In this phase 1b trial, the safety profile, pharmacokinetic characteristics, and preliminary efficacy of HR070803 combined with 5-FU and LV were assessed in patients with advanced solid tumors. DLTs that occurred were associated with myelosuppression, and the MTD of HR070803, which is also the recommended phase 2 dose, was determined to be 60 mg/m2. The pharmacokinetic results indicated that compared with conventional nonliposomal irinotecan injection, the Cmax of SN-38 in HR070803 was lower, and the t1/2 was longer. In terms of treatment efficacy, 2 patients had confirmed PR, 2 patients had unconfirmed PR, and 9 patients had SD.
Because irinotecan damages blood cells, epithelial cells, and commensal bacteria, treatment with irinotecan is commonly accompanied by hematologic and gastrointestinal toxicities [1]. In our study, both DLTs observed were myelosuppressive (neutropenia and febrile neutropenia), and no gastrointestinal DLTs occurred; this result might be attributed to the small sample size and interpatient variations. A phase 1 study assessed the MTD, pharmacokinetics and preliminary efficacy of PEP02 in combination with 5-FU and LV when administered every 3 weeks in patients with advanced solid tumors [12]. The DLTs were myelosuppression and gastrointestinal events, including diarrhea, neutropenia, infection with hypotension, and hemorrhage. Another phase 1 study evaluated the MTD, pharmacokinetics, and preliminary efficacy of irinotecan liposome injection (LY01610) when administered Q2W in patients with advanced esophageal squamous cell carcinoma [10]. The DLTs observed were vomiting and febrile neutropenia [10]. The DLT results from the abovementioned phase 1 MTD exploration studies of liposomal irinotecan indicated that nanoliposome encapsulation did not impact the safety profile of irinotecan and, more importantly, did not cause new safety concerns.
In recent years, several phase 1 studies of liposomal irinotecan, used either as monotherapy or in combination with other therapeutic agents, have been conducted in patients with various tumors, such as metastatic breast cancer [13], advanced esophageal squamous cell carcinoma [10], recurrent high-grade glioma [9], pancreatic ductal adenocarcinoma [14], and advanced refractory solid tumors [4, 12]. The MTDs of different liposomal irinotecan formulations in these studies ranged from 50 mg/m2 to 120 mg/m2, whereas it was determined to be 60 mg/m2 in this study. The disparities in MTD might be attributed to different treatments, administration schedules, tumor types, and nanoliposome formulations as well as interpatient variation.
No new safety signals were identified with HR070803 compared with conventional irinotecan injection [7, 8]. Most TEAEs were of grade 1 or 2 severity, and they were resolved after appropriate supportive therapies or dose interruptions. No patients discontinued treatment due to TEAEs, and no deaths occurred. Cholinergic reactions can occur upon injection of irinotecan [7, 8, 15, 16]. However, in this study, no cholinergic syndrome was observed. The manageable and tolerable safety profile of HR070803 plus 5-FU/LV renders it a feasible treatment modality for patients with advanced solid tumors.
The pharmacokinetic parameters of HR070803 monotherapy at 80 mg/m2 in our previous phase 1a study (undisclosed data) and HR070803 plus 5-FU/LV at 80 mg/m2 in this study were similar, suggesting that 5-FU and LV exerted weak effects on the pharmacokinetic profile of HR070803. Compared with a previous study that assessed plasma SN-38 concentrations after the injection of nonliposomal irinotecan at 180 mg/m2 (Q2W) [17], the mean Cmax of SN-38_LAC after administration of HR070803 at the MTD (60 mg/m2) was much lower (3.22 ng/mL vs. 26.2 ng/mL), as was its mean AUC0∍∞ (191 h·ng/mL vs. 368 h·ng/mL). The t1/2 of SN-38_LAC was longer after HR070803 administration compared with that after conventional irinotecan injection (mean value: 37.0 h vs. 19.7 h). Both irinotecan and its metabolite SN-38 exist in equilibrium between an active lactone form and an inactive carboxylate form, depending on the pH and binding proteins, after intravenous injection [4, 12, 18]. An acidic pH, such as that found in the tumor microenvironment, promotes the formation of the active lactone form. A liposome-encapsulated formulation could theoretically shift the equilibrium, resulting in greater amounts of the active lactone form within tumor tissue, enhancing the activity of irinotecan [5]. In this study, in addition to total irinotecan and active SN-38_LAC, we also assessed the plasma concentrations and AUCs of CPT-11_LAC, CPT-11_CAR, and SN-38_CAR, which made it possible to perform comparisons between the active LAC form and the inactive CAR form of irinotecan and SN-38. At the MTD (60 mg/m2), the mean AUC0 − t of CPT-11_LAC was approximately 19fold greater than that of CPT-11_CAR. The mean ratio of lactone to total free CPT-11 was > 90% after HR070803 administration, which compared favorably with the ratio of 34-44% observed after the administration of the nonliposome formulations [18, 19]. The mean AUC0 − t of SN-38_LAC was approximately 2-fold greater than that of SN-38_CAR. These results were consistent with previous findings showing that the lactone form of SN-38 accounted for approximately 60–70% of the total plasma SN-38 levels after the intravenous injection of irinotecan [18].
The active metabolite of irinotecan, SN-38, is inactivated and detoxified by the UGT enzyme, which is encoded by the UGT1A1 gene [20]. Reduced UGT enzyme activity caused by genetic variation, such as the homozygous UGT1A1*28 allele, leads to decreased detoxification and persistence of SN-38, thus resulting in increased toxicity [20]. Considering that this study aimed to determine the MTD of HR070803 in combination with 5-FU/LV, patients with homozygous UGT1A1*28 were excluded. There were 5 patients who were heterozygous for UGT1A1*28 in this study. We also assessed the UGT1A1*6 variation in the patients. There was 1 patient with homozygous UGT1A1*6 who experienced febrile neutropenia and 3 patients with heterozygous UGT1A1*6. No patients had concurrent mutations in UGT1A1*6 and UGT1A1*28. In patients with UGT1A1*6/28 mutations, the safety and pharmacokinetics results were similar to those in patients who expressed the wild-type gene. However, owing to the small sample size, these results should be interpreted with caution. Future PK/pharmacodynamic studies are warranted to draw firm conclusions on the correlations between UGT1A1 gene polymorphism and the tolerability and pharmacokinetics profiles of HR070803.
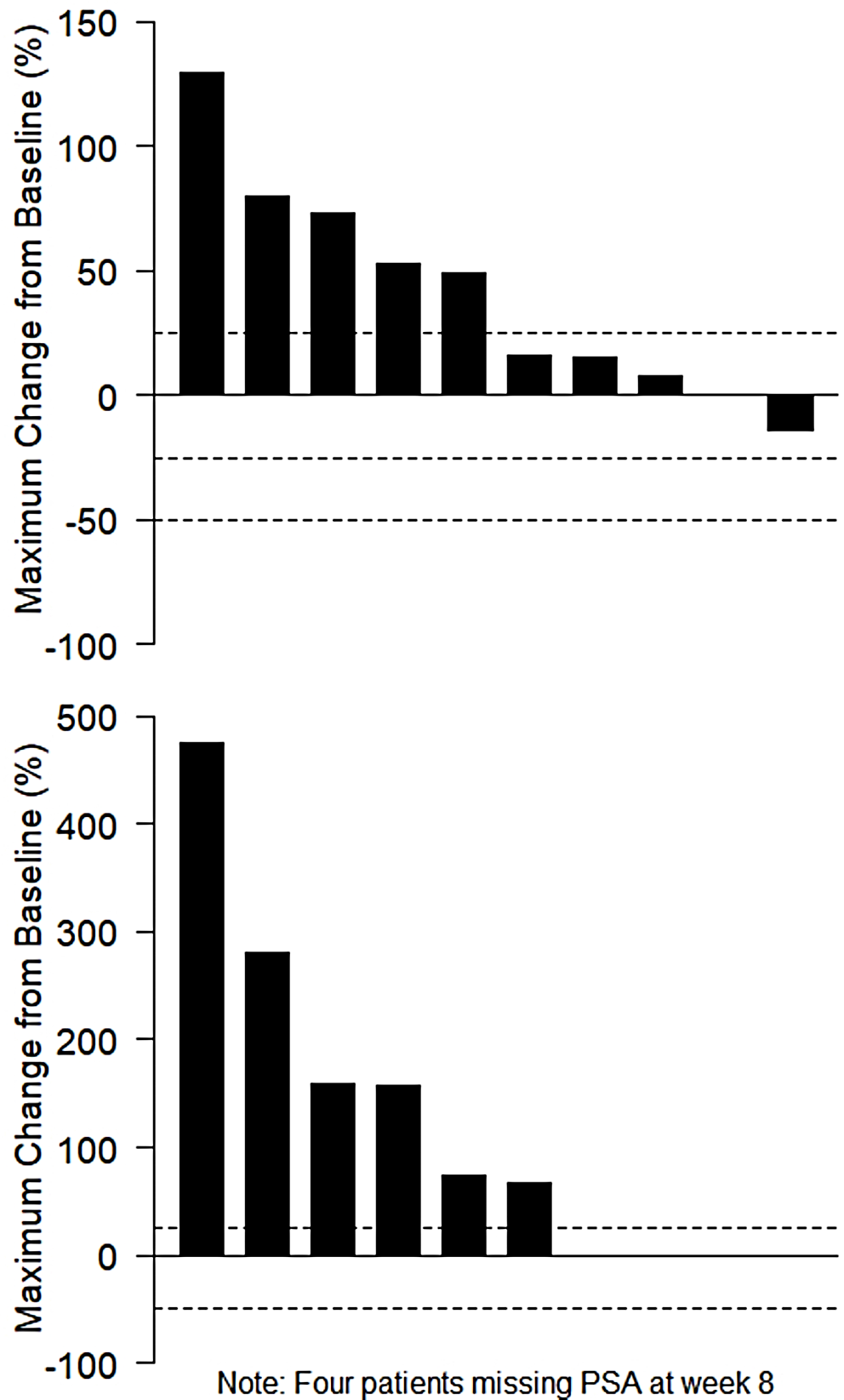
Although the interpretation of the efficacy results was limited by the small sample size and heterogeneous tumor types, the ORR (13.3%) and DCR (73.3%) results indicated the potential antitumor activity of HR070803 in combination with 5-FU/LV. Indeed, a randomized, double-blinded, parallel-controlled, phase 3 study (NCT05074589) was conducted to evaluate the efficacy and safety of HR070803 plus 5-FU/LV versus placebo plus 5-FU/LV as the second-line therapy for gemcitabinerefractory locally advanced or metastatic pancreatic cancer. Treatment with HR070803 plus 5-FU/LV resulted in statistically significant and clinically meaningful prolonged OS versus placebo plus 5-FU/LV, and the safety profile was manageable [21].
In conclusion, the DLTs observed in this study were associated with myelosuppression. The MTD of HR070803 was determined to be 60 mg/m2 (Q2W) when it was combined with 5-FU and LV, and this is also the recommended dose for future studies. HR070803 in combination with 5-FU and LV had a manageable safety profile and promising antitumor activity in patients with advanced solid tumors. Compared with conventional nonliposomal irinotecan, HR070803 administration resulted in a lower Cmax and prolonged t1/2 of SN-38 owing to nanosized liposome encapsulation.





留言 (0)