
記住我

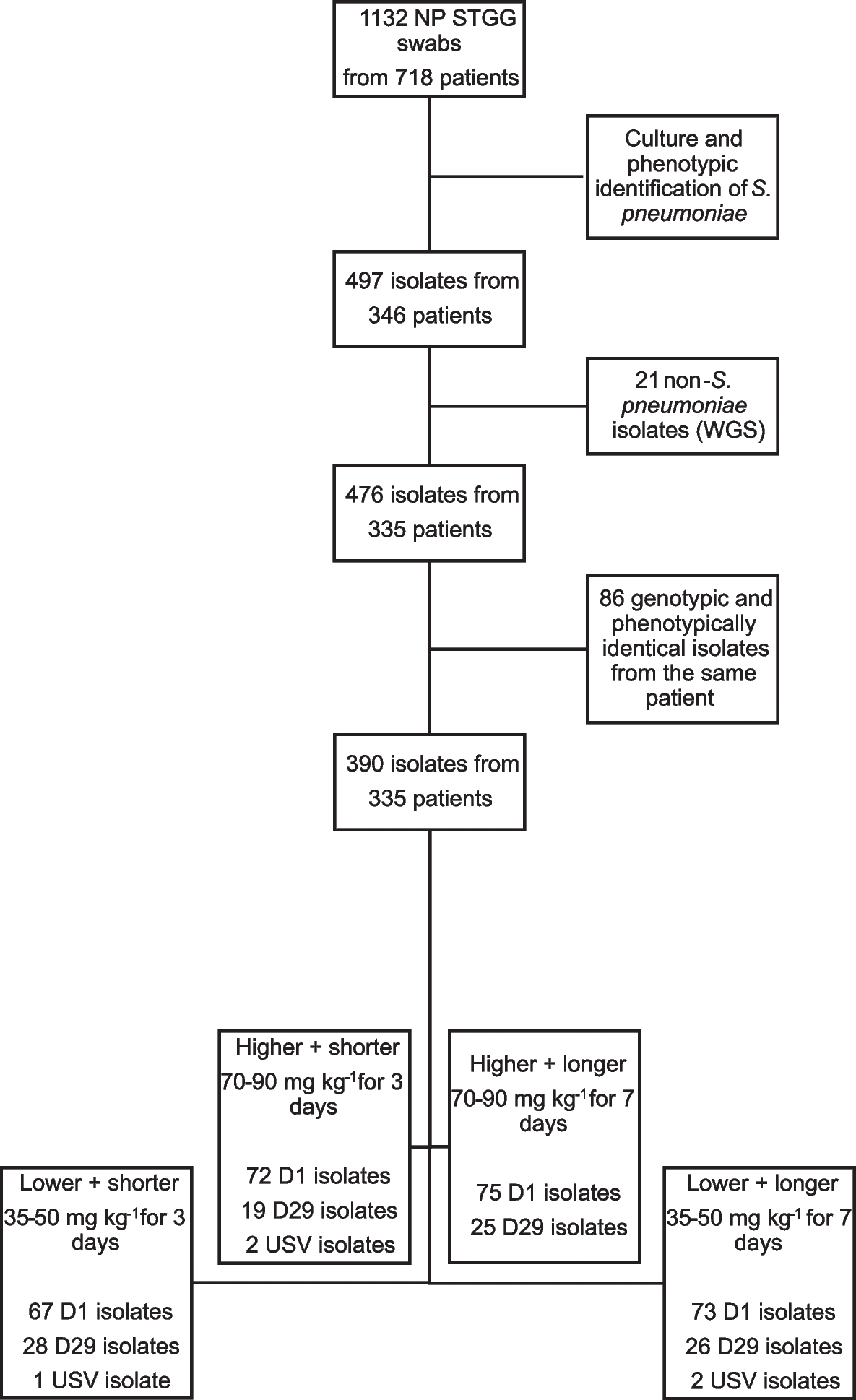


A retrospective study was conducted from December 2018 to December 2019. Data from September 2016 to December 2019 on TB status were extracted from the registers in TB-NRL. We included in this study data of 5267 TB presumptive people previously diagnosed using three consecutive samples and having culture and SD Bioline results with or without Microscopy and reverse hybridization-based LPA (GenoType Mycobacterium CM and GenoType Mycobacterium AS) results. The data on comorbidities and history of people infected with NTM were then checked (Fig. 1).
Fig. 1
Flow diagram showing study population
Study locationThe study was conducted at the TB-NRL for Bacteriological analysis of samples and JHY for clinical evaluation of confirmed NTM patients.
The TB-NRL is located at the Mycobacteriology Unit of the Centre Pasteur du Cameroun (CPC). The TB-NRL have a technical platform for TB bacteriological analysis using WHO recommended rapid diagnosis (WRD), TB-LAMP and Xpert MTB/ RIF; BACTEC MGIT 960 for Culture and drug susceptibility testing (DST) and NTM bacteriological analysis using reverse hybridization-based LPA, GenoType Mycobacterium CM and GenoType Mycobacterium AS (Hain Lifescience, Nehren Germany). This laboratory received samples from presumptive TB and NTM cases coming from about 93 Diagnosis and Treatment Centers (DTC) from 03 regions of Cameroon (Centre, Est and South) for Culture and DST analysis.
The JHY is a reference hospital for pneumology and a DTC of Yaounde and its surrounding areas. JHY is also specialized in the management of patients infected with multi-drug-resistant M. tuberculosis. The hospital provides diagnostic tests for TB using sputum smear microscopy and TB-LAMP tests.
The CPC and Jamot hospital are in close vicinity and have a long history of collaborative research.
Routine laboratory processMicroscopyMicroscopy was performed as described previously by Donfack et al. [7]. Sample was first smeared on a glass slide and fixation was conducted by heating on the fire. This was then flooded with auramine followed by adequate rinsing with water and discoloration with acid-alcohol solution (3% V/V). It was then rinsed well with water, stained with methylene blue (1% V/V), dryed and visualized under fluorescence microscopy.
TB-LAMP assayThe test was carried out with the HumaLoop T(Eiken Chemical Company Ltd, Japan) according to the WHO guideline [8]. The 60 µl sample was transferred to a heating tube and incubated at 90 °C for 5 min. After inactivation, the sample was mixed well with absorption powder and 30-μL DNA solution was extracted and placed in a reaction tube, and loop-mediated isothermal amplification was performed at 67 °C for 40 min. A positive control tube containing sputum with AFB and a negative control tube containing bacilli-free artificial sputum were used for each manipulation. Positive result was characterized by the presence of strong fluorescence in the tube, which was not released from the negative reaction.
Xpert MTB/RIF assayThe Xpert MTB/RIF assay was performed according to manufacturer’s instruction [9]. Sample reagent was added using a double volume of the sample, homogenized and incubated for 15 min at room temperature with mixing intervals. After inactivation, 2 ml of the treated sample was transferred to the cartridge containing all the reaction mixture and loaded to the GeneXpert instrument. An automatic process completed the remaining assay steps and the results were interpreted.
CultureThe culture was carried out using the automated system BACTEC MGIT 960 Mycobacteria detection system as recommended by the manufacturer. Samples were decontaminated in N-acetyl-l-cysteine-sodium hydroxide and 500 µL of the decontaminated sample was inoculated into a MGIT medium, incubated for 42 days in the MGIT™ 960™ instrument and the appearance of the colonies was then observed [10].
Identification of Mycobacterium tuberculosis complexImmunological identification of isolates was done by rapid detection of MPT64 antigen with the immunochromatographic assay, (SD Bioline assay, Kyonggi, Korea). The SD Bioline assay was performed with acid fast bacilli in MGIT medium as described by the manufacturer [11]. A positive test confirmed the species of MBTC. All culture isolates which were negative for immunochromatographic assay were submitted for NTM identification.
Hybridization-based line probe assayCulture isolates with a negative results for SD Bioline assay were processed first for primary identification using reverse hybridization-based line probe assay, GenoType Mycobacterium CM (Hain Lifescience, Nehren Germany), then the GenoType Mycobacterium AS for culture isolates which were negative to GenoType Mycobacterium CM. The process was performed as recommended by the manufacturer and was consisted of an extraction, amplification and hybridization [12].
Statistical analysisData was entered into the software Excel 2010 and validated by double entry and comparison. The frequencies were determined and the graphs were then plotted.
Ethics approvalThis study was approved by the Cameroon National Ethics Committee for Human Health Research under the number N°2017/02/872/CE/CNERSH/SP. Patient identifying information was removed prior to analysis. As this was a study of routinely collected data, patient consent was not required.
留言 (0)