Osimertinib is widely used in the treatment of EGFR-mutated NSCLC. To the best of our knowledge, this is the first retrospective real-world data study evaluating the effect of dose reduction of osimertinib on efficacy in patients of all ages who were started on osimertinib as the first-line therapy for EGFR-mutated NSCLC.
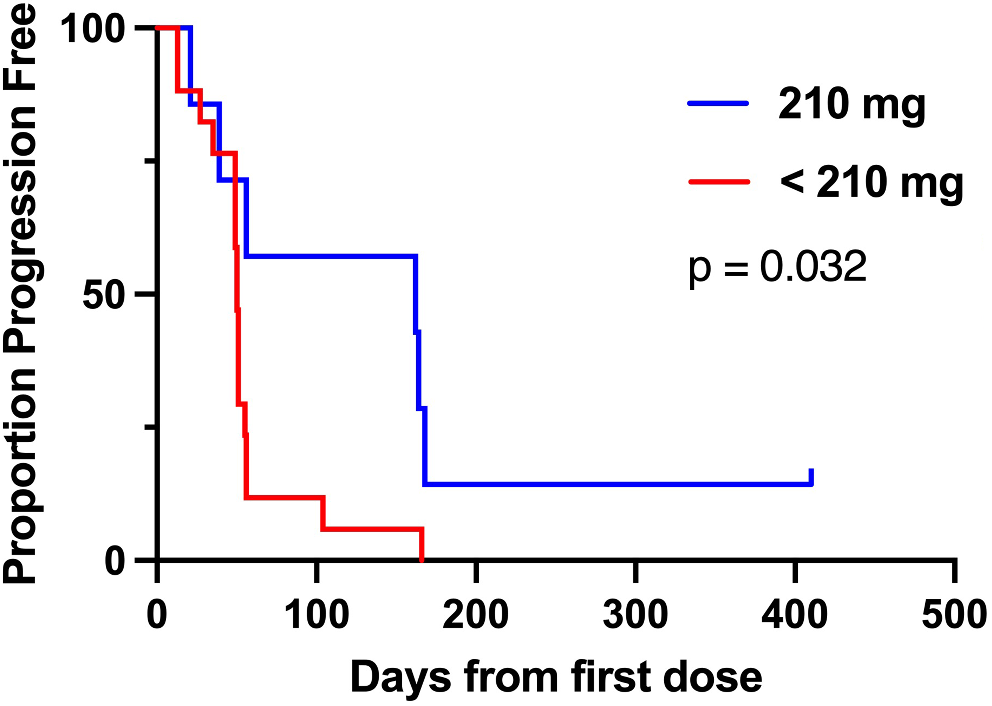
The median PFS was significantly prolonged in the dose reduction group compared with that in the standard dose group. This may be due to differences in osimertinib exposure and treatment discontinuation due to ILD between the two groups. A previous study reported that PFS was prolonged in patients with predicted osimertinib trough concentration (Cmin, pred) < 166 µg/L compared with those with Cmin, pred ≥ 166 µg/L [11]. Additionally, the AURA study that evaluated the safety and efficacy of osimertinib at doses of 20–240 mg once daily showed similar response rates at doses of 20, 40, and 80 mg/day [12]. Furthermore, an observational study of Japanese patients aged 75 years and older treated with osimertinib as the first-line therapy showed that PFS tended to be longer in patients with reduced osimertinib dose than in those with a standard dose (80 mg/day) [13]. These findings are consistent with those of our study. The relative increase in osimertinib exposure due to the administration of the standard dose compared with the reduced dose of osimertinib may contribute to the increased treatment discontinuation rate due to ILD. In this study, although no significant difference in the incidence rate of ILD was observed between the standard dose group and the dose reduction group (30.0% vs. 24.0%), the rate of treatment discontinuation due to ILD was higher in the standard dose group than in the dose reduction group (25.0% vs. 4.0%). Moreover, the patients who discontinued treatment due to ILD showed significantly shorter PFS than the other patients (Fig. 3). Among 16 patients who discontinued treatment due to ILD, 15 patients were in the standard dose group, which may have contributed to the poor PFS in the standard dose group. With first-generation TKI gefitinib, patients who developed ILD tended to show higher exposure to gefitinib than those without ILD [14]. Additionally, it has been reported that pneumonitis tends to increase with increased exposure to osimertinib [15], and increased osimertinib exposure in the standard dose group may have resulted in treatment discontinuation. Therefore, the dose reduction group tended to have a longer median TTF than the standard dose group. In this study, plasma concentrations of osimertinib were not measured, and the association between exposure to osimertinib and ILD onset remains unclear. Furthermore, no significant difference in OS was observed between the groups. Since OS is greatly affected by post-treatment after osimertinib therapy, osimertinib dose reduction in the first-line therapy may not affect OS.
The proportion of patients, who continued or resumed osimertinib treatment after the incidence of ILD because the image findings of pneumonia had resolved and there were no abnormalities in respiratory function, was higher in the dose reduction group (20.0%) than in the standard dose group (5.0%). Treatment discontinuation due to ILD was one patient among six patients with incidence of ILD in the dose reduction group, indicating that ILD observed in patients with dose reduction may not preclude continuation of treatment. On one hand, dose reduction within 6 months significantly prolonged PFS in the elderly patients, whereas it did not significantly contribute to PFS prolongation in the non-elderly patients (Supplemental Fig. 1). This may reflect that the treatment discontinuation rate due to ILD was higher in elderly patients compared to non-elderly patients in the standard dose group (34.5% vs. 16.1%). Since elderly patients have relatively low body surface area, the fixed dose of osimertinib might result in relatively higher blood concentrations in the standard dose group, causing increased severe ILDs and higher rates of osimertinib treatment discontinuation, while there was no relationship between dose reduction and PFS in non-elderly patients. These results suggest that dose reduction of osimertinib with a lower frequency of adverse events may be an option in a wide range of ages, especially in the elderly patients.
Generally, osimertinib can greatly penetrate the blood–brain barrier and has a reduced risk for central nervous system progression compared with first-generation EGFR-TKIs, such as gefitinib and erlotinib [16, 17]. However, dose reduction caused a lower osimertinib concentration in the cerebrospinal fluid, raising concerns about an increased risk of brain metastasis recurrence. In this study, metastasis recurrence was not significantly different between the dose reduction group (4.0%) and the standard dose group (5.0%). In this study, periodic imaging tests to confirm brain metastasis recurrence were not performed in some cases. Therefore, further investigations are needed to evaluate the effect of dose reduction on the exacerbation of brain metastasis.
In the dose reduction group, the severity of AE that triggered the initial dose reduction was grade 3 in more than half of the cases at the time of each AE onset. However, the severity grades of all AEs were reduced to grade 1 or less within 60 days after dose reduction (Supplemental Table 1). Therefore, almost all AEs were appropriately managed by dose reduction.
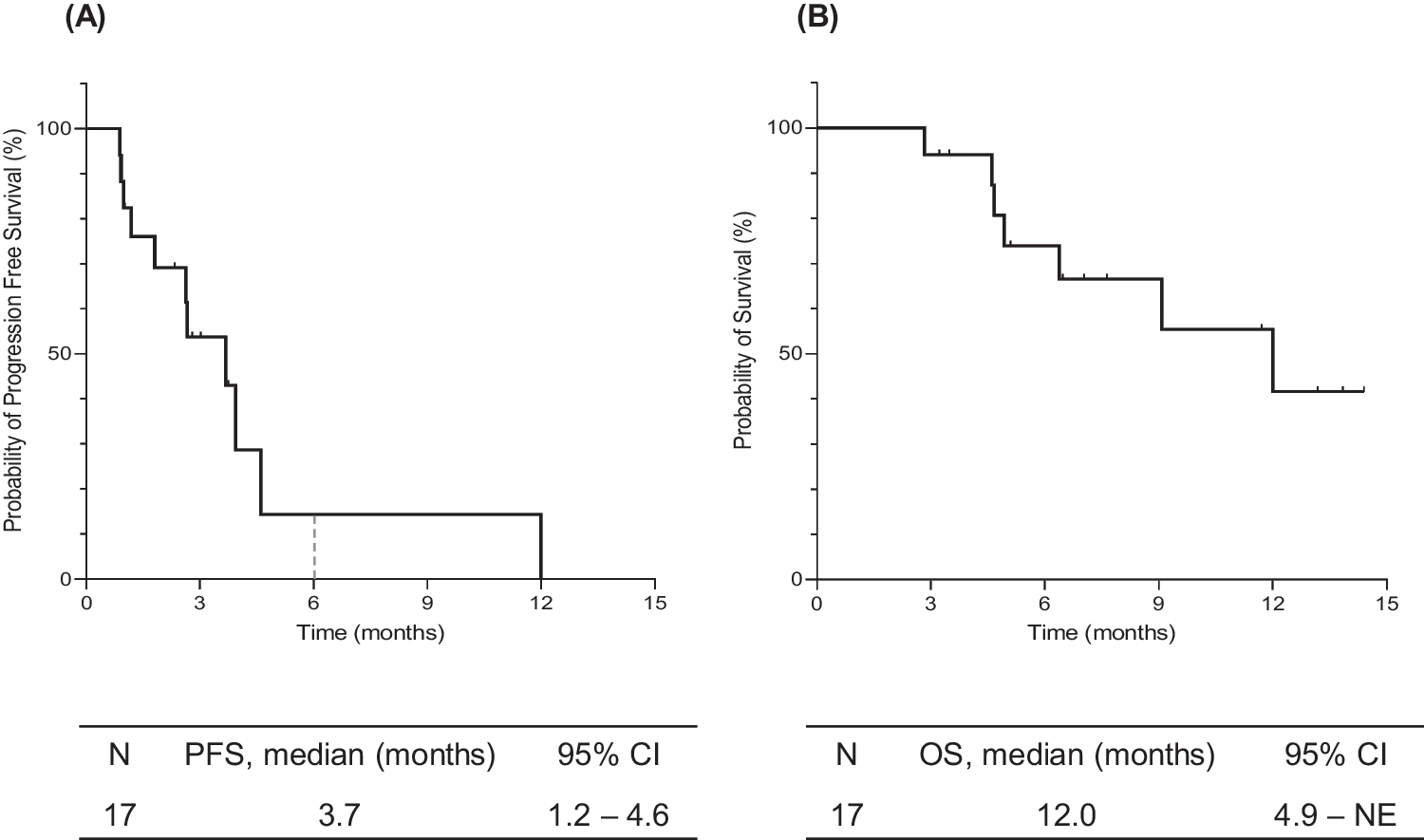
In this study, the median PFS was 15.1 months, which was shorter than that reported in a multicenter, retrospective observational study on Japanese patients (OSI-FACT study) in which osimertinib as a first-line therapy showed efficacy with a median PFS of 20.5 months [10]. Additionally, the median OS was 34.5 months, which was a little shorter than 38.6 months in the FLAURA study [7]. The reason why the PFS and OS observed in this study were shortened compared with those in previous studies might be related to the high incidence rate of ILD. In this study, the incidence rate of ILD was 28.2% (24/85), which was more than two times as frequent as that in the FLAURA study (12.3%) [5]. Additionally, the discontinuation rate due to ILD was 18.8% (16/85), which was more than 1.8 times as frequent as that in the OSI-FACT study (10.4%) [10]. Previous reports have shown that PFS is significantly shorter, and OS tends to be shorter in patients with ILD than in those without ILD in Japanese patients [18]. The high treatment discontinuation rate due to ILD may have affected the lower efficacy of this study compared with previous reports. In this study, the multivariable analysis revealed that the independent factors for PFS shortening were pleural and liver metastasis. This finding is consistent with a previous report [10]. Additionally, the independent factors for PFS prolongation were exon 21 L858R and dose reduction within 6 months. Generally, exon 19 deletion is associated with greater antitumor efficacy of EGFR-TKIs than exon 21 L858R [19]. PD-L1 TPS ≥ 50% is a poor prognostic factor for osimertinib therapy [10]. In this study, the rate of PD-L1 TPS ≥ 50% in patients with exon 19 deletion was about twice as high as that in patients with exon 21 L858R, which caused reduced efficacy in patients with exon 19 deletion.
This study has some limitations. First, this was a single-center retrospective study with a small sample size. Thus, the results cannot be considered definitive. Second, the performance status of each patient was not available in the electronic medical records. Third, in the multivariable analysis, PD-L1 TPS, which has been reported as a prognostic factor [10], could not be included as an explanatory variable because many cases were unknown.


留言 (0)