
記住我


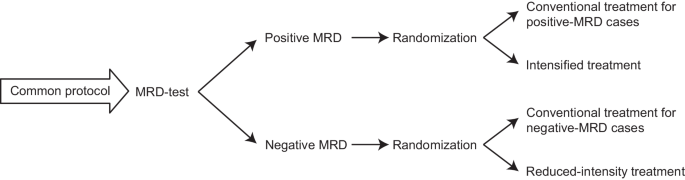

Major patient characteristics and a diagram describing patient flow with regard to RT are shown in Table 1 and Fig. 1. Median follow-up of all patients was 9.3 years.
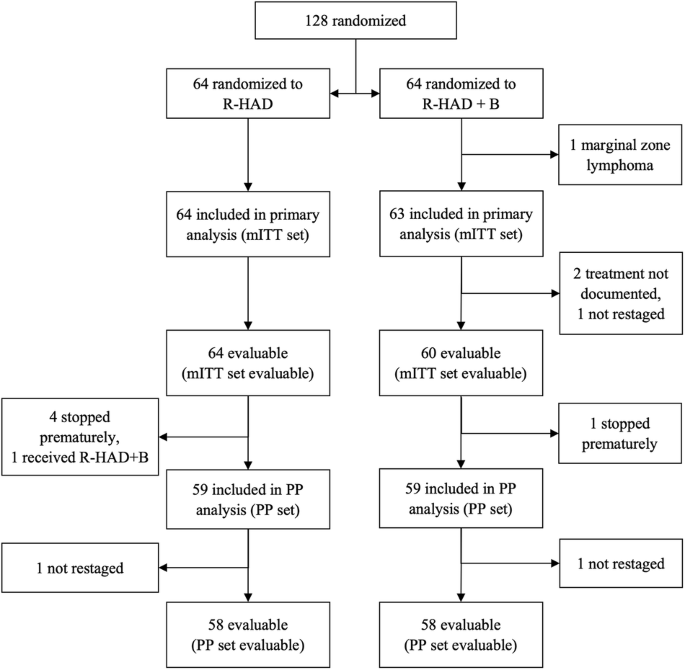
Table 1 Patient characteristics for the whole study population and patients with bulky disease in comparison between the group undergoing radiotherapy (RT) and the group without RT (no-RT).Fig. 1: Consort diagram.
Consort diagram displaying patient numbers included within the study with or without radiation treatment and numbers for extranodal and bulky disease.
RadiotherapyOne-hundred-twenty of 261 patients (46%) were irradiated, 52 of whom had reached a complete (CR) or unconfirmed complete remission (CRu) according to the Cheson criteria [18] at the end of immunochemotherapy, 50 patients were irradiated for PR or less than PR at the end of immunochemotherapy (18 patients with unknown response after chemotherapy; Supplementary Table 1). Patients with RT were predominantly male (66%), almost uniformly showed an elevated LDH (97%), about two-thirds had ECOG scores of 0-1 (65%) (Table 1). Compared to the no-RT group, there were more patients in stage I/II in the RT group (1% vs. 7%, for the no-RT vs. RT-group, respectively). These early-stage patients uniformly had bulky disease.
RT was administered to 49.6% of patients in the R-CHOEP arm and 42.4% in the Mega-CHOEP arm (p = 0.244). Twenty-six (50%) and 26 (50%) patients were irradiated after reaching a CR/CRu, 32 (64%) and 18 (36%) patients received RT for insufficient response (PR, SD) in the R-CHOEP and the R-MegaCHOEP arm, respectively. 47% and 43% of patients with aaIPI 2 and 3 were irradiated with no difference in aaIPI between the irradiated and the no-RT group (p = 0.540).
The regions most frequently irradiated were mediastinum (50), paraaortic (27), and mesenteric (15) regions, followed by left iliac lymph nodes (12) and bone (12). Median RT dose was 36 Gy (5.4 Gy- 46 Gy) with single doses of 1.8 Gy (1.5 Gy–2 Gy).
Extranodal involvement occurred most frequently in the pleura (29), pericardium (26), spleen (24), lungs (23) and skeleton (13 below and 5 above the diaphragm, 4 both). Bulky disease at diagnosis was present in 103 of 120 irradiated patients in comparison to 54 of 141 patients in the non-irradiated group (Table 1). In the RT-group, bulky disease had a maximum width of 7.5–20.0 cm (median: 11.0 cm, lower quartile: 9.0 cm, upper quartile: 14.2 cm). Bulky disease was located predominantly in the mediastinal (44), paraaortic (17) and mesenteric (13) region. A second and third bulk was found in 21 and 5 patients, respectively. The main location for a second bulk was the paraaortic region (7), there was no predominant pattern for a third bulk (5 different regions). Of the 103 patients irradiated with bulky disease, 101 (98%) were treated according to protocol (2 for other reasons). Characteristics of all patients with bulky disease both in the RT and the no-RT group are displayed in Table 1.
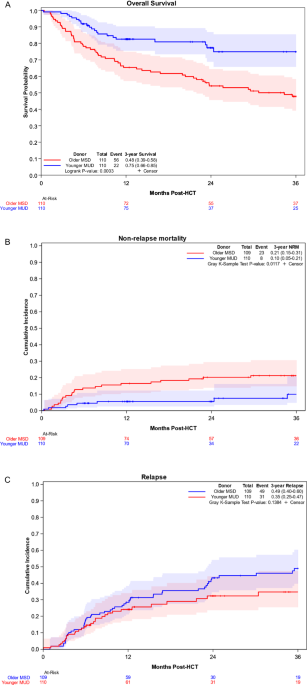
OutcomesOutcomes—intention-to-treat (ITT) populationFor the ITT population, 10-year EFS was 54% (95%-confidence interval (95%-CI): 48–61%), 10-year PFS was 60% (95%-CI: 53–67%) and 10-year OS was 69% (95%-CI: 63–76%). There were significant differences for patients treated with RT in comparison to the group without RT regarding EFS (64%, 95%-CI: 54–74% vs. 46%, 95%-CI: 36–56%; p = 0.001) and PFS (67%, 95%-CI: 58–77% vs. 54% 95%-CI: 44–64%; p = 0.025) but not OS (73%, 95%-CI: 63–82% vs. 66%, 95%-CI: 57–75%; p = 0.132; Fig. 2A–C). Limiting the analysis to patients with a CR/CRu after completion of immunochemotherapy, patients with RT did not differ significantly compared to the non-irradiated group regarding EFS (p = 0.798), PFS (p = 0.692) and OS (p = 0.367). For patients with DLBCL, there was a significant improvement in 10-year EFS with RT (p = 0.019). As there has been no randomization concerning RT, we further compared the outcomes in the two treatment arms within the RT-group. There were no differences in EFS (p = 0.816), PFS (p = 0.555) or OS (p = 0.190).
Fig. 2: Survival curves for the intention-to-treat population and patients with bulky disease.
A–C Survival curves for the whole patient collective. Event-free survival (A), progression-free survival (B) and overall survival (C) for the patients undergoing RT (red) in comparison to those without RT (blue). Outcomes were compared after a 10-year follow-up and compared using a log-rank test. D–F Survival curves for patients with bulky disease. Event-free survival (D), progression-free survival (E) and overall survival (F) for the patients undergoing RT (red) in comparison to those without RT (blue). Outcomes were compared after a 10-year follow-up and compared using a log-rank test.
Outcome—extranodal and bulky diseaseConsidering extranodal lesions only, there was a difference in EFS (10-year EFS: 62%, 95%-CI: 51–72% for patients with RT vs. 51%, 95%-CI: 40–62% for patients without RT; p = 0.017) but not in PFS or OS (PFS: p = 0.068; OS: p = 0.305). In contrast, we observed significant differences in all survival endpoints for patients with bulky disease. Ten-year EFS (64%, 95%-CI: 54–75% vs. 35%, 95%-CI: 16–53%; p < 0.001), 10-year PFS (68%, 95%-CI: 58–78% vs. 47%, 95%-CI: 30–65%; p = 0.003) and most importantly 10-year OS (72%, 95%-CI: 61–82% vs. 59%, 95%-CI: 45–73%; p = 0.011; Fig. 2D–F) were all significantly better for patients with RT.
As in the group of patients with bulky disease, there was an imbalance regarding IPI categories between irradiated and non-irradiated patients (see Table 1), further analyses were done. There was a significant improvement in 10-year EFS for patients with bulky disease undergoing RT with an aaIPI of 2 (68%, 95%-CI: 57–79% vs. not reached; p < 0.001), but not with an aaIPI of 3 (p = 0.296) (Fig. 3A, B). Similar results were observed for PFS and OS when patients with aaIPI 2 and 3 were analyzed separately (data not shown). To exclude confounding by early termination of chemotherapy, an analysis of patients with bulky disease who completed immunochemotherapy as intended was done confirming a significant improvement in EFS with RT (10-year EFS: 66%, 95%-CI: 51–74% vs. 37%, 95%-CI: 5–69%; p = 0.017; Fig. 3C). However, for patients with bulky disease reaching a CR/CRu after systemic therapy, no difference in EFS was found with the use of RT (p = 0.693). Limiting the analysis to patients with DLBCL did not alter the impact of RT on outcome parameters (EFS: p < 0.001; PFS: p = 0.016; OS: p = 0.026). Also in the bulky subgroup, no differences in outcomes between the two treatment arms were found for the irradiated patients (EFS: p = 0.952; PFS: p = 0.699; OS: p = 0.121).
Fig. 3: Survival curves for subgroups of patients with bulky disease.
Event-free survival (EFS) for patients undergoing RT (red) in comparison to those without RT (blue). Subgroups of patients with an age-adjusted international prognostic index of 2 (A) or 3 (B) or with completion of chemotherapy as intended (C), respectively. Outcomes were compared after a 10-year follow-up and compared using a log-rank test.
Protocol violationsOnly one patient not qualifying underwent RT; in contrast, forty patients assigned to RT as per protocol did not receive it as a protocol violation. Twenty-one of these patients had an extranodal involvement being amenable to RT and 19 revealed a bulky disease (with no prior R0-resection). Thirty-one of forty patients (77.5%) had at least one localization challenging to irradiate (gastrointestinal tract, lungs, pancreas, pleura, reproductive organs, or the central nervous system). Other reasons for radiation not to be carried out were insufficient response to immunochemotherapy (19 patients), excessive toxicity (11 patients), patients wish (5 patients) or other (3 patients; Fig. 1).
To estimate the impact of patients who did not receive RT by protocol violation, we compared the patients undergoing RT with the non-irradiated group after exclusion of these 40 patients. The results obtained after exclusion of patients with protocol violations were comparable overall (EFS: p < 0.001; PFS: 0.003; OS: 0.043) and in the subgroup with bulky disease (EFS: p < 0.001; PFS: p < 0.001; OS: p < 0.001).
ToxicitiesToxicities attributed to RT were mostly mild to moderate with 24 grade 3 and 8 grade 4 toxicities (Table 2). Most toxicities, especially of grades 3 or 4 were hematologic (19/24 and 8/8, respectively), with leukocytopenia being most frequently reported (14 and 6 cases, respectively). Typical RT-associated acute side effects like skin toxicities or dysphagia were limited to grade 1 and 2 (28 and 3 or 23 and 6 cases, respectively). The previously reported toxicities of immunochemotherapy and RT included grade 3–4 mucositis in 8.3% (R-CHOEP) and 64.8% (R-MegaCHOEP) of patients, respectively [8]. All patients in the high-dose therapy arm had grade 4 leukopenia and grade 3–4 thrombocytopenia in comparison to 58.5% leukocytopenia and 33.8% grade 3–4 thrombocytopenia in the R-CHOEP arm [8].
Table 2 Overview on acute toxicities documented during radiotherapy.Secondary malignanciesAfter a median observation period of 51 months (8 months–148 months), 23 secondary malignancies in 22 patients have been reported, with 13 cases in 12 patients in the RT group (5 leukemias/myelodysplastic syndromes, 1 case each of melanoma, endometrial cancer, Hodgkin lymphoma, cancer of oral cavity, epidermoid cancer of the scalp, thyroid cancer, basal cell carcinoma of the nose, and cancer of unknown primary). The rate of secondary malignancies did not differ significantly between patients with and without RT, respectively (10.1% vs. 7.1%; p = 0.504). However, all but one of the leukemias/myelodysplastic syndromes reported occurred in patients who had received both immunochemotherapy and RT. In two patients secondary malignancies occurred in areas which had been irradiated, 1 case of Hodgkin lymphoma and 1 case of thyroid cancer following mediastinal irradiation after an observation time of 31 and 102 months, respectively.
留言 (0)