
記住我






 Figure
Figure Box 1
Box 1Esophageal cancer, the eighth most common cancer in the world, continues to have a poor prognosis and a low 5-year survival rate.1 Compared with 2020, the number of new cases globally is projected to increase 31.4% by 2030 and 63.5% by 2040. The incidence and type vary geographically but almost 80% of cases occur in areas of lower socioeconomic development that rank low on the human development index (HDI), a score based on life expectancy, education, and gross national income. The two main subsets of esophageal cancer, accounting for 95% of all cases, are squamous cell cancer (SCC) and adenocarcinoma. Esophageal SCC accounts for 90% of esophageal cancer cases worldwide and is found mainly in the Central Asian Esophageal Cancer Belt (extending from Iran to China), Africa, and South America.2,3 Esophageal adenocarcinoma is more predominant in Western countries with high HDI scores but has been rising steadily in other parts of the world.3 Reasons for this are not fully understood but can be attributed to a combination of rising obesity rates and declining smoking prevalence.2
Men over age 50 years are three to four times more likely to develop esophageal cancer than women of the same age, and in the United States, White, Native American, and Black patients are more at risk than those of Hispanic and Asian ethnicity.4,5 Black patients are more likely to develop esophageal SCC; White patients are more likely to develop esophageal adenocarcinoma.6,7 Diagnosis tends to occur between ages 60 and 80 years for both types.7 Esophageal cancer accounts for only 1% of cancer in the United States, and awareness remains poor among clinicians and patients alike because of lack of screening and surveillance recommendations.5,8 This is alarming, considering the rising incidence of esophageal adenocarcinoma in US patients under age 50 years.8
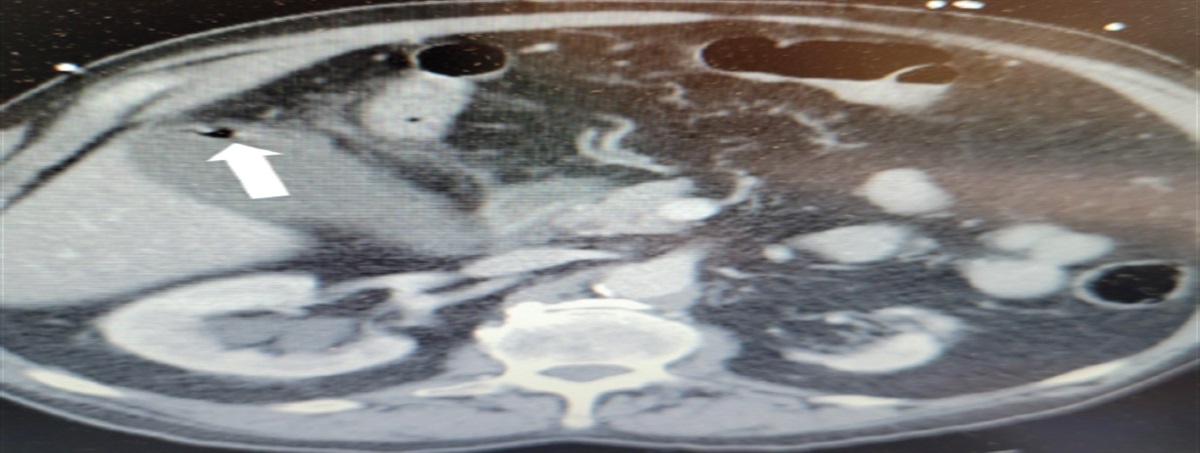
PATHOPHYSIOLOGY AND RISK FACTORSEsophageal SCC and esophageal adenocarcinoma develop in different anatomic locations and have different risk factors (Table 1). As the name implies, esophageal SCC starts in mucosal squamous cells in the upper third of the esophagus; esophageal adenocarcinoma develops in gland cells in the lower third of the esophagus.1 Both types traverse the same anatomical path—inner mucosa, submucosa, muscularis propria, and adventitia—which is a key reason for late-stage diagnosis because early symptoms will be mild or nonexistent (Figure 1).9
TABLE 1. - Risk factors for esophageal SCC and esophageal adenocarcinomaEsophageal SCC
Black ethnicity
Smoking
Daily alcohol consumption
Human papillomavirus
Drinking hot beverages
Poor intake of fruits and vegetables
Exposure to polycyclic aromatic hydrocarbons such as coal, crude oil, gasoline, and smoked products
Rare genetic disorders such as tylosis, Fanconi anemia, or Plummer-Vinson syndrome
Esophageal adenocarcinoma
White ethnicity
Alcohol consumption
Obesity
GERD
Barrett esophagus
Beta-agonist drugs
 FIGURE 1.:
FIGURE 1.: The TNM staging system for esophageal cancer helps determine prognosis and treatment based on tumor depth, number of affected lymph nodes, and metastasis to distant organs.Reprinted with permission from Joseph A, Raja S, Kamath S, et al. Esophageal adenocarcinoma: a dire need for early detection and treatment. Cleve Clin J Med. 2022;89(5):269-279. © 2022 Cleveland Clinic Foundation. All rights reserved.
 Box 2
Box 2The most important risk factors for esophageal SCC are tobacco smoking and alcohol use; for esophageal adenocarcinoma, risk factors are obesity, Barrett esophagus, gastroesophageal reflux disease (GERD), and high dietary fat intake.3,10 The rare genetic disorders tylosis, Plummer-Vinson syndrome, and Fanconi anemia also can predispose patients to esophageal SCC because they involve disorders of squamous cell production.11,12
GERD can lead to Barrett esophagus, dysplasia of gland cells, and esophageal adenocarcinoma in 10% of patients who are not managed properly.7 Drugs known to relax lower esophageal sphincter tone have been suspected to be linked to esophageal adenocarcinoma, but most results are inconclusive, with the exception of beta-agonists, thus increasing the risk of esophageal adenocarcinoma for patients with obstructive pulmonary disease.13 Surprisingly, recent studies have revealed inconclusive results about risk factors that would normally be assumed to be on the list for esophageal adenocarcinoma, namely smoking and Helicobacter pylori infection.7,14,15H. pylori infection has been shown to have protective value in some studies because of atrophy of the gastric corpus and resulting loss of parietal cells and acidity, but overall, results have been variable.15 Moderate alcohol consumption has been proven to have a negative effect on survival for patients with esophageal adenocarcinoma, but no association was found with cigarette smoking.14 These newer findings are speculative and clinicians should continue to adhere to established risk factors set forth by such organizations as the American Cancer Society.16
DIAGNOSIS AND STAGINGDysphagia is the most common presenting symptom and should be followed up with screening questions about smoking history, alcohol consumption, frequency of GERD symptoms, diet, preference of drinking fluid temperature, and medications used for symptoms.17,18 Other symptoms of note include recent weight loss, night sweats, painful swallowing, chest pain/heartburn, and, less commonly, hemoptysis, persistent cough, and hoarseness.18 Physical examination findings may reveal cachexia, cervical lymphadenopathy, organomegaly, and epigastric abdominal pain with palpation.19 A bedside swallow evaluation, in which the patient sips a small amount of water and the process of swallowing is monitored and timed, is a basic screening test with a 95% sensitivity for dysphagia and should be considered in the assessment.18
A fecal occult blood test also can be incorporated into the examination, but a positive result is more likely to be found in later stages.20 Initial laboratory testing can include a complete blood cell count and complete metabolic panel, each having the intent of finding general signs of advanced cancer and/or metastasis such as anemia, elevated hepatic transaminase, or elevated alkaline phosphatase.17,21 Blood biomarker testing such as carcinoembryonic antigen, cancer antigen 19-9, p53, and alpha-fetoprotein can play a significant role in determining the type and progression of esophageal cancer. For example, Zhang and colleagues found a correlation between some rising cancer biomarker levels and the progression of esophageal dysplasia to invasive esophageal SCC.22 However, considering that biomarker tests are still evolving in their accuracy and do not meet the criteria for mass screening use in settings such as primary care, they can be left to the discretion of the gastroenterologist or oncologist, who can correlate these tests with histopathologic findings.17,23,24
After esophageal cancer is suspected, the patient's cancer continuum should begin with an upper endoscopy with biopsies of any suspicious lesions. Upper endoscopy remains the gold standard for screening and surveillance of Barrett esophagus, as well as any clinical presentation suggestive of esophageal cancer.21,25 If the primary suspicion is for esophageal cancer or Barrett esophagus, avoid swallow studies for screening and surveillance because they do not allow for histologic assessment; reserve swallow studies for patients who are poor candidates for endoscopy.25
Noninvasive imaging studies, such as CT, positron emission tomography (PET)/CT, and MRI, can be used in conjunction with other modalities for detection and staging.26 CT often is the first imaging test ordered when evaluating patients for esophageal cancer. It can clearly detect invasion of adjacent structures as well as tumors in the chest, abdomen, and pelvis.27 PET/CT is the modality of choice for local and distant metastasis staging but may not be needed if CT has clearly detected metastasis.27,28 MRI can provide detailed views of esophageal anatomy and has shown promise in regional and local staging, but its overall specificity for esophageal cancer can be low.29,30 All three modalities have proven to be useful when integrated into conventional staging, but each has limitations, including inability to distinguish among T1, T2, and T3 diseases; discrepancies in assessing nodal status; and artifacts from organ movement and blood flow.26 The more invasive endoscopic ultrasound varies greatly in its ability to aid in staging but can be useful in determining whether a tumor has penetrated beyond certain layers of the esophagus.27 Overall, if endoscopy or gastroenterology referral is delayed, or if the patient is a poor candidate for endoscopy, primary care providers (PCPs) should consider moving forward with one or more of these modalities, keeping in mind their limitations.
MANAGEMENTInitial management depends on the patient's clinical stage. The accuracy of the physical examinations, imaging studies, biopsies, diagnostic procedures, and pathology reports are crucial to choosing the right treatment pathway.23,31 The staging system most often used for esophageal cancer is the American Joint Committee on Cancer TNM system, which is based on the extent of the tumor (T), spread to nearby lymph nodes (N), and metastasis (M). Because esophageal cancer can be treated in various ways, different staging systems have been created for pathologic (or surgical) stage, clinical stage, and postneoadjuvant stage. Prefixes are used to indicate the patient's status in the treatment process:
Clinical (cTNM): Based on physical examination, imaging studies, and pathology reports. Pathologic (pTNM): Combines clinical staging and the postoperative report. Posttherapy or postneoadjuvant (yTNM): Staging after systemic treatment and before surgery or if no surgery is indicated. Recurrence or retreatment (rTNM): Staging if cancer returns.23If the patient is in early stages and surgery will be the sole intervention (cT1 N0 M0), minimally invasive resection is typically the first-line treatment.25,32 The preferred method globally for resectable esophageal cancer is the transthoracic esophagectomy with lymphadenotomy.33 This can be successfully accomplished with endoscopic approaches, the two main types being endoscopic mucosal resection and endoscopic submucosal dissection.25 Later stages (cT2-T4 or cN1-3 M0) or more aggressive treatment pathways use surgery plus neoadjuvant or adjuvant chemoradiotherapy (the trimodality approach), as well as types of precision medicine, such as immunotherapy and targeted therapy.32 The recent addition of precision medicine (discussed later) to the trimodality protocols of numerous healthcare institutions has resulted in increased overall survival rates.34,35 However, considering the toxic effects of chemoradiation and the aggressiveness of certain cancer types, surgery should not be delayed if pathologic analysis cannot confirm benefit of any of the options in neoadjuvant treatment.35 Postoperatively, adjunctive chemotherapy and radiation are contingent on the stage of disease but, depending on the extent of surgery and tissue removal, many patients will not recover to the point of being able to tolerate either modality.9 Lastly, recurrence and chemotherapy resistance are common and multifactorial—postoperative surveillance is key and can be tailored based on postoperative pathology results and patient preference.36,37
More than half of patients are unsuitable for resection and have metastatic disease.38 The palliative approach for esophageal cancer focuses on controlling cancer-related symptoms, improving quality of life, and prolonging survival.38 Treatment includes chemoradiotherapy, immunotherapy, and targeted therapy.37 The treatment landscape is broad and because of the numerous options, patients often have a tailored regimen dependent on pathology results. Because of this ever-increasing plethora of treatments and the combinations thereof, there is potential to downstage the tumor, thus facilitating a curative resection not previously possible.39 If cancer-directed treatment is no longer effective and the patient chooses hospice, the focus shifts to controlling common symptoms of esophageal cancer and maintaining patient quality of life.40
POSTTREATMENT AND SURVIVORSHIP PLANSPCPs play a crucial role in coordinating care and recordkeeping for cancer survivors. This can be challenging, especially for underserved patients and those with comorbidities.41 Although all states have cancer registries, the accuracy and sharing of that data with the patient's electronic medical record (EMR) varies immensely from state to state.42 Survivorship plans, developed by the American Society of Clinical Oncology, are simple forms that consolidate patient history and can be of immense value to any clinician participating in the patient's care. Clinicians should consider incorporating a survivorship plan into the EMR to further continuity of care.43
RECENT ADVANCES AND PROSPECTS Precision medicineAlso called precision oncology, this specialty involves the molecular profiling of individual tumors to identify targetable alterations and their expressed biomarkers.44 Now considered the standard of care for many types of cancer, precision medicine has led to better outcomes, more durable responses, increased survival time, and application to treatment protocols alongside other modalities.34,45 The process involves a pathology laboratory sequencing the DNA of biopsied specimens or blood samples and analyzing the expression of their proteins for abnormalities.34 Oncologists can use this information to tailor treatment plans with medications that are more precise in their actions on the type of cancer being targeted. Two examples are trastuzumab and nivolumab. The international Trastuzumab for Gastric Cancer (ToGA) study found that 32% of esophageal adenocarcinoma tumors had an altered ERBB2 gene, a target of the monoclonal antibody drug trastuzumab, which is only approved for the treatment of gastric and gastroesophageal junction adenocarcinoma but routinely is used off-label for esophageal adenocarcinoma.46 When combined with chemotherapy, trastuzumab has been shown to improve pathologic response and reduce the risk of relapse and disease progression.47 Nivolumab, an anti-PD-1 antibody delivered adjunctively in the CheckMate 577 trial, demonstrated improvement in disease-free survival compared with placebo (22.4 months compared with 11 months, respectively) for patients who had received neoadjuvant chemoradiation followed by resection; this drug is now recommended for treatment.48
Sentinel lymph node mappingLymph node metastasis is the single most important prognostic factor and is crucial to staging.49 The gastrointestinal lymphatic system is complex and specific lymph node removal is challenging, so aggressive resections with lymphadenectomies are common because of the fear of missing micrometastases.50 Mapping of the sentinel node, the first lymphatic drainage area from the primary tumor, has helped to prevent unnecessary extensive lymphadenectomy in patients with early esophageal cancer and can lead to better surgical approaches.51
RadiogenomicsAnother example of precision medicine, radiogenomics is defined as the linking of medical imaging with molecular characteristics for the purpose of prognostication.52 Radiogenomics can provide cost-effective, computer-aided diagnosis and treatment guidance and also curb invasive interventions.53 The analysis of diverse large-scale databases containing only quality imaging allows for such uses as tumor region assessment, a task previously performed by a radiologist using only functional and morphologic features. Integrating a radiogenomics workflow of data acquisition, tumor segmentation, feature extraction, analysis, and modeling into the treatment protocol allows for extraction of additional complex information not previously available, all before resection is attempted or chemoradiotherapy initiated.
Palliative measuresDysphagia is a common complaint and serious hurdle for patients, often causing malnutrition and weight loss. A few palliative measures exist and often are used in combination. Self-expanding metal stents can be placed endoscopically over esophageal lesions, generally without the need for dilation, and can provide rapid relief.38 Intraluminal brachytherapy, a form of radiotherapy, applies a stent over the lesion to provide rapid relief from dysphagia with an additional radioactive source.54 This treatment, although rarely used, has proven long-term benefits, especially for patients with unresectable esophageal cancer.38 Ablative therapy, more useful after resection and for patients with Barrett esophagus, also can provide some relief but is associated with the need for more sessions compared with stent placement.38,55
Screening methodsAbout 60% of patients will have a concurrent diagnosis of Barrett esophagus and esophageal cancer, thus representing a gap in screening for Barrett esophagus.56 Screening in moderate- and high-risk populations is key to prevention and early diagnosis.25 Unfortunately, no single screening tool has proven to be cost-effective and accurate. Further, guidelines for screening from the American Society for Gastrointestinal Endoscopy are limited to patients with longstanding GERD and/or frequent reflux symptoms.25,57 The increasing prevalence of esophageal cancer will likely give rise to new screening techniques and procedures. Swallowable devices for sample collection, transnasal endoscopy, and breath testing are a few of the methods being introduced.20
CONCLUSIONAlthough the incidence of esophageal cancer in the United States is low, cases of esophageal adenocarcinoma are increasing rapidly.1 At the time of diagnosis, patients often have a poor prognosis and low 5-year survival rate. Screening methods are strongly encouraged, especially for those in high-risk populations with suspicious symptoms. A complete medical and social history, including questions tailored to esophageal cancer risk factors and dysphagia symptoms, will guide management. A bedside swallow test should be incorporated into the dysphagia evaluation. If endoscopy or GI consultation is delayed, the clinician can progress with imaging studies such as CT or PET/CT, keeping in mind their limitations. Although precision medicine is not ready to replace chemoradiation, clinicians should become familiar with targeted therapy and immunotherapy, which may lead to the elimination of more invasive procedures in the future. For patients who have survived cancer, an accurate record of their treatment can be managed by the primary care clinician with the incorporation of a survivorship plan into the EMR, thus improving continuity of care.
REFERENCES 1. Liu C-Q, Ma Y-L, Qin Q, et al. Epidemiology of esophageal cancer in 2020 and projections to 2030 and 2040. Thorac Cancer. 2023;14(1):3–11. 2. Abnet CC, Arnold M, Wei W-Q. Epidemiology of esophageal squamous cell carcinoma. Gastroenterology. 2018;154(2):360–373. 3. Grille VJ, Campbell S, Gibbs JF, Bauer TL. Esophageal cancer: the rise of adenocarcinoma over squamous cell carcinoma in the Asian belt. J Gastrointest Oncol. 2021;12(suppl 2):S339–S349. 4. Stabellini N, Chandar AK, Chak A, et al. Sex differences in esophageal cancer overall and by histological subtype. Sci Rep. 2022;12(1):5248. 5. American Cancer Society. Cancer facts and statistics. https://cancerstatisticscenter.cancer.org/#!/cancer-site/Esophagus. Accessed December 11, 2023. 6. Arnold M, Laversanne M, Brown LM, et al. Predicting the future burden of esophageal cancer by histological subtype: international trends in incidence up to 2030. Am J Gastroenterol. 2017;112(8):1247–1255. 7. American Cancer Society. Key statistics for esophageal cancer. www.cancer.org/cancer/types/esophagus-cancer/about/key-statistics.html. Accessed December 11, 2023. 8. Codipilly DC, Sawas T, Dhaliwal L, et al. Epidemiology and outcomes of young-onset esophageal adenocarcinoma: an analysis from a population-based database. Cancer Epidemiol Biomarkers Prev. 2021;30(1):142–149. 9. Ilson DH, van Hillegersberg R. Management of patients with adenocarcinoma or squamous cancer of the esophagus. Gastroenterology. 2018;154(2):437–451. 10. Lam AK. Introduction: esophageal squamous cell carcinoma—current status and future advances. In: Lam A, ed. Esophageal Squamous Cell Carcinoma. (Methods in Molecular Biology, 2129.) New York, NY: Humana Press; 2020. 11. Lach FP, Singh S, Rickman KA, et al. Esophageal cancer as initial presentation of Fanconi anemia in patients with a hypomorphic FANCA variant. Cold Spring Harb Mol Case Stud. 2020;6(6):a005595. 12. Ellis A, Risk JM, Maruthappu T, Kelsell DP. Tylosis with oesophageal cancer: diagnosis, management and molecular mechanisms. Orphanet J Rare Dis. 2015;10:126. 13. Spence AD, Busby J, Murchie P, et al. Medications that relax the lower oesophageal sphincter and risk of oesophageal cancer: an analysis of two independent population-based databases. Int J Cancer. 2018;143(1):22–31. 14. McCain RS, McManus DT, McQuaid S, et al. Alcohol intake, tobacco smoking, and esophageal adenocarcinoma survival: a molecular pathology epidemiology cohort study. Cancer Causes Control. 2020;31(1):1–11. 15. Polyzos SA, Zeglinas C, Artemaki F, et al. Helicobacter pylori infection and esophageal adenocarcinoma: a review and a personal view. Ann Gastroenterol. 2018;31(1):8–13. 16. American Cancer Society. Esophageal cancer risk factors. www.cancer.org/cancer/types/esophagus-cancer/causes-risks-prevention/risk-factors.html. Accessed January 2, 2024. 17. Short MW, Burgers KG, Fry VT. Esophageal cancer. Am Fam Physician. 2017;95(1):22–28. 18. Jansson-Knodell CL, Codipilly DC, Leggett CL. Making dysphagia easier to swallow: a review for the practicing clinician. Mayo Clin Proc. 2017;92(6):965–972. 19. Wilkinson JM, Codipilly DC, Wilfahrt RP. Dysphagia: evaluation and collaborative management. Am Fam Physician. 2021;103(2):97–106. 20. van der Vlugt M, Grobbee EJ, Bossuyt PM, et al. Risk of oral and upper gastrointestinal cancers in persons with positive results from a fecal immunochemical test in a colorectal cancer screening program. Clin Gastroenterol Hepatol. 2018;16(8):1237–1243.e2. 21. Ajani JA, D'Amico TA, Almhanna K, et al. Esophageal and esophagogastric junction cancers, version 1.2015. J Natl Compr Canc Netw. 2015;13(2):194–227. 22. Zhang H, Li H, Ma Q, et al. Predicting malignant transformation of esophageal squamous cell lesions by combined biomarkers in an endoscopic screening program. World J Gastroenterol. 2016;22(39):8770–8778. 23. Gress DM, Edge SB, Greene FL, et al. Principles of cancer staging. In: Amin MB, Edge SB, Greene FL, et al., eds. AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer; 2017:3–30. 24. Thota PN, Chak A. Is mass screening for Barrett's esophagus a myth or reality. Clin Gastroenterl Hepatol. 2019;17(4):610–612. 25. Joseph A, Raja S, Kamath S, et al. Esophageal adenocarcinoma: a dire need for early detection and treatment. Cleve Clin J Med. 2022;89(5):269–279. 26. Luo L-N, He L-J, Gao X-Y, et al. Evaluation of preoperative staging for esophageal squamous cell carcinoma. World J Gastroenterol. 2016;22(29):6683–6689. 27. Jayaprakasam VS, Yeh R, Ku GY, et al. Role of imaging in esophageal cancer management in 2020: update for radiologists. AJR Am J Roentgenol. 2020;215(5):1072–1084. 28. Elsherif SB, Andreou S, Virarkar M, et al. Role of precision imaging in esophageal cancer. J Thorac Dis. 2020;12(9):5159–5176. 29. Pellat A, Dohan A, Soyer P, et al. The role of magnetic resonance imaging in the management of esophageal cancer. Cancers. 2022;14(5):1141. 30. Lee SL, Yadav P, Starekova J, et al. Diagnostic performance of MRI for esophageal carcinoma: a systematic review and meta-analysis. Radiology. 2021;299(3):583–594. 31. Qumseya B, Sultan S, et al.ASGE Standards of Practice Committee ASGE guideline on screening and surveillance of Barrett's esophagus. Gastrointest Endosc. 2019;90(3):335–359.e2. 32. National Cancer Institute. Esophageal cancer treatment (PDQ)–health professional version. www.cancer.gov/types/esophageal/hp/esophageal-treatment-pdq#_212. Accessed January 2, 2024. 33. Haverkamp L, Seesing MF, Ruurda JP, et al. Worldwide trends in surgical techniques in the treatment of esophageal and gastroesophageal junction cancer. Dis Esophagus. 2017;30(1):1–7. 34. Sorscher S. Precision oncology comes of age. JAAPA. 2023;36(4):28–31. 35. Eyck BM, van Lanschot JJB, Hulshof MCCM, et al. Ten-year outcome of neoadjuvant chemoradiotherapy plus surgery for esophageal cancer: the randomized controlled CROSS trial. J Clin Oncol. 2021;39(18):1995–2004. 36. Wani S, Qumseya B, et al.Standards of Practice Committee Endoscopic eradication therapy for patients with Barrett's esophagus-associated dysplasia and intramucosal cancer. Gastrointest Endosc. 2018;87(4):907–931.e9. 37. He S, Xu J, Liu X, Zhen Y. Advances and challenges in the treatment of esophageal cancer. Acta Pharm Sin B. 2021;11(11):3379–3392. 38. van Rossum P, Mohammad N, Vleggaar F, van Hillegersberg R. Treatment for unresectable or metastatic oesophageal cancer: current evidence and trends. Nat Rev Gastroenterol Hepatol. 2018;15(4):235–249. doi:10.1038/nrgastro.2017.162. 39. Ashok A, Tiwari V, Jiwnani S, et al. Controversies in preoperative therapy in esophageal cancer: current evidence and ongoing research. Ann Gastroenterol Surg. 2019;3(6):592–597. 40. Guyer DL, Almhanna K, McKee KY. Palliative care for patients with esophageal cancer: a narrative review. Ann Transl Med. 2020;8(17):1103. 41. Balasubramanian BA, Higashi RT, Rodriguez SA, et al. Thematic analysis of challenges of care coordination for underinsured and uninsured cancer survivors with chronic conditions. JAMA Netw Open. 2021;4(8):e2119080. 42. Hoopes M, Voss R, Angier H, et al. Assessing cancer history accuracy in primary care electronic health records through cancer registry linkage. J Natl Cancer Inst. 2021;113(7):924–932. 43. American Cancer Society. ASCO cancer treatment and survivorship care plans. www.cancer.org/cancer/survivorship/long-term-health-concerns/survivorship-care-plans.html. Accessed January 2, 2024. 44. Dutta R, Vallurupalli M, McVeigh Q, et al. Understanding inequities in precision oncology diagnostics. Nat Cancer. 2023;4(6):787–794. 45. Sharma N. Recent advances in esophageal cancers go beyond a one-size-fits-all approach. www.targetedonc.com/view/recent-advances-in-esophageal-cancers-go-beyond-a-one-size-fits-all-approach. Accessed December 11, 2023. 46. Bang Y-J, Cutsem EV, Feyereislova A, et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet. 2010;376(9742):687–697. 47. Buzatto IP, Ribeiro-Silva A, Andrade JM, et al. Neoadjuvant chemotherapy with trastuzumab in HER2-positive breast cancer: pathologic complete response rate, predictive and prognostic factors. Braz J Med Biol Res. 2017;50(2):e5674. 48. Obermannová R, Alsina M, Cervantes A, et al. ESMO Guidelines Committee. Oesophageal cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2022;33(10):992–1004. 49. Cho JW, Choi SC, Jang JY, et al. Lymph node metastases in esophageal carcinoma: an endoscopist's view. Clin Endosc. 2014;47(6):523–529. 50. Nagaraja V, Eslick GD, Cox MR. Sentinel lymph node in oesophageal cancer—a systematic review and meta-analysis. J Gastrointest Oncol. 2014;5(2):127–141. 51. Takeuchi H, Kitagawa Y. Sentinel node navigation surgery in esophageal cancer. Ann Gastroenterol Surg. 2018;3(1):7–13. 52. Brancato V, Garbino N, Mannelli L, et al. Impact of radiogenomics in esophageal cancer on clinical outcomes: a pilot study. World J Gastroenterol. 2021;27(36):6110–6127. 53. Shui L, Ren H, Yang X, et al. The era of radiogenomics in precision medicine: an emerging approach to support diagnosis, treatment decisions, and prognostication in oncology. Front Oncol. 2021;10:570465. 54. Safaei AM, Ghalehtaki R, Khanjani N, et al. High-dose-rate intraluminal brachytherapy prior to external radiochemotherapy in locally advanced esophageal cancer: preliminary results. J Contemp Brachytherapy. 2017;9(1):30–35. 55. Sullivan R, Mulki R, Peter S. The role of ablation in the treatment of dysplastic Barrett's esophagus. Ther Adv Gastrointest Endosc. 2021;14:26317745211049967. 56. Tan MC, Mansour N, White DL, et al. Systematic review with meta-analysis: prevalence of prior and concurrent Barrett's oesophagus in oesophageal adenocarcinoma patients. Aliment Pharmacol Ther. 2020;52(1):20–36. 57. Bagaria B, Sood S, Sharma R, Lalwani S. Comparative study of CEA and CA19–9 in esophageal, gastric and colon cancers individually and in combination (ROC curve analysis). Cancer Biol Med. 2013;10(3):148–157.
留言 (0)