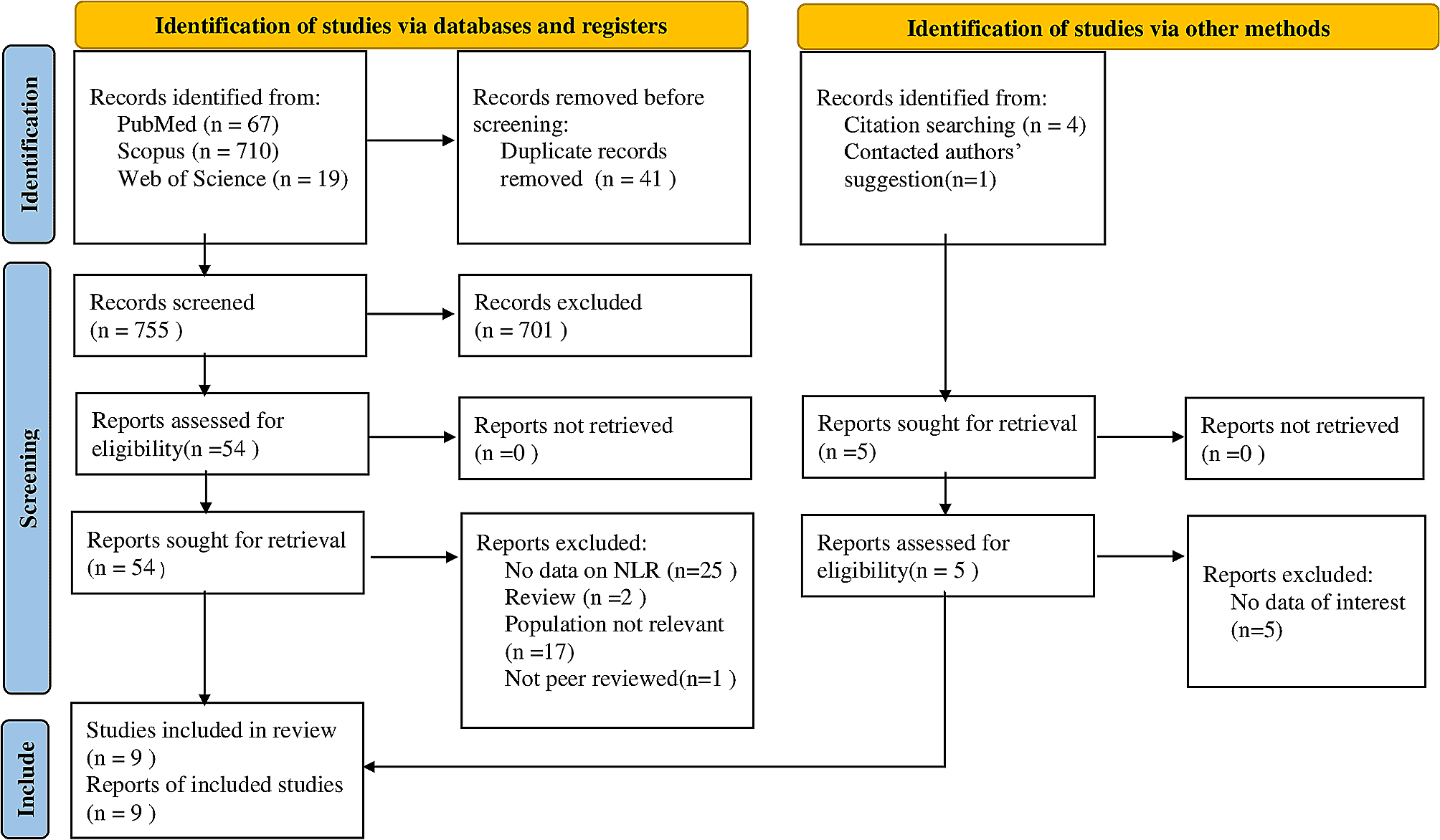

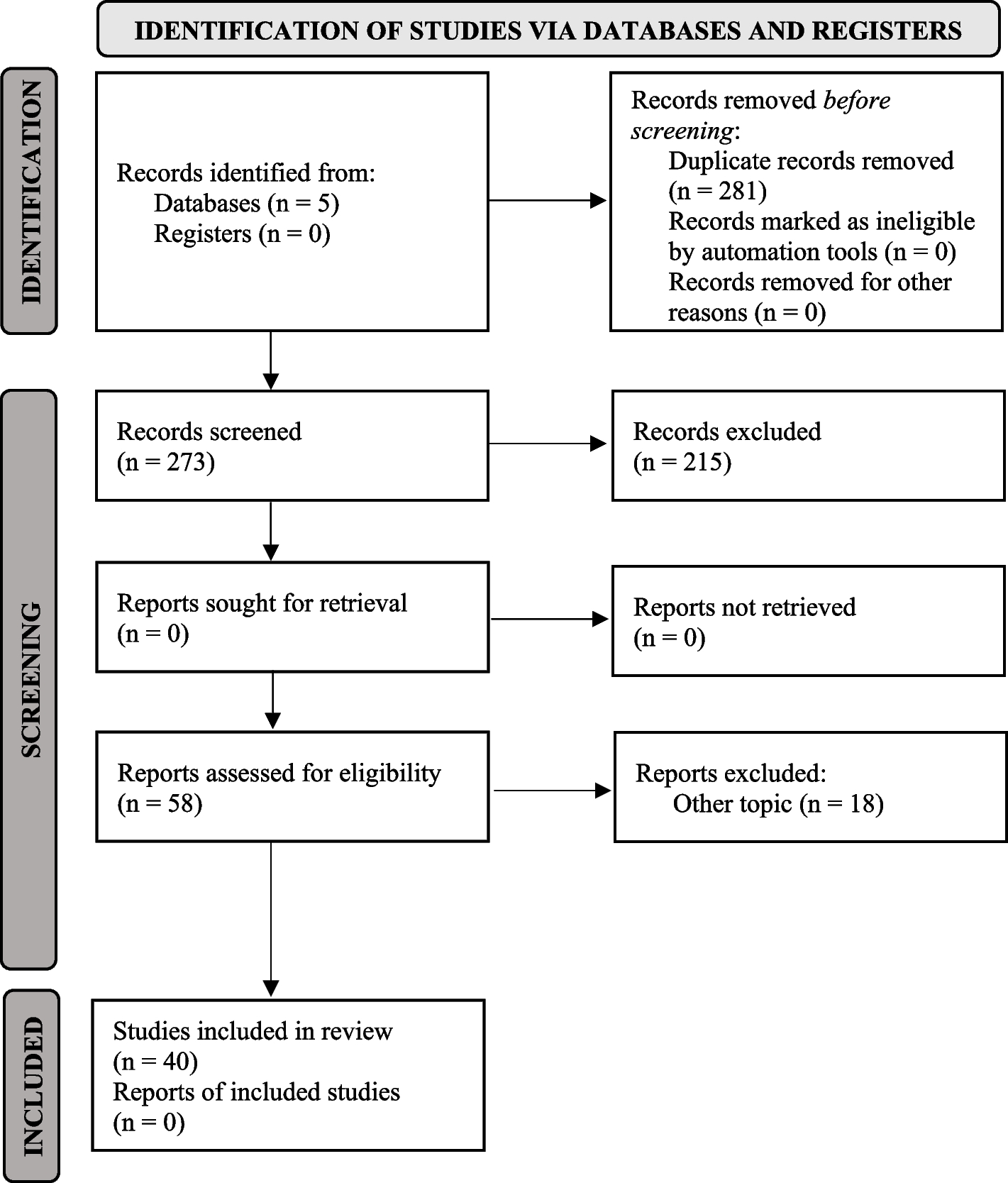
A total of 801 articles were identified through databases and manual searches. Finally, nine articles were included for this review. The article-chosen process is illustrated in Fig. 1. The selected articles comprised two prospective, six retrospective, and one cross-sectional study. The characteristics of the included studies and their risk of bias assessment are summarized in Table 1. One study had a NOS score of six, five had a NOS score of seven, and two had a NOS score of eight. All studies therefore met criteria for high quality.
Fig. 1
Flow diagram of includes searches
Table 1 General characteristic of included studiesIn a research published by Dogruel et al. [17], 100 patients with severe OI were retrospectively reviewed to assess the prognostic value of NLR and mean platelet volume (MPV). Based on the length of hospital stay, they divided patients into two groups: Group 1 with a hospital stay of one day or less and Group 2 with more than one day. No statistically significant difference was detected in age and gender (p = 0.925 for age and p = 0.823 for gender). Spearman’s correlation results indicated positive and statistically significant correlations of NLR with a prolonged hospital stay, postoperative antibiotics, and total antibiotic doses. In receiver operating characteristics (ROC) analysis, NLR’s optimum cut–off level was 5.19 (specificity: 81, sensitivity: 51). NLR of group 2 was detected to be 5.19 or higher. Patients were also divided according to the presence of fever, defined as a temperature of 38 °C or more pre- and post-operatively. As a result, NLR was correlated with preoperative fever (p = 0.001).
Pavan et al. [18] implemented a prospective research of 50 cases diagnosed with OI. They aimed to detect the value of vital sign changes and laboratory tests in determining the severity and length of stay (LOS). The authors categorized patients into group 1 and group 2, representing the hospital stays that lasted up to three days and more than three days, respectively. The distribution of cases regarding mean age and sex showed no statistical significance. The average LOS was 2.8 and 6.9 days for groups 1 and 2, respectively. Obtained mean values of all laboratory tests showed statistical significance between groups, apart from ESR (p-value of NLR = 0.044). Spearman’s correlation analysis revealed a positive correlation of LOS with NLR (r = + 0.291, p = 0.041), leukocytosis (r = + 0.284, p = 0.045), neutrophilia (r = + 0.302, p = 0.033), CRP levels (r = + 0.426, p = 0.003), and heart rate (r = + 0.311, p = 0.028). Moreover, the simple regression analysis of the numbers obtained in decreasing order demonstrated that 29.0% of the variation in hospital stay time was related to an increase in NLR.
Kusumoto et al. [19] retrospectively analyzed 271 patients with severe OI to evaluate the efficiency of routine blood tests as an early detective method. Patients were divided into four groups: cellulitis, cellulitis with superficial abscess formation, profound abscess formation, and necrotizing soft tissue infection (NSTI), representing groups I to IV, respectively. There was no significant difference concerning age and gender among these four groups (P = 0.087 for age and P = 0.561 for gender). There was an increasing pattern in all inflammatory and hematologic factors, including WBC, neutrophil, CRP, NLR, CRP + NLR, platelet-to-lymphocyte ratio (PLR), systemic immune-inflammation index (SII), and the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC). This was consistent for group I to group IV (P < 0.001), independent from hemoglobin and lymphocyte fraction that tends to decrease. NLR was utilized to calculate SII (platelet count × neutrophil count/lymphocyte count). Moreover, the necessity for contrast-enhanced CT (CECT) was decided based on comparing these parameters between groups I + II and III + IV. They performed a decision tree analysis considering higher amounts of inflammatory and hematologic parameters in groups III + IV than in groups I + II. Decision-making for CECT and differentiation of group III + IV can be determined by SII of ≥ 282 or < 282 but with a CRP + NLR of ≥ 25 because of this analysis.
Sakarozi et al. [20] conducted a retrospective cohort study of 96 patients with Ludwig’s Angina, a submandibular cavity infection with cellulitis that can quickly progress and become life-threatening. They aimed to determine the association between pre-therapy NLR and various prognostic factors in these patients. Regarding gender distribution, males were more likely to develop the condition. ROC analysis illustrated the optimal cut-off value of 16.86 for NLR. Forty-nine samples were with low NLR (< 16.86), and 47 were with high NLR values (≥ 16.86). NLR reached a significant relationship in predicting disease severity and LOS (p = 0.032 and p = 0.033, respectively). This study evaluated mortality status during hospitalization. The relationship between NLR and mortality was statistically significant (p = 0.026, specificity of 55.5%, and sensitivity of 70.8%). Considering Kaplan Meier’s analysis, the low-NLR group’s survival rate was significantly higher than that of the high-NLR group (p = 0.009).
A retrospective study by Xiaojie et al. [21], including 18 patients with severe and extremely severe oral and maxillofacial space infection (OMSI), was carried out to determine the predictive value of NLR and IL-6 in OMSI intensity. Of these 18 patients, 12 had severe OMSI, and 6 had extremely severe OMSI. Correlation analyses demonstrated a positive correlation between IL-6 and CRP with NLR (rs = 0.773, P = 0.005 and rs = 0.556, P = 0.020, respectively). This study also revealed that the number of involved organs correlated positively with NLR (rs = 0.511, P = 0.030). Furthermore, the number of complications positively correlated with NLR values (r = 0.576, P = 0.012). Consequently, a higher NLR was considered an essential predictor of organ involvement (P = 0.027) as well as the number of complications (P = 0.001).
In another retrospective study, Rosca et al. [22] evaluated 108 hospitalized patients with OI to determine whether NLR and CRP were the accurate prognostic tools for OI severity. Considering the severity of the infection, cases were divided into two equal groups: Group A with mild to moderate infections; Group B with moderate to severe infections. Regarding age and sex, no statistically significant differences were found among groups A and B (P = 0.150 and P = 0.236, respectively). In contrast, coming from rural regions (P = 0.019), being afflicted with diabetes mellitus (P < 0.001), and being a smoker (P = 0.028) were more frequent in group B compared to group A. Regarding the infection characteristics among patients, abscesses comprise 70.4% of infections in group A, while associations of abscesses and cellulitis were responsible for 55.6% of infections in group B (P < 0.001). Moreover, group B had more patients developing sepsis than group A (p-value = 0.030). Severity evaluations were calculated according to SII and the Symptom Severity score (SS). SII and SS scores were significantly higher in group B patients (P < 0.001). Likewise, tested biomarkers, including the CRP-NLR association, showed higher scores in patients of group B (median score of 341.4 vs. 79.0 in group A, P < 0.001). No statistical significance prior to logistic regression was seen for NLR between groups A and B (P = 0.019). However, in logistic regression analysis adjusted for age, gender, and comorbidities, NLR reached statistical significance with an odds ratio of 4.46 (95% CI = (3.53–5.40), P < 0.001), and the CRP-NLR association accounted for a 7.28 (95% CI = (4.83–10.16), P < 0.001) higher risk for severe OI.
In parallel, Gallagher et al. [23] retrospectively enrolled 161 patients with deep neck space infections of odontogenic origin and divided them based on the LOS: Group 1 consisted of 91 patients admitted for zero to two days, Group 2 with 70 patients admitted for three or more days. The male gender was statistically significant (p = 0.03). In contrast, no statistical significance was found between groups regarding age evaluation (p = 0.47). The mean days of LOS were 2.9 ± 3.2 (range: 0.5–35), and the mean values of admission NLR were 7.5 ± 7.7. According to Spearman’s correlation test, admission NLR showed a positive correlation with LOS (r = 0.30, p ≤ 0.01). In the ROC analysis, the best cut-off value of NLR to predict a LOS ≥ two days was 4.65 (test specificity = 61.5%, test sensitivity = 61.4%). In addition, a cut-off of 11.75 for NLR predicted admission in ICU with 82.6% specificity and 66.7% sensitivity.
Silva et al. [24] prospectively collected 66 hospitalized patients with OI, aiming to detect the possible correlations between computed tomographic findings of involved fascial spaces and laboratory markers, length of hospital stays, and Intensive Care Unit (ICU) admission. The mean LOS was 4.3 days. The involvement of 240 fascial spaces was observed in this study, with a mean of 3.63 spaces per patient. Submandibular 65 (27.1%), buccal 50 (20.8%), and sublingual 44 (18.3%) were the first three involved spaces. Higher levels of neutrophils (p = 0.001), NLR (p < 0.001), and CRP (p < 0.001) were associated with more significant numbers of involved spaces. The mean LOS progressively increased regarding the number of involved fascial spaces. Also, the need for ICU admission and the number of fascial spaces revealed a significant difference (p < 0.001).
An analytic observational study by Chamora et al. [25] was performed to identify NLR correlation with LOS among two groups of patients with and without diabetes mellitus (DM) afflicted with submandibular abscesses. Of 15 patients, six were in the DM group, and nine were in the non-DM group. The mean age of DM patients was higher than non-DM participants (50.33 ± 9.54 years and 33.56 ± 17.78 years, respectively). In addition, the male-to-female ratio of DM patients was 1:1, compared to 2:1 for patients without DM. For DM participants, the mean length of hospital stay was 7.83 + 1.47, and for non-DM participants, it was 8.22 + 2.86. Considering the therapeutic response, assessments were based on LOS, defining a good response as LOS ≤ 7 days. The mean NLR of the non-DM group was higher than for patients with DM (16.53 ± 11 and 7.65 ± 4.92, respectively). However, this lower value in the DM group did not lead to a better therapeutic response. In this study, contrary to previous studies, the comparison of NLR between DM and non-DM patients for therapeutic responses did not reach statistical significance (p = 0.88 for the DM group and p = 0.5 for, respectively).
留言 (0)