Research design
This study was designed to examine the association between HF and intestinal inflammation caused by a disturbance in the intestinal microbiota in infants with CHD. Left-to-right shunt CHD is the most common type of CHD, accounting for approximately 50 to 70% of CHD cases. Severe HF often leads to congestive HF in infants. Infants with left-to-right shunt CHD and congestive HF were selected as the study subjects. This study was the first to examine the relationship between HF and intestinal inflammation in infants with CHD. Since no similar study has been performed, it was difficult to find adequate data in the literature for sample size calculation. Being an exploratory study, here the sample size could not be calculated. Twenty infants with HF and CHD who were admitted to our hospital between October 2021 and March 2022 were included in this study. Twenty age- and sex-matched infants without HF were selected as the control group. We used the modified Ross score and NT-BNP to evaluate the severity of HF.
The inclusion criterion was HF caused by left-to-right shunt CHD. The exclusion criteria were as follows: (1) patients with other serious diseases, such as digestive tract malformation, kidney failure, or liver failure; (2) patients with digestive tract diseases, such as diarrhoea, constipation, or jaundice; (3) patients with infection or who were using antibiotics; and (4) patients whose parents refused to participate in this study.
Faecal sample collection
Fresh faecal samples were obtained using a faecal collector and were transported in a liquid nitrogen tank. The faecal samples were stored in at − 80 ℃.
Experimental methods16 S rDNA sequencing
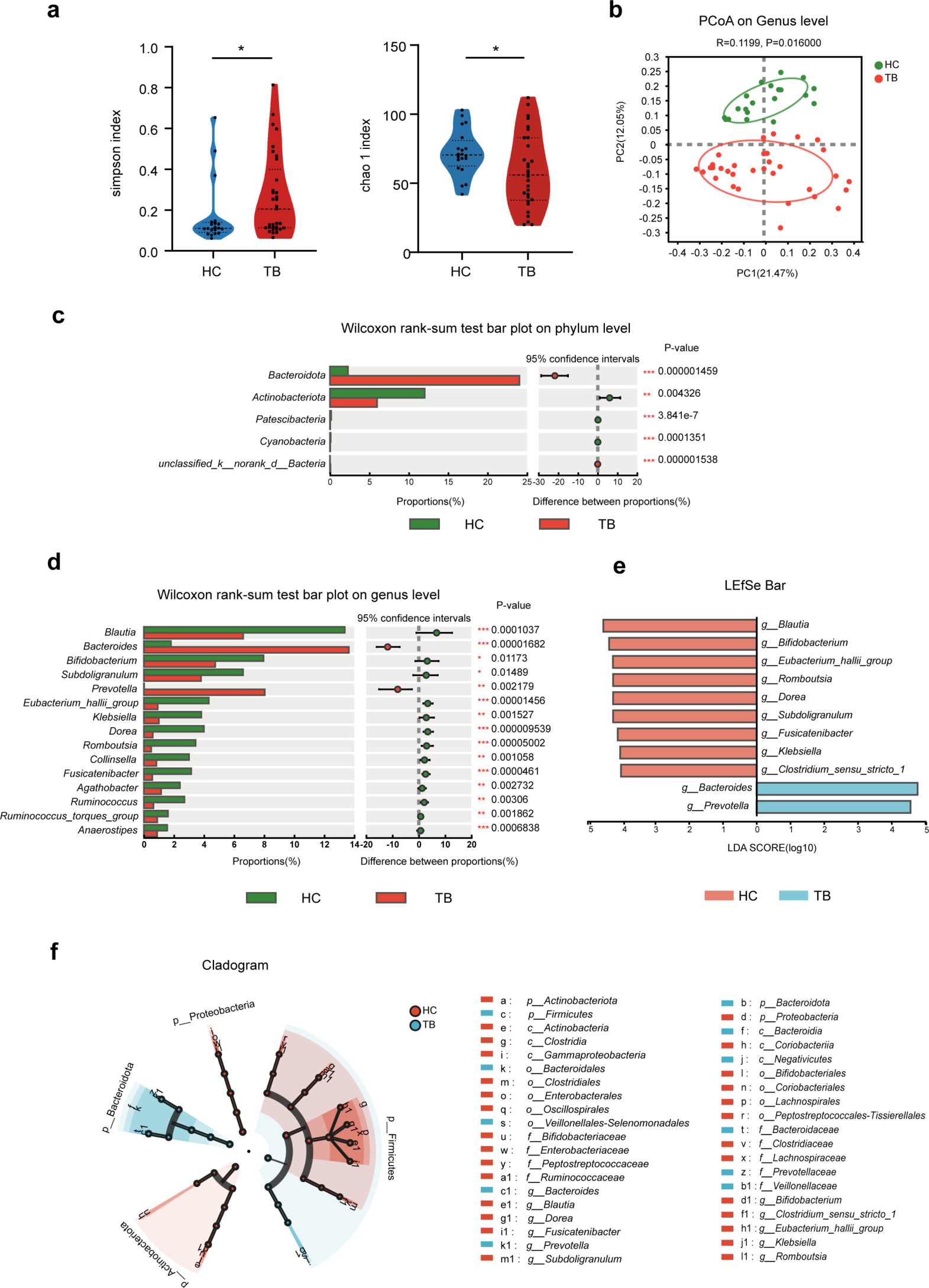
Total genomic DNA samples were prepared with the M5635-02 OMEGA Soil DNA Kit (Omega Bio-Tek, Norcross, GA). The extracted DNA was selected as a template. PCR amplification of bacterial 16 S rRNA genes (V3–V4 region) was performed, and a PCR amplification library was subsequently constructed. A NovaSeq 6000 SP Reagent Kit (500 cycles) from Suzhou PANOMIX Biomedical Tech Co., Ltd., was used for sequencing on the Illumina NovaSeq platform. The sequence data were analysed by using the QIIME2 and R packages (v3.2.0).
Enzyme-linked immunosorbent assay (ELISA) analysis of intestinal inflammatory factors
Intestinal inflammatory factor levels were measured with ELISA kits. Human interferon IL-1β, IL-4, IL-5, IL-6, IL-8, IL-10, IL-12, IL-17 A, IFN-α, IFN-γ, and TNF-α ELISA kits were used to determine the levels of IL-1β, IL-4, IL-5, IL-6, IL-8, IL-10, IL-12, IL-17 A, IFN-α, IFN-γ and TNF-α, respectively, in the faecal samples.
The faecal samples were maintained at 2–8 °C after being thawed. PBS (pH 7.4) was added, and the samples were homogenized by hand or with grinders and centrifuged for 20 min at 2000–3000 r.p.m, after which the supernatant was removed. After packaging, one aliquot was tested, and the rest was frozen for later use. Standard and test sample wells were established, and 50 µl of the standard was added to the standard wells. Blank wells were also established for comparison. Neither the sample nor the HRP-conjugated reagent was added to these wells; otherwise, these wells were subjected to the same process. In total, 10 µl of the test sample was added to 40 µl of solution in each test sample well (the final dilution was 5-fold) without touching the well wall; the sample was then gently mixed.
Next, 100 µl of HRP-conjugated reagent was added to each well except for the blank wells. The plate was sealed with a membrane and incubated for 60 min at 37 °C. The plate was then uncovered, the liquid was discarded, the plate was air dried, and wash buffer (a wash solution diluted 20-fold in distilled water) was added to each well. After 30 s, the wells were drained, and the wash step was repeated 5 times before the plate was patted dry.
Chromogen Solution A (50 µl) and Chromogen Solution B were added to each well, and the plate was protected from light for 15 min at 37 °C. The reaction was stopped by adding 50 µl of a stop solution to each well (the blue colour changed to yellow). A blank well was used to zero the analyser, and the absorbance was measured at 450 nm within 15 min of adding the stop solution. The levels of intestinal inflammatory factors were calculated by comparing the OD450 values of the samples to a standard curve.
Cardiac function scores of infants
Cardiac function was assessed using the modified Ross scale. There were 6 score indicators: the participant’s sweating position, frequency of rapid breathing, breathing condition, respiratory rate, heart rate and liver size. Each item was scored as 0, 1 or 2 according to the severity of symptoms from mild to severe. A higher score indicated more severe HF. A total score of 0 ~ 2 indicated “no HF”; a total score of 3–6 indicated “mild HF”; a total score of 7–9 indicated “moderate HF”; and a total score of 10 to 12 indicated “severe HF [13].”
Statistical analysis
SPSS 25.0 was used to perform the statistical analysis. Categorical variables were compared by Fisher’s exact test. Comparisons between groups of continuous variables with a normal distribution deviation were performed with the T test. Continuous variables without a normal distribution deviation were compared with the Mann‒Whitney U test. Pearson’s test was used for correlation analysis between two variables.




留言 (0)